Keywords
Administration, Metronomic; Antineoplastic Protocols; Drug
Therapy, Combination; Immunotherapy; Pancreatic Neoplasms
Abbreviations
ALL acute lymphoblastic leukemia; CTL cytotoxic
T-cells; DC dendritic cells; GM-CSF granulocyte macrophage colonystimulating
factor; HA hyaluronan; IFN interferon alfa-2b; MTD
maximum tolerated dose; NaG: nab-paclitaxel and gemcitabine; NOLF
nab-paclitaxel, oxaliplatin, folinic acid and 5-fluorouracil; NK cells
natural killer cells; PaCT paclitaxel, cisplatin and oral trifluridine/
tipiracil; PaG paclitaxel and gemcitabine; PIC paclitaxel, irinotecan and
cisplatin; POLF paclitaxel, oxaliplatin, folinic acid and 5-fluorouracil;
Tregs regulatory T-cells
INTRODUCTION
Pancreatic cancer claims the lives of approximately
43,000 people each year and is the third leading cause
of cancer-related deaths in the United States. Metastatic
disease has an exceptionally poor prognosis, with a 5-year
survival of only 3%; the lowest of the cancers reported
by the American Cancer Society. Despite a declining
mortality rate for most other cancers, the mortality rate
for pancreatic cancer has increased in recent years, which
may be attributed to an increased disease incidence
and lack of new effective treatments for the disease [1].
Current trends suggest that pancreatic cancer will become
the second leading cause of cancer-related deaths in the
United States by 2030 [2]. Long term survival with nonresectable
metastatic pancreatic adenocarcinoma is rare
and there are only sparse case reports published showing
survival longer than 5 years. To our knowledge, this is
the first case report published in a reputable journal
of a patient with non-resectable metastatic pancreatic
adenocarcinoma who has survived for longer than 10 years. There are two standard treatment regimens
indicated for the treatment of metastatic pancreatic
cancer: nab-paclitaxel and gemcitabine, and FOLFIRINOX.
Median survival after diagnosis of metastatic disease,
even with standard treatment, is short in the order of 8.5
to 11.1 months [3, 4]. Pancreatic cancer’s poor prognosis
and lack of new therapy options highlight the need for
the development of better treatments for this devastating
disease. The following case report is of an 11 year survivor
of metastatic non-resectable pancreatic adenocarcinoma.
Her case is followed by the discussion of the treatment
strategy that contributed her exceptionally long survival.
CASE REPORT
The patient is currently a 74-year-old woman who
presented with an enlarged left supraclavicular lymph
node at the age of 63 in late 2006. The work-up and
diagnosis of this patient was made before the patient came
to our clinic for treatment. She underwent a biopsy of her
enlarged left supraclavicular lymph node in October 2006
which revealed an adenocarcinoma positive for two GI
tract restricted markers and negative for eight markers
for carcinomas primary to the lung, breast, and squamous
differentiation (Figure 1). The patient’s pathology was
most consistent with metastatic adenocarcinoma from
the upper GI tract. A CT scan performed after her biopsy
revealed peripancreatic retroperitoneal adenopathy at
the level of the pancreatic head, dilatation of the main
pancreatic duct, and secondary pancreatic duct, with
additional lesions in the lungs and the liver (Figure 2).
The scan findings combined with the pathology report
were felt to be most consistent with the diagnosis of
metastatic pancreatic adenocarcinoma. The patient
obtained two opinions, including one from the University
of Washington Medical Center, who all agreed that the
patient’s diagnosis was most consistent with metastatic pancreatic adenocarcinoma. Given her presentation with
non-resectable metastatic disease, it was felt at the time
that the patient should start treatment sooner rather than
later. Further work-up, such as a biopsy of the pancreatic
head, could not be justified due to the poor prognosis of
her disease and the possibility of complications that could
delay starting treatment.
Figure 1. Slides from original biopsy specimen. An analysis of the original biopsy specimen of the left supraclavicular lymph node in October 2006 revealed an adenocarcinoma. Immunohistochemistry showed two GI tract restricted markers, CDX-2 and villin. These markers indicated that the primary site of the metastatic adenocarcinoma was most likely in the upper GI tract, as the markers of carcinomas primary to the lung (TTF-1, surfactant apoA), breast (estrogen receptor, progesterone receptor, GCDFP-15, mammaglobin), and squamous differentiation (p63, CK5/6) were negative.
Figure 2. CT images from October 2006 showed (a). pancreatic ductal dilation, (b). peripancreatic retroperitoneal adenopathy at the level of the pancreatic head, (c). a segment 5 liver metastasis, (d). and a right upper lobe lung metastasis.
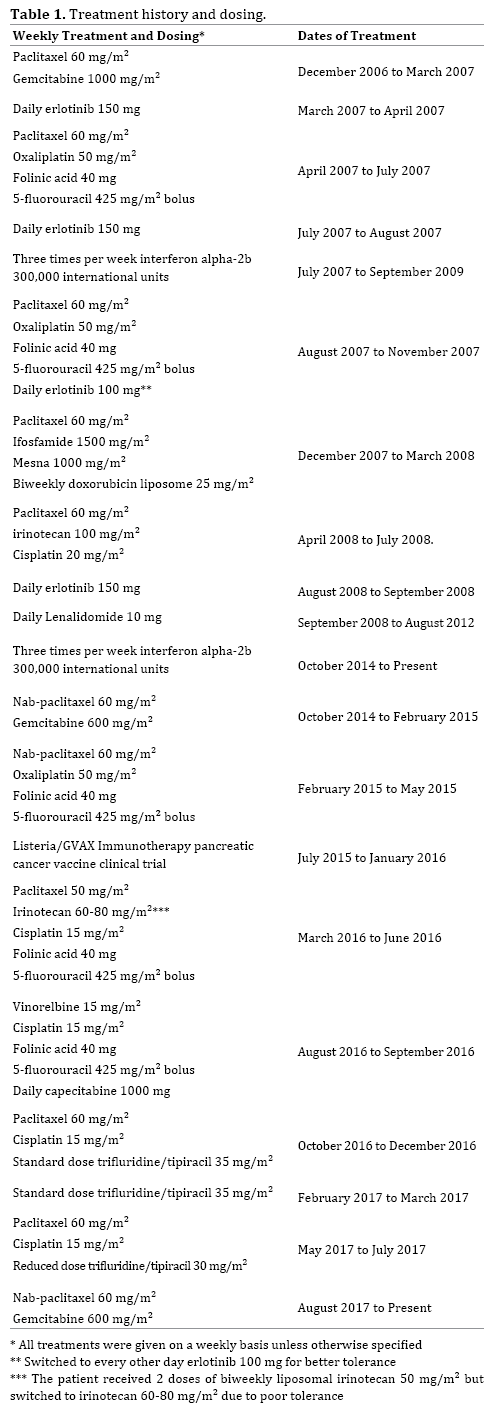
The patient started on weekly paclitaxel and
gemcitabine (PaG) in December 2006 (Table 1) with
a significant clinical reduction in the size of her left
supraclavicular lymph node. During this and all subsequent
treatments, the patient received granulocyte macrophage
colony-stimulating factor (GM-CSF) for chemotherapyinduced
neutropenia and immune stimulation. The patient
switched to daily erlotinib in March 2007 and continued
on erlotinib for one month until she restarted weekly
chemotherapy treatment with paclitaxel, oxaliplatin,
folinic acid and 5-fluorouracil (POLF). She continued
treatment with POLF until late-July 2007. A PET/CT
scan in July 2007 showed a substantial decrease in her
retroperitoneal adenopathy, significant improvement
in the hepatic metastatic lesions and shrinkage of
pulmonary nodules. The patient was switched back to
daily erlotinib in July 2007 and started on low-dose
interferon alfa-2b (IFN) for its immunostimulatory effects.
In August 2007, the patient restarted on weekly
chemotherapy treatment with POLF for an additional 3
months in combination with daily erlotinib. The patient
later switched to every other day erlotinib for better
tolerance. In December 2007, the patient changed
treatment to weekly paclitaxel, ifosfamide, mesna, and
bi-weekly doxorubicin liposome chemotherapy and
continued until mid-March 2008. Her treatment was then
switched in April 2008 to weekly paclitaxel, irinotecan,
and cisplatin (PIC) which she continued until mid-July
2008. A repeat CT scan of the chest, abdomen, and pelvis
in July 2008 showed an interval decrease in the size and
number of multiple liver metastases with the residual
lesions representing probable small liver cysts and a stable
right upper lobe pulmonary nodule with no new nodules
seen. The patient switched back to erlotinib and continued
this treatment until late-September 2008. The patient then
started on lenalidomide, an immunomodulatory drug for
maintenance therapy. A CT scan of the chest, abdomen, and
pelvis in October 2008 showed no evidence of recurrent or
persistent pancreatic cancer (Figure 3); although, there
were residual nodular infiltrates in the upper lobes of the
lungs thought to be the result of an infection. The lesions in
the liver were stable and most likely indicative of cysts. The
patient was considered to be in complete remission and
remained free of her disease for almost 6 years. A repeat
scan in October 2010 and a PET/CT scan from skull base to
mid-thigh in July 2011 showed no new pulmonary nodules,
no definite pancreatic mass, no new hepatic lesions and no
activity of progressive cancer. The patient discontinued
lenalidomide in late-August 2012 due to intolerance.
Figure 3. CT images from October 2008 showed (a). persistent pancreatic ductal dilation, (b). resolution of the previous peripancreatic retroperitoneal adenopathy, (c). resolution of the previous segment 5 liver metastasis, (d). and an improved right upper lobe lung metastasis.
Unfortunately, in October 2014 the patient was under
considerable stress and developed right abdominal discomfort. Blood work later revealed an elevated CA 19-9
of 322 (normal range: <37 units/mL). She underwent a
PET/CT scan in October 2014 which revealed multiple new
hypermetabolic liver lesions. A core liver biopsy showed
an adenocarcinoma consistent with a metastasis from the
patient’s original pancreatic primary.
The patient then restarted chemotherapy treatment
with weekly nab-paclitaxel and gemcitabine (NaG) along
with low-dose IFN in late-October 2014. The patient’s
disease responded to treatment with a drop in CA 19-9,
and a repeat CT scan in February 2015 showed a decrease
in the size of the patient’s hepatic metastases. The patient
switched treatments to weekly nab-paclitaxel, oxaliplatin,
folinic acid and 5-fluorouracil (NOLF) in February 2015
and continued this treatment for approximately 3 months.
A repeat CT scan in June 2015 showed stable disease,
and the patient’s CA 19-9 decreased to within normal range. The patient then enrolled in a phase 2B clinical
trial (NCT02004262) in early-July 2015 that investigated
if the efficacy of a GVAX pancreatic cancer vaccine given
with low-dose cyclophosphamide and live attenuated Listeria monocytogenes engineered to express mesothelin
in previously treated patients with a histologically proven
malignant adenocarcinoma of the pancreas. The patient
was in the treatment arm that received 6 doses of modified Listeria alone. She participated in this clinical trial until a
repeat CT scan in February 2016 revealed an increased
size and number of hepatic lesions. Corresponding blood
work showed her CA 19-9 had increased to 16,311.
The patient restarted chemotherapy treatment with
weekly paclitaxel, irinotecan, cisplatin, folinic acid, and
5-fluorouracil in March 2016 and continued treatment
until mid-June 2016. The patient originally started
treatment with paclitaxel, liposomal irinotecan, folinic acid and 5-fluorouracil but did not tolerate liposomal irinotecan
due to persistent nausea and vomiting and her liposomal
irinotecan was switched to irinotecan after two doses.
She then switched chemotherapy treatment to weekly
vinorelbine, cisplatin, folinic acid and 5-fluorouracil in
addition to daily low-dose capecitabine in mid-August
2016 and continued on this regimen until mid-September
2016. A CT scan in October 2016 showed overall stable
disease except for an interval increase in the size of one
liver lesion.
The patient then switched treatment to weekly
paclitaxel, cisplatin and oral trifluridine/tipiracil (PaCT)
in late-October, 2016 which she discontinued in late-
December 2016 due to severe diarrhea secondary to Clostridium difficile. Her CA 19-9 had decreased in response
to treatment and a repeat CT scan in January 2017 showed an
interval decrease in multiple hepatic lesions to approximately
one third of their previous size. After regaining strength from
her C. difficile infection, the patient resumed oral trifluridine/
tipiracil alone in early-February 2017. Weekly paclitaxel and
cisplatin were again added to the patient’s regimen in early-
May 2017. The patient then switched treatment back to NaG
in early-August 2017, which she continues on to try and
control her disease.
DISCUSSION
The patient’s case of metastatic non-resectable
pancreatic adenocarcinoma is one of remarkably long
survival. We believe this patient’s unusually long survival
is due to our treatment strategy which includes using
a weekly metronomic dosing of chemotherapy,
synergistic combinations of chemotherapy, switching
chemotherapy regimens before disease progression,
and using immune therapies. Two other patients treated
with a similar strategy, although they were not treated
exactly the same, also had survivals of over 5 years,
with one case previously described in detail [5, 6]. Our
strategy is as follows:
Metronomic Chemotherapy
Typically, a standard chemotherapy dosing
schedule calls for a maximum tolerated dose (MTD)
that is administered every 2 to 3 weeks. This break in
treatment is necessary to allow patients to recover from
acute toxicities associated with a MTD. In contrast, a
metronomic chemotherapy dosing schedule utilizes lower
doses of chemotherapy agents that are administered
more frequently, without any prolonged drug-free
breaks. Metronomic chemotherapy dosing allows for an
increased dose density, or, frequency of chemotherapy
administration. Dose-dense chemotherapy schedules
are often more tolerable and can increase the efficacy of
chemotherapy treatment [7, 8, 9, 10]. These chemotherapy
regimens follow in line with the Norton-Simon hypothesis
which suggests that tumor cell death is not maximized by
administering high doses of chemotherapy, but instead
by administering an effective dose of chemotherapy more
frequently [11].
A dose-dense chemotherapy regimen can also increase
dose-intensity, or, the total dose of chemotherapy
administered per unit time. For example, our POLF and
NOLF combinations use oxaliplatin at a dose of 50 mg/m²
once per week, and our PIC combination uses irinotecan
at a dose of 100 mg/m² once per week. In contrast, the
standard FOLFIRINOX regimen uses oxaliplatin at a dose
of 85 mg/m² and irinotecan at a dose of 180 mg/m² every
2 weeks. Therefore, our POLF/NOLF and PIC regimens
have an increased dose-intensity of oxaliplatin (100 mg/
m² vs. 85 mg/m²) and irinotecan (200 mg/m² vs. 180 mg/
m²) when compared to the FOLFIRINOX regimen, and may
consequently be more effective.
Although the dose-intensity of metronomic
chemotherapy regimens can be greater, they are
generally better tolerated as chemotherapy agents are
given at a lower dose during each administration. This
allows for better continuation of treatment without
interruptions due to intolerable side-effects. For example,
the FOLFIRINOX regimen is known to cause harsh sideeffects
which can result in lapses in treatment. The poor
tolerability of FOLFIRINOX results in a poorer quality of
life for patients, and breaks in treatment can also allow
for tumor cells to proliferate and mutate, resulting in
disease progression. In contrast, the patient’s weekly
metronomic chemotherapy regimens were generally
well tolerated with the usual side effects associated
with the chemotherapy agents involved, although all
side effects were decreased in severity. The patient had
an average ECOG score ranging between 1-2 throughout
her treatment, which allowed her to continue treatment
for the majority of each planned treatment cycle in
addition to maintaining a good quality of life.
The primary mechanism of action of metronomic
chemotherapy is thought to be its ability to enhance the
antiangiogenic properties of certain chemotherapy agents
[12]. In particular, there is preclinical evidence suggesting
that paclitaxel and nab-paclitaxel have antiangiogenic
effects when administered in low doses [13, 14, 15].
The increased vascularity of a tumor can decrease the
effectiveness of chemotherapy delivery by diverting
chemotherapy agents away from the tumor bed [16, 17].
By blocking angiogenesis, more chemotherapy may reach
the tumor bed, thereby improving the efficacy of the
cytotoxic chemotherapy agents. This is a major reason why
paclitaxel and nab-paclitaxel were used in the majority of
the patient’s treatment regimens.
In pancreatic cancer, another mechanism may
also impair drug delivery in addition to, or in place of,
angiogenesis. Stromal layers composed of hyaluronan
(HA) are commonly found surrounding pancreatic cancers
and are thought to decrease intratumoral chemotherapy
delivery [18, 19]. In a recent clinical trial, the survival of
patients expressing high levels of tissue HA improved
when PEGPH20, a hyaluronidase, was administered with
chemotherapy [20]. This finding highlights the importance
of including an anti-stromal agent in a chemotherapy regimen when treating pancreatic cancer. Nab-paclitaxel
has also been shown to decrease cancer-associated
fibroblasts, which are thought to contribute to and promote
the formation of the stromal layer [21, 22]. Paclitaxel may
also have a similar effect since the patient responded to
treatment when paclitaxel or nab-paclitaxel was used in
her chemotherapy treatment regimens.
Combination Chemotherapy
A combination approach can be more effective
than a single-agent therapy due to synergy between
treatment agents. For example, the combination of nabpaclitaxel
and gemcitabine has been shown to improve
overall survival versus gemcitabine alone [3]. An ideal
combination chemotherapy regimen is one where the
chemotherapy agents are synergistic in efficacy against
the disease while not being overly additive in their sideeffects.
When one examines the side-effect profiles of the
agents within the patient’s regimens, one can see that the
major potential side effects of each agent generally differs
from the other agents in each regimen. For example, the
POLF regimen followed by the PIC regimen contains
similar agents as in the FOLFIRINOX regimen; however,
the main agents causing diarrhea (5-fluorouracil and
irinotecan) and neutropenia (oxaliplatin and irinotecan)
are kept separate between the POLF and PIC regimens.
This method of selecting chemotherapy agents allows for
better tolerability which in turn allows for more consistent
and continuous treatment.
Sequential Therapy
Currently, the standard treatment protocol for
metastatic pancreatic cancer generally involves continuing
treatment until there is obvious disease progression. Drug
resistance in tumor cells is seen as the primary cause
of failure of chemotherapy treatment for cancer. The
Goldie-Coldman hypothesis suggests that drug resistance
mutations develop spontaneously over time, which can
result in the selection of drug-resistant populations of
cancer cells with treatment. Thus, the probability of a tumor
cell developing resistance to a single chemotherapeutic
agent increases in a short period of time [23]. The rationale
behind sequential chemotherapy regimens is to decrease
the chance of drug resistance and maximize efficacy of the
treatment.
The idea of sequential therapy has been introduced
successfully in maintenance therapy in advanced non-small
cell lung carcinoma [24]. Sequential therapy has also found
major success in acute lymphoblastic leukemia (ALL). A
diagnosis of ALL was fatal for children in the 1950s. Today,
this disease has a cure rate of more than 80 percent in
children. The current clinical treatment for ALL involves
sequential combination chemotherapy regimens in the
remission-induction phase, intensification or consolidation
phase, and maintenance phase. The treatment results from
ALL have been considered one of the greatest achievements
in oncology to this date [25]. In this case, chemotherapy
regimens were purposely switched before obvious disease progression due to the concern of cancer cell resistance and
to prevent the accumulation of chemotoxicity to a single
chemotherapy regimen, approximately every 12 weeks (Table 1). Continuing chemotherapy and implementing
sequential therapy may be more effective at reducing the
total number of cancer cells over time, therefore allowing
for optimal disease control [26].
Immunotherapy
The immune system is thought to play a major role
in the treatment of pancreatic cancer. However, immune
suppression from regulatory T-cells (Tregs) and the
secretion of immunosuppressive factors in the tumor
microenvironment can inhibit cytotoxic T-cells (CTL),
natural killer cells (NK cells) and dendritic cells (DC) that
are crucial to the body’s anti-tumor immune response [27].
The metronomic dosing of chemotherapy may decrease
immunosuppressive cells, such as Tregs, allowing for an
anti-tumor immune response [28, 29]. Using lower doses
of chemotherapy also generally results in a less profound
drop in blood counts, which allows for the preservation
of the immune system. Moreover, aberrant blood vessels
from angiogenesis may serve as a protective mechanism,
diverting immune cells away from the tumor bed. The
metronomic dosing of chemotherapy can also normalize
aberrant blood vessels caused by angiogenesis and thus
allow the immune system to better reach the tumor bed.
In addition to the possible immunostimulatory effects of
metronomic chemotherapy, the patient received 3 other
immunostimulatory agents.
To stimulate the immune system and prevent
neutropenia, 250-500 mcg of GM-CSF was administered
intradermally and subcutaneously 2 to 5 times per week
during the patient’s treatment. Typically GM-CSF is
only administered subcutaneously, but the intradermal
route of administration was also used because of the
abundance of DCs found in the intradermal area. This
immunostimulatory agent has been shown to produce the
most potent anti-tumor immune response in comparison to
other immunostimulatory agents such as interleukins and
interferon gamma [30]. GM-CSF’s anti-tumor properties
have also been used to enhance potential vaccines for
several cancers, including pancreatic cancer [31].
To further stimulate the patient’s immune system,
300,000 international units of IFN was injected
intradermally 3 times per week. Typically, IFN is not
tolerated well, but the patient had no side effects
secondary to this medication likely due to its low dose. IFN
has known anti-tumor properties and has shown efficacy
in the treatment of several types of cancer [32]. IFN’s antitumor
properties may be related to its ability to stimulate
DCs and NK cells. CTL cell stimulation is also thought to
occur indirectly by the abolishment of tolerogenic DCs
which prevents the induction of Tregs [33].
Lenalidomide was also used in the treatment of this
patient as maintenance therapy post-chemotherapy
treatment, which may have played a role in her 6 year period of remission. This drug has been used in the treatment
of multiple myeloma and has antiangiogenic effects and
immunomodulatory properties, such as stimulating CTLs
and NK cells. Lenalidomide has also been shown to have
anti-tumor effects in some solid tumors such as renal
cell carcinoma [34]. The anti-tumor and antiangiogenic
properties of this drug may be more efficacious in patients
with minimal tumor burden.
CONCLUSION
We believe that weekly metronomic chemotherapy,
combination chemotherapy, sequential therapy and the
incorporation of immune therapies in this patient’s case
each contributed to her long-term survival. We hope that
this case report helps provide a roadmap for treatment
of this devastating disease and perhaps a framework for
the treatment of other types of cancers. Given that most
patients with metastatic pancreatic cancer are given a
prognosis on the order of months, the enduring survival of this
patient of 11 years can provide a ray of hope for others with
this disease. The treatment strategy used in this patient’s case
should be further researched due to the potential significant
medical, psychological, and economic implications.
Acknowledgements
We would like to thank Dr. Udo Schmiedl, M.D. Ph.D, Dr.
Kathrin Ahl, M.D., and Dr. Kristin Manning, M.D., for their
help with analyzing CT scan images, Dr. Jennifer LaPoint,
M.D., for her help providing pathology slides, Matti
Niemisto and Kin Lai for drafting earlier versions of this
paper, and Chi Rho, without whom none of this work could
have been done.
Funding
No source of funding was used to conduct this research
or write this case report.
Conflicts of Interest
The authors have declared that no conflicts of interest
exist.
Informed Consent
Informed consent was obtained from the patient
in the study for publication of this case report and any
accompanying images. A copy of the written consent is
available for review upon request.
References
- Siegel RL, Miller KD, Jemal A. Cancer Statistics, 2017. CA Cancer J Clin 2017;67:7-30. [PMID: 28055103].
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014; 74:2913-21. [PMID: 24840647].
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369:1691-703. [PMID: 24131140].
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364:1817-25. [PMID: 21561347].
- Chue BM. Five-year survival of metastatic pancreatic carcinoma: a study of courage and hope. Gastrointest Cancer Res 2009; 3:208-11. [PMID: 20084164].
- Shigihara M and Erickson K. Living Lessons. El Segundo, CA: Active Interest Media, 2010.
- Katsumata N, Yasuda M, Isonishi S, Takahashi F, Michimae H, Kimura E, et al. Long-term results of dose-dense paclitaxel and carboplatin versus conventional paclitaxel and carboplatin for treatment of advanced epithelial ovarian, fallopian tube, or primary peritoneal cancer (JGOG 3016): a randomised, controlled, open-label trial. Lancet Oncol 2013; 14:1020-6. [PMID: 23948349].
- Citron ML, Berry DA, Cirrincione C, Hudis C, Winer EP, Gradishar WJ, et al. Randomized trial of dose-dense versus conventionally scheduled and sequential versus concurrent combination chemotherapy as postoperative adjuvant treatment of node-positive primary breast cancer: first report of Intergroup Trial C9741/Cancer and Leukemia Group B Trial 9741. J Clin Oncol 2003; 21:1431-9. [PMID: 12668651].
- Citron ML. Dose-Dense Chemotherapy: Principles, Clinical Results and Future Perspectives. Breast Care (Basel) 2008; 3:251-255. [PMID: 21076605].
- Fornier M, Norton L. Dose-dense adjuvant chemotherapy for primary breast cancer. Breast Cancer Res 2005; 7:64-9. [PMID: 15743513].
- Simon R, Norton L. The Norton-Simon hypothesis: designing more effective and less toxic chemotherapeutic regimens. Nat Clin Pract Oncol 2006; 3:406-7. [PMID: 16894366].
- Kerbel RS, Kamen BA. The anti-angiogenic basis of metronomic chemotherapy. Nat Rev Cancer 2004; 4:423-36. [PMID: 15170445].
- Belotti D, Vergani V, Drudis T, Borsotti P, Pitelli MR, Viale G, et al. The microtubule-affecting drug paclitaxel has antiangiogenic activity. Clin Cancer Res 1996; 2:1843-9. [PMID: 9816139].
- Wang J, Lou P, Lesniewski R, Henkin J. Paclitaxel at ultra-low concentrations inhibits angiogenesis without affecting cellular microtubule assembly. Anticancer Drugs 2003; 14:13-9. [PMID: 12544254].
- Bocci G, Di Paolo A, Danesi R. The pharmacological bases of the antiangiogenic activity of paclitaxel. Angiogenesis 2013; 16:481-92. [PMID: 23389639].
- Tong RT, Boucher Y, Kozin SV, Winkler F, Hicklin DJ, Jain RK, et al. Vascular normalization by vascular endothelial growth factor receptor 2 blockade induces a pressure gradient across the vasculature and improves drug penetration in tumors. Cancer Res 2004; 64:3731-6. [PMID: 15172975].
- Goel S, Duda DG, Xu L, Munn LL, Boucher Y, Fukumura D, et al. Normalization of the vasculature for treatment of cancer and other diseases. Physiol Rev 2011; 91:1071-121. [PMID: 21742796].
- Provenzano PP, Cuevas C, Chang AE, Goel VK, Von Hoff DD, Hingorani SR. Enzymatic targeting of the stroma ablates physical barriers to treatment of pancreatic ductal adenocarcinoma. Cancer Cell 2012; 21:418-29. [PMID: 22439937].
- Jacobetz MA, Chan DS, Neesse A, Bapiro TE, Cook N, Frese KK, et al. Hyaluronan impairs vascular function and drug delivery in a mouse model of pancreatic cancer. Gut 2013; 62:112-20. [PMID: 22466618].
- Hingorani SR, Harris WP, Beck JT, Berdov BA, Wagner SA, Pshevlotsky EM, et al. Phase Ib Study of PEGylated Recombinant Human Hyaluronidase and Gemcitabine in Patients with Advanced Pancreatic Cancer. Clin Cancer Res 2016; 22:2848-54. [PMID: 26813359].
- Sato N, Maehara N, Goggins M. Gene expression profiling of tumor-stromal interactions between pancreatic cancer cells and stromal fibroblasts. Cancer Res 2004; 64:6950-6. [PMID: 15466186].
- Alvarez R, Musteanu M, Garcia-Garcia E, Lopez-Casas PP, Megias D, Guerra C, et al. Stromal disrupting effects of nab-paclitaxel in pancreatic cancer. Br J Cancer 2013; 109:926-33. [PMID: 23907428].
- Goldie JH, Coldman AJ. A mathematic model for relating the drug sensitivity of tumors to their spontaneous mutation rate. Cancer Treat Rep 1979; 63:1727-33. [PMID: 526911].
- Gentzler RD, Patel JD. Maintenance treatment after induction therapy in non-small cell lung cancer: latest evidence and clinical implications. TherAdv Med Oncol 2014; 6:4-15. [PMID: 24381656].
- Pui CH, Robison LL, Look AT. Acute lymphoblastic leukaemia. Lancet 2008; 371:1030-43. [PMID: 18358930].
- Chue BM. Long-Term Survival in Metastatic Pancreatic Adenocarcinoma and Cholangiocarcinoma Can Be Achieved With “Metronomic Dosing” of Paclitaxel/Oxaliplatin/Leucovorin/5-Fluorouracil (POLF) and Possibly Other Chemotherapy Regimens. Gastrointestinal Cancer Research 2010; (Suppl 2):S7-S9.
- Sideras K, Braat H, Kwekkeboom J, van Eijck CH, Peppelenbosch MP, Sleijfer S, et al. Role of the immune system in pancreatic cancer progression and immune modulating treatment strategies. Cancer Treat Rev 2014; 40:513-22. [PMID: 24315741].
- Tongu M, Harashima N, Monma H, Inao T, Yamada T, Kawauchi H, et al. Metronomic chemotherapy with low-dose cyclophosphamide plus gemcitabine can induce anti-tumor T cell immunity in vivo. Cancer ImmunolImmunother 2013; 62:383-91. [PMID: 22926062].
- Nars MS, Kaneno R. Immunomodulatory effects of low dose chemotherapy and perspectives of its combination with immunotherapy. Int J Cancer 2013; 132:2471-8. [PMID: 22927096].
- Dranoff G, Jaffee E, Lazenby A, Golumbek P, Levitsky H, Brose K, et al. Vaccination with irradiated tumor cells engineered to secrete murine granulocyte-macrophage colony-stimulating factor stimulates potent, specific, and long-lasting anti-tumor immunity. Proc Natl Acad Sci U S A 1993; 90:3539-43. [PMID: 8097319].
- Le DT, Wang-Gillam A, Picozzi V, Greten TF, Crocenzi T, Springett G, et al. Safety and survival with GVAX pancreas prime and Listeria Monocytogenes-expressing mesothelin (CRS-207) boost vaccines for metastatic pancreatic cancer. J Clin Oncol 2015; 33:1325-33. [PMID: 25584002].
- Jonasch E, Haluska FG. Interferon in oncological practice: review of interferon biology, clinical applications, and toxicities. Oncologist 2001; 6:34-55. [PMID: 11161227].
- Bacher N, Graulich E, Jonuleit H, Grabbe S, Steinbrink K. Interferon-α abrogates tolerance induction by human tolerogenic dendritic cells. PLoS One 2011; 6:e22763. [PMID: 21818385].
- Segler A, Tsimberidou AM. Lenalidomide in solid tumors. Cancer Chemother Pharmacol 2012; 69:1393-406. [PMID: 22584909].




