Keywords
Pancreatic Neoplasms; Prognosis; Secretoglobins
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) is the
fourth most common cause of cancer death in the Western
world [1]. The prognosis is poor, with 1- and 5-year survival
rates of only 20% and 6%, respectively [2]. Early diagnosis
of PDAC is difficult, and there are no blood biomarkers to
identify patients with pancreatic cancer at an early stage
[3]. Therefore, new insights into the biology and genetics of
PDAC are required to identify novel markers for diagnosis
and prognosis prediction, and the development of targeted
therapies.
SCGB1D2 (Secretoglobin, Family 1D, Member 2), also
termed lipophilin B, is a member of the secretoglobin
(SCGB) supergene family [4]. Secretoglobins are secreted proteins of small molecular weight belonging
to a polypeptide family that includes at least nine family
members in humans [5, 6]. Although the first SCGB
polypeptide, uteroglobin (SCGB1A1), was discovered
more than 30 years ago, the pathophysiological functions
of the family are still poorly understood. SCGB1D2 is
generally located in secretory epithelia such as that found in
breast tissue [7], and its dysregulated expression has been
reported in several malignancies, including breast [8] and
gynecological cancers [9]. We recently reported that insulinlike
growth factor-2 mRNA-binding protein 3 (IGF2BP3), can
bind to ADP-ribosylation factor 6 (ARF6) and Rho guanine
nucleotide exchange factor 4 (ARHGEF4) messenger RNAs
(mRNAs), leading to their accumulation in the cell protrusions
of PDAC cells [10]. In turn, these locally translated proteins
influence the formation of additional membrane protrusions
and thereby increase the motility and invasiveness of PDAC
tumors [10, 11]. Since IGF2BP3 also binds SCGB1D2 mRNA
[10], these findings suggest that SCGB1D2 translated within
cell protrusions may also be associated with cell invasion and
metastasis. However, little is known about the relationship
of SCGB1D2 expression in regard to clinicopathological
parameters and prognosis in PDAC patients.
In this study, we analyzed the expression of the
SCGB1D2 protein in human PDAC tissues using
immunohistochemistry and immunocytochemistry,
and evaluated the relationship of SCGB1D2 expression
with corresponding clinicopathological parameters and
patient prognosis. SCGB1D2 was found to accumulate in
cell membrane protrusions, indicating that this protein
plays an important role in their formation. Importantly,
our results suggest that high expression of SCGB1D2 is a
reliable indicator for poor prognosis in PDAC patients.
METHODS
Primary Human PDAC Samples
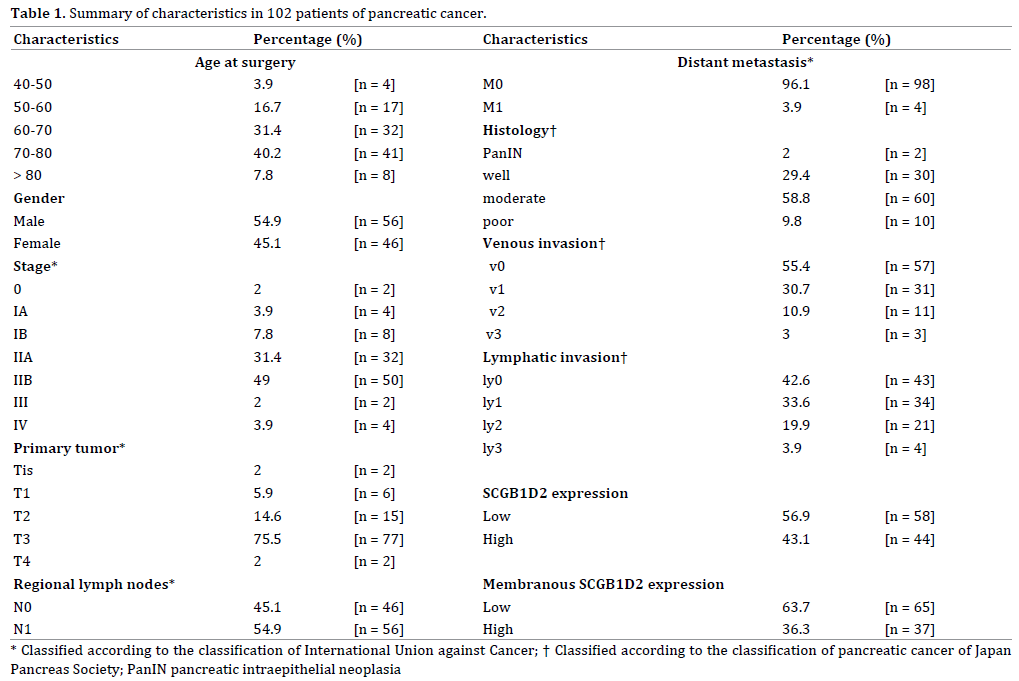
Patients (n = 102) who underwent surgical treatment
for PDAC at the Departments of Surgery, Kochi Medical
School Hospital (Nankoku, Japan) and Matsuyama Shimin
Hospital (Matsuyama, Japan) between 1999 and 2014 were
studied (clinicopathological findings of these 102 patients
are summarized in Table 1), as published previously [12].
The follow-up period for survivors ranged from 18 to 192
months (median 64.0). Of these patients, 83 had received
adjuvant chemotherapy with gemcitabine or S-1 (tegafur/
gimeracil/oteracil), or chemoradiation therapy after
resection. Pancreatic carcinomas were classified according
to the Japan Pancreas Society [13] and the Union for
International Cancer Control (UICC) TNM staging notation
[14]. Immunohistochemical analysis of PDAC samples was
approved by the ethical review boards of Kochi Medical
School and Matsuyama Shimin Hospital prior to patient recruitment, and was carried out in accordance with the
approved guidelines. Informed consent was obtained from
each patient.
Immunohistochemical Staining
Immunohistochemistry was carried out, as published
previously [12]. Tissue sections from normal pancreas,
brain, lung, liver and kidney were purchased from
Biochain (Hayward, CA). The sections were deparaffinized
and autoclaved at 108°C for 15 min. After endogenous
peroxidase activity was quenched by incubation for 30
min in 0.33% hydrogen peroxide diluted in methanol,
the sections were incubated with fetal bovine serum for
blocking. Sections were then incubated with anti-SCGB1D2
antibody (sc-48327; Santa Cruz Biotechnology, Santa
Cruz, CA) at room temperature for 1 h and washed with
PBS. Immunodetection was performed with peroxidaselabeled
anti-rabbit immunoglobulin (DakoCytomation,
Carpinteria, CA). Finally, the reactants were developed
with 3,3’-diaminobenzidine (Dako), and the sections were
counterstained with hematoxylin.
Evaluation of SCGB1D2 Staining
Staining was evaluated by one researcher (KT) with two
independent observers (SN and MF), who were blinded
to the clinical and outcome data, as published previously
[12]. Immunoreactivity was scored semi-quantitatively
according to the estimated percentage of positive tumor
cells (1, <50% reacting cells; 2, 50% to 80% reacting
cells; 3, >80% reacting cells) and the staining intensity (1, weaker than the intensity of staining on the surface of the
islets of Langerhans; 2, equal to the intensity of staining
of the islets of Langerhans; 3, stronger than the intensity
of staining of the islets of Langerhans). Slides on which
the islets of Langerhans did not stain significantly were
considered to be in bad condition and were not evaluated.
A total immunohistochemical score was calculated by
summing the percentage score and the intensity score.
The level of SCGB1D2 expression was classified into two
groups according to the total score (score of 2-3, lowexpressing
group; score of 4-6, high-expressing group).
In addition, the distribution of SCGB1D2 expression
in PDAC tissues was recorded as negative (0), weak
cytoplasmic positivity in any proportion of cells (1),
moderate cytoplasmic positivity in any proportion of cells
(2), distinct membranous positivity in ≤ 50% of cells (3),
and distinct membranous positivity in >50% of cells (4) as
previously described [15, 16]. The level of membranous
SCGB1D2 expression was then classified into two groups
according to the total score (membranous score of 0-2,
low-expressing group; membranous score of 3-4, highexpressing
group).
Cell Culture
The human PDAC cell line S2-013, a subline of SUIT-
2, was obtained from Dr. T. Iwamura (Miyazaki Medical
College, Miyazaki, Japan) [17]. The human PDAC cell line
PANC-1 was purchased from the American Type Culture
Collection (ATCC; Manassas, VA). All cells were grown in
Dulbecco’s modified Eagle’s medium (DMEM; Gibco-BRL,
Carlsbad, CA) supplemented with 10% heat-inactivated
fetal calf serum at 37°C in a humidified atmosphere
saturated with 5% CO2.
Immunocytochemistry Analysis by Confocal
Immunofluorescence Microscopy
Immunocytochemistry was carried out, as published
previously [12]. Coverslips were coated with 10 μg/mL
fibronectin (Sigma-Aldrich, St. Louis, MO) for 1 h at room
temperature. Cells were seeded on fibronectin-coated
glass coverslips and incubated for 5 h. The cells were then
fixed with 4% paraformaldehyde, permeabilized with
0.1% Triton X-100, covered with blocking solution (3%
BSA/PBS), and then incubated with the primary antibody
for 1 h. Alexa488- or Alexa594-conjugated secondary
antibody (Molecular Probes, Carlsbad, CA) was then
applied with Alexa594- or Alexa594-conjugated phalloidin
(Cytoskeleton, Denver, CO). Each specimen was visualized
using a Zeiss LSM 510 META confocal microscope (Carl
Zeiss, Gottingen, Germany).
Small Interfering RNA Treatment
Individual mixtures of four different small interfering
RNA (siRNA) oligonucleotides (oligos) targeting SCGB1D2 were purchased from Qiagen (FlexiTube GeneSolution
siRNA GS10647; Valencia, CA), and individual mixtures
of four different scrambled negative control siRNA oligos
were obtained from Santa Cruz (37007). To examine
the effect of the siRNAs on SCGB1D2 expression, S2-013 and PANC-1 cells were plated in six-well plates, and
transfected 20 h later with 80 pmol of the relevant siRNA
mixture in siRNA transfection reagent (Qiagen) following
the manufacturer's instructions. After incubation for 48
h, the cells were processed for Western blotting or for
immunocytochemistry analysis.
SCGB1D2-rescue Construct
Reverse transcription-PCR (RT-PCR) was used to
amplify the entire coding sequence of the SCGB1D2 cDNA.
The resultant PCR product was subsequently inserted into
a pCMV6-Entry vector (Origene Technologies, Rockville,
MD) bearing a C-terminal myc-DDK-tag. The X-tremeGENE
HP DNA Transfection Reagent (Roche, Penzberg, Germany)
was used to transiently transfect target cells with the
resultant SCGB1D2-rescue construct. After incubation for 48
h, the cell pellet was resuspended in lysis buffer containing
20 mM HEPES (pH 7.4), 100 mM KCl, 2 mM MgCl2, 0.5%
Triton X-100, protease inhibitor cocktail tablets (Roche),
and phosphatase inhibitor cocktail (Nacalai, Kyoto, Japan).
The bicinchoninic acid (BCA) assay was used to determine
the protein concentration of each lysate, and an aliquot of
each lysate was then diluted with sample buffer (50 mM
Tris, 2% sodium lauryl sulfate (SDS), 0.1% bromophenol
blue, and 10% glycerol) to a final concentration of 1-2 μg/
μL and analyzed by SDS-polyacrylamide gel electrophoresis
and Western blotting using anti-SCGB1D2 (sc-48327;
Santa Cruz Biotechnology) and anti-myc (sc-789; Santa
Cruz Biotechnology) antibodies.
Statistical Analysis
Statistical analysis was carried out, as published
previously [12]. StatFlex software (Ver. 6; YUMIT, Osaka,
Japan) and SAS software (Ver. 9.1.3; SAS Institute, Cary,
NC) were used for statistical analysis. Student’s t-test was
used for the comparison of continuous variables. Fisher's
exact test was used to assess the association between
SCGB1D2 expression levels and clinicopathological
parameters. The following parameters were examined:
age, sex, and the TNM classification or pathological stage,
based on the Japan Pancreas Society [13] and UICC [14]
scoring systems. Overall survival time was measured
from the date of surgery to the date of death (due to any
cause) or the last clinical follow-up, as determined by
review of electronic medical records. Survival curves were
plotted using the Kaplan-Meier method and compared
using the log-rank test (Mantel-Cox). Survival rates are
expressed as the median value and interquartile range
(IQR). Independent factors, including age, sex, and the
pathological stage for overall survival, were assessed with
Cox proportional hazards regression analysis. P values
<0.05 were considered to be statistically significant, and
all tests were two-tailed.
RESULTS
SCGB1D2 Expression in Human PDAC Tissues
We examined SCGB1D2 expression in surgical specimens
from 102 patients with PDAC by immunohistochemical analysis. A histoscore method [12, 18], which takes into
account both the extent of expression and the staining
intensity of SCGB1D2, was employed. Expression levels of
SCGB1D2 were evaluable in all 102 cases, and these cases
were classified into low-expressing (56.9%, n = 58; total
immunohistochemical score, 2-3) and high-expressing
(43.1%, n = 44; total immunohistochemical score, 4-6)
SCGB1D2 groups (Table 1). SCGB1D2 was localized to
both the cytoplasm of PDAC cells (Figure 1a), and their
cell membranes (Figure 1b). High levels of membranous
SCGB1D2 (i.e. a membranous immunohistochemical score
of 3-4) were found in 36.3% (n = 37) of patients (Table 1). There was no obvious staining with the SCGB1D2
antibody in the pancreatic ducts of normal pancreas, or
in normal samples of brain, lung, liver and kidney (Figure
1c). The expression levels of intracellular SCGB1D2 and
membranous SCGB1D2 were not different in the central
region and the penumbra of the PDAC tumor.
Figure 1. SCGB1D2 expression in resected PDAC tissues.
(a). Immunohistochemical staining of PDAC tissues with anti-SCGB1D2, showing that SCGB1D2 is present in the cytoplasm of tumor cells (magnification 200×).
Scale bar, 50 μm. (b). Immunohistochemical staining of PDAC tissues with anti-SCGB1D2, showing membrane staining of SCGB1D2 in tumor cells (magnification
200×). Scale bar, 50 μm. (c). Expression of SCGB1D2 in normal pancreas, brain, lung, liver and kidney (magnification 200×). Scale bars, 50 μm.
Association Between SCGB1D2 Expression,
Clinicopathology, and Overall Survival
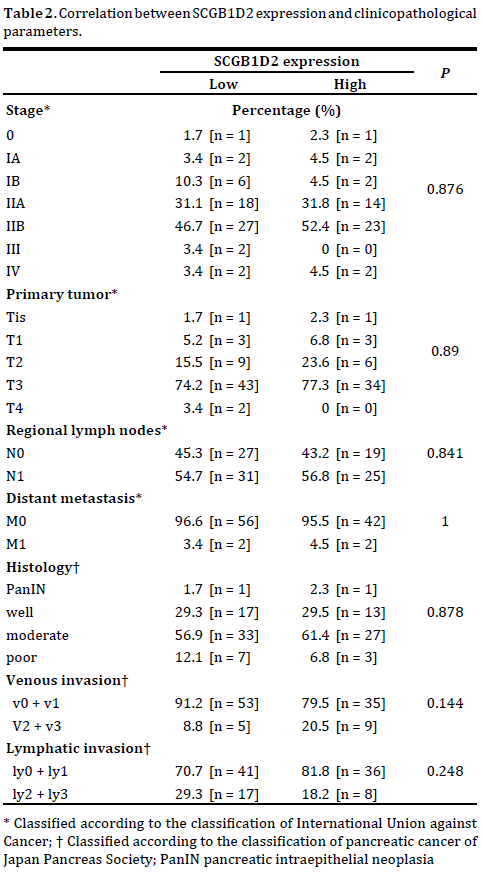
We next analyzed the relationship between SCGB1D2
expression and clinicopathological features as shown in Table 2, however there was no significant correlation found between overall expression score and the
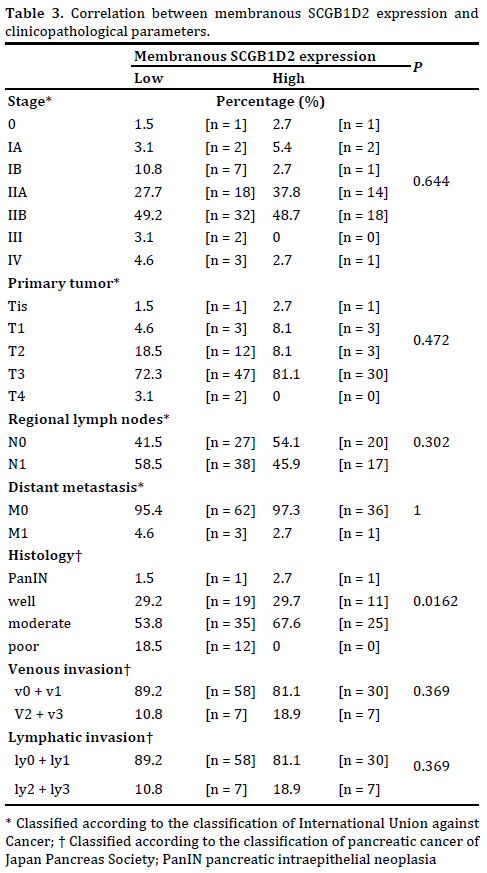
clinicopathological features examined. Membranous
SCGB1D2 expression was associated with histology
grade, but there was no significant correlation between
high-expressing membranous SCGB1D2 and other
clinicopathological features (Table 3).
The follow-up period for survivors of the 102 PDAC
patients ranged from 18 to 192 months (median 64.0).
Median survival time was 26 months (95% confidence
interval [CI], 23-33), the 3-year survival rate was 35.1%
(95%CI, 25.6-44.8), and the 5-year survival rate was 25.9%
(95%CI, 17.2-35.5). Kaplan-Meier plots showed there was
a significant difference in overall survival rate (P = 0.007)
between groups with high and low SCGB1D2 expression
(Figures 2a, 2b), but not between groups with high and low
membranous SCGB1D2 expression (P = 0.583; Figure 2c).
Figure 2. Association of SCGB1D2 expression with poor outcome in PDAC patients.
(a). Kaplan-Meier analysis of PDAC-specific survival and (b). overall survival according to SCGB1D2 expression. (c). Kaplan-Meier analysis of overall
survival rates in patients with high and low membranous SCGB1D2 expression. Scale bars, 10 μm.
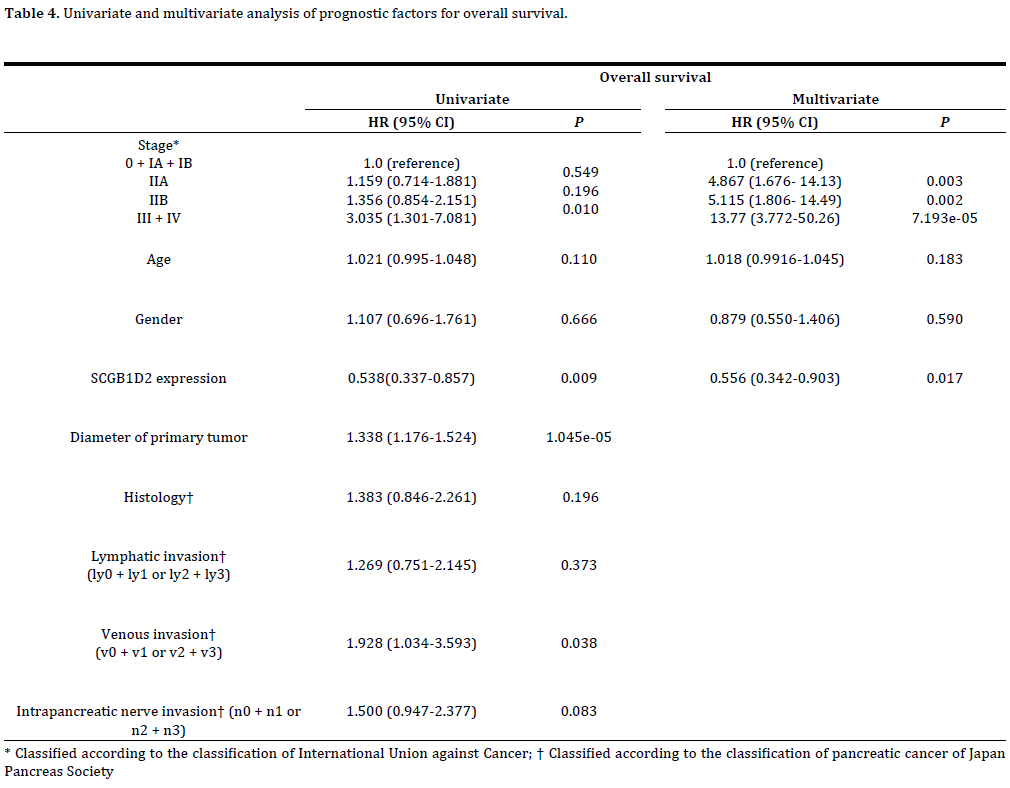
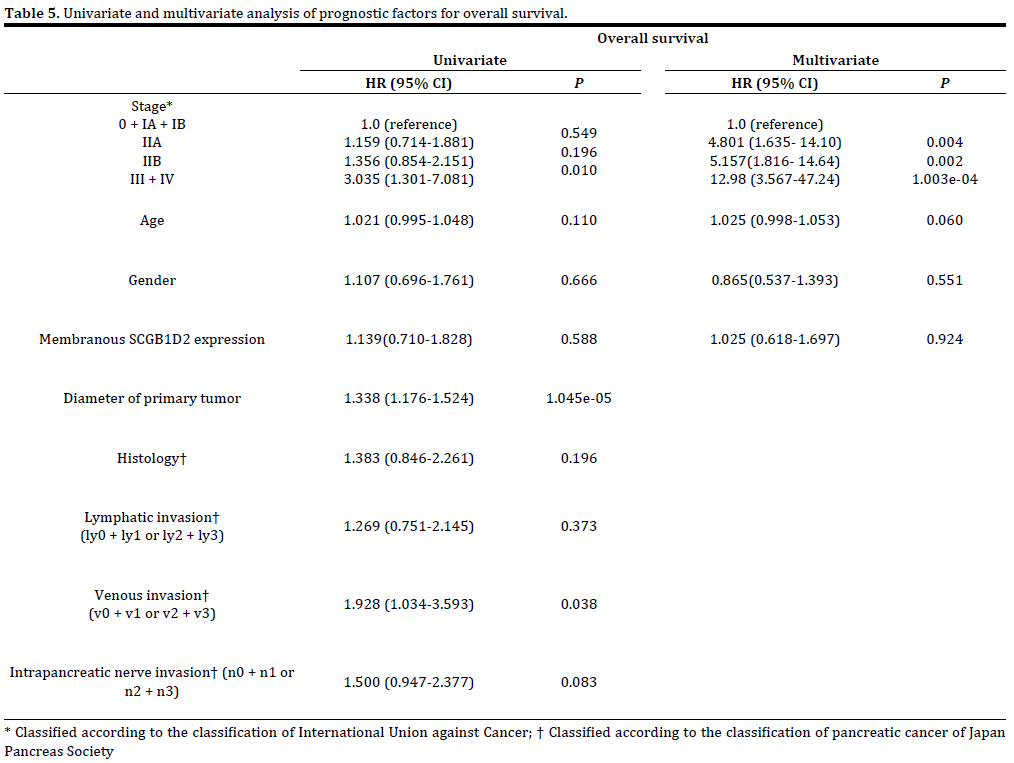
Univariate and multivariate analyses were then used
to assess the prognostic value of SCGB1D2 expression in
PDAC. Stage III and IV UICC TNM classification (hazard
ratio [HR], 3.035; 95% CI, 1.301-7.081; P = 0.010) and high
SCGB1D2 expression (HR, 0.538; 95% CI, 0.337-0.857; P = 0.009) were found to be independent and significant
prognostic factors for worse patient survival by univariate
Cox regression analysis (Table 4). Multivariate survival
analysis supported this finding, showing that Stage III
and IV classification (HR, 13.77; 95% CI, 3.772-50.26; P < 0.001) and high SCGB1D2 expression (HR, 0.556;
95% CI, 0.342-0.903; P = 0.017) were again independent
prognostic factors for poor survival (Table 4). The effects
of Stage III / IV, and SCGB1D2 expression on overall
survival were similar between univariate and multivariate
analyses. Membranous SCGB1D2 expression however, was
not found to be a significant prognostic factor for patient
survival (Table 5).
Localization of SCGB1D2 in Cell Protrusions
We used immunocytochemistry to determine the
subcellular localization of SCGB1D2 in two types of
cultured PDAC cells: moderately differentiated PDAC cells
(line S2-013) [17] and cells from a poorly differentiated
PDAC line (PANC-1) [19]. It has been previously reported
that when S2-013 cells in a suspension attach to an
immobilized fibronectin substrate, nascent membrane protrusions with de novo actin patches at the cell periphery
form, and as these protrusions mature, they promote cell
motility [20, 21]. It has also been reported that both S2-
013 and PANC-1 cells form fewer membrane protrusions
when cultured without fibronectin [12, 22]. Our analysis of
fibronectin-stimulated S2-013 and PANC-1 cells indicated
that SCGB1D2 was mainly present in the cytoplasm of the
cell bodies. It should be noted that S2-013 and PANC-1 cells
showed greater accumulation of SCGB1D2 in membrane
protrusions, that contained many peripheral actin
structures, when cultured on fibronectin compared to cells
cultured without fibronectin (Figure 3a). Z stack panels showed that fibronectin-stimulated S2-013 and PANC-1
cells exhibited intracellular expression of SCGB1D2 within
membrane protrusions (Figure 3b).
Figure 3. Subcellular localization of SCGB1D2 in PDAC cells.
(a). S2-013 and PANC-1 cells were cultured with or without fibronectin and labeled with anti-SCGB1D2 (green), DAPI (blue), and phalloidin for actin
filaments (red). Arrows indicate SCGB1D2 localized within cell protrusions; scale bars, 10 μm. (b). Confocal Z stack showing nuclear DAPI staining (blue),
abundant cytoplasmic SCGB1D2, and the accumulation of SCGB1D2 (green) in the membrane protrusions (arrows) of fibronectin-stimulated S2-013 and
PANC-1 cells. The lower and right panels in the confocal Z stack show a vertical cross-section (yellow lines) through the cells; scale bars, 10 μm. (c). Confocal
immunofluorescence microscopy of S2-013 and PANC-1 cells pretreated with 100 μM cytochalasin D for 12 h and then incubated on fibronectin. Cells were
stained with anti-SCGB1D2 (green), DAPI (blue), and phalloidin for actin filaments (red). Arrows indicate SCGB1D2 localized to cell protrusions; scale bars,
10 μm.
To determine whether alteration of actin cytoskeleton
dynamics could directly affect the subcellular distribution
of SCGB1D2, we treated S2-013 and PANC-1 cells with
the actin depolymerizing agent, cytochalasin D. There
were fewer peripheral actin structures in the fibronectinstimulated
S2-013 and PANC-1 cells exposed to 100
μM cytochalasin D for 12 hr, than in the fibronectinstimulated
non-treated cells, and SCGB1D2 was localized
to the cytoplasm in the treated cells (Figure 3c). In the fibronectin-stimulated non-treated S2-013 and PANC-1
cells, SCGB1D2 was instead localized to the cell protrusions
(Figure 3c).
Role of SCGB1D2 in the Formation of Cell Protrusions
To determine whether SCGB1D2 participates in
the induction of membrane protrusions, we analyzed
the peripheral actin structures in membrane ruffles of
scrambled (control) siRNA and SCGB1D2 siRNA-transfected
S2-013 and PANC-1 cells cultured on fibronectin. SCGB1D2
expression in S2-013 and PANC-1 cells was transiently
suppressed by SCGB1D2-specific siRNAs. Western
blotting performed 48 hr after transfection, showed that
expression of SCGB1D2 was markedly higher in scrambled
siRNA-transfected S2-013 and PANC-1 cells, compared
with SCGB1D2 siRNA-transfected cells (Figures 4a, 4b).
Confocal microscopy showed that SCGB1D2 knockdown
decreased peripheral actin structures, compared to control
S2-013 and PANC-1 cells (Figures 4c, 4d). Furthermore, SCGB1D2-knockdown significantly inhibited the formation
of membrane protrusions, compared to control S2-013
and PANC-1 cells (Figure 4e).

Figure 4. Effects of SCGB1D2 knockdown on the formation of cell protrusions.
(a, b). siRNA oligos targeting SCGB1D2 (siSCGB1D2) or control scrambled siRNAs (Scr) were transiently transfected into either S2-013 (a). or PANC-
1 (b). cells, and analyzed by Western blot using anti-SCGB1D2 antibody. (c, d). siRNAs targeting SCGB1D2 (siSCGB1D2) or control scrambled siRNAs
(Scr) were transiently transfected into S2-013 (c). or PANC-1 (d). cells, and analyzed by confocal immunofluorescence microscopy. Cells were incubated
on fibronectin and stained with anti-SCGB1D2 antibody (green), DAPI (blue), and phalloidin (red). Arrows indicate peripheral actin structures in the
protrusions of Scr-transfected cells; scale bars, 10 μm. (e). Quantification of the data presented in (c). and (d)., respectively. Values represent the number of
cells (mean ± SD) with fibronectin-stimulated cell protrusions in which peripheral actin structures increased. All cells in four fields per group were scored,
in three independent experiments; *p < 0.005 vs. Scr-transfected control (Student’s t-test).
Transfection of the SCGB1D2 rescue construct into S2-
013 and PANC-1 cells that had not been exposed to siRNA
treatment, showed that the protein strongly accumulated in cell protrusions when exogenously expressed (Figures
5a, 5b). Transfection of the SCGB1D2-rescue construct
into SCGB1D2-siRNA transfected S2-013 and PANC-
1 cells successfully abrogated both the decrease in
peripheral actin structures (Figures 5c, 5d), and the
decrease in membrane protrusions, which are peripheral
actin structures (Figure 5e), caused by SCGB1D2-siRNA
knockdown. These results suggest that SCGB1D2 localized
to cell membrane protrusions could play a role in the
formation of these structures in PDAC.

Figure 5. Effects of SCGB1D2 rescue on the formation of cell protrusions in SCGB1D2-siRNA transfected PDAC cells.
(a, b). A myc-tagged SCGB1D2 rescue construct or a mock-construct was transfected into S2-013 (a). or PANC-1 (b). cells, with analysis performed 48 hr
later by Western blot (anti-myc and anti-SCGB1D2 antibodies, left panels) and confocal immunofluorescence microscopy (right panels). For microscopy,
cells were incubated on fibronectin and stained with anti-myc (green), DAPI (blue), and phalloidin for actin filaments (red); scale bars, 10 μm. (c, d). A
myc-tagged SCGB1D2-rescue construct or a mock-construct was transfected into S2-013 (c). or PANC-1 (d). cells that had been co-transfected with either
scrambled control siRNA (Scr) or SCGB1D2-siRNA (siSCGB1D2), with analysis performed 48 h later by confocal immunofluorescence microscopy. Cells
were incubated on fibronectin then stained with anti-myc (green), DAPI (blue), and phalloidin (red). Arrows represent exogenous SCGB1D2 localized to cell
protrusions; scale bars, 10 μm. (e). Quantification of the data shown in (c). and (d). with values representing the number of cells with protrusions in which
peripheral actin structures were increased (mean ± SD). All cells in four fields per group were scored, from three independent experiments; *p < 0.005 vs.
siSCGB1D2 cells co-transfected with mock vector (Student’s t-test).
DISCUSSION
PDAC is one of the deadliest cancers due to its ability to
extensively invade surrounding tissue and to metastasize
at an early stage [23]. Extensive local infiltration and
metastasis are the main causes of death in PDAC [24]. In
this study, we showed that SCGB1D2 expression level is
a prognostic factor that predicts the overall survival of
patients with PDAC. Individual clinicopathological factors
did not significantly correlate with SCGB1D2 expression,
but this may have been due to the remarkably short
overall survival of patients with PDAC. The finding that
patients with a high level of SCGB1D2 expression showed
significantly worse overall survival in both univariate and
multivariate analyses is important, since it demonstrates that SCGB1D2 might be both a novel and independent
prognostic factor for PDAC. Future studies should evaluate
whether the benefits from predicting postoperative
prognosis of PDAC patients by the SCGB1D2-histoscore
scoring system provide the appropriate postoperative
treatment and management. Furthermore, if necessary,
the low-cost SCGB1D2-histological scoring system should
be provided in many countries.
The molecular differences (sequence and posttranslational
modifications) between intracellular
SCGB1D2 and membranous SCGB1D2 are currently
unknown. Notably, membranous SCGB1D2 expression
was observed in 36.3% of resected PDAC tissues. The
fact that histology grade significantly correlated with
the membranous expression of SCGB1D2 indicates
that membranous SCGB1D2 may play a role in PDAC
development and progression, however membranous
SCGB1D2 was not significantly associated with prognosis
in this study.
Our findings indicate that SCGB1D2 is not normally
expressed in pancreas, brain, lung, liver, or kidney,
consistent with a previous report of low SCGB1D2
expression in normal colon, pancreas, heart and lung [9].
SCGB1D2 is abundantly expressed however, in normal and
malignant tissue from the breast, cervix, uterus, ovary and prostate [9]. The fact that SCGB1D2 is absent in normal
pancreas suggests that it is not essential for the normal
functioning of this organ, however its upregulation in PDAC
tissues indicates that the protein could play an important
role in PDAC carcinogenesis.
The present study indicated that SCGB1D2 accumulated
in the protrusions of PDAC cells, as evidenced by
immunocytochemistry. Since the formation of protrusions
is essential for cell migration and invasion, the role of
SCGB1D2 in the formation of these structures could be
important for PDAC progression. Dynamic, actin-based
plasma membrane protrusions that control growthcone
pathfinding include: (i) lamellipodia in which the
actin cytoskeleton assumes a crosslinked and branched
meshwork; and (ii) filopodia, which consist of parallel
bundles of actin filaments protruding from the growth
cone or lamellipodial margin [25]. Migratory competence
of tumor cells requires activation of the motility cycle, the
first step of which is actin remodeling; this remodeling
drives the formation of cell protrusions, defines the
direction of migration, and initiates the growth of the
lamellipodium [26]. In the present study, we have shown
that SCGB1D2 promotes the formation of cell protrusions
in PDAC cells, however the precise mechanism by which
this operates is still unknown. Future studies should
evaluate the SCGB1D2-associated signaling cascades that coordinate the actin-cytoskeletal remodeling required for
the formation of cell protrusions.
Recently, the paradigm of PDAC research has shifted
from a focus on parenchyma to that of stroma [27]. Since
mature SCGBs are secreted proteins composed of homo- and
heterodimers of SCGB polypeptides [6], it is possible that
secreted SCGB1D2 may thus be present in PDAC stroma.
PDAC is one of the most stroma-rich cancers that is known,
with the stroma potentially accounting for more than 90%
of total tumor volume [28]. Many signaling pathways have
been proposed to mediate interactions between PDAC cells
and stroma [29]. For example, the overexpression of matrix
metalloproteinases in PDAC cells plays an important role
in tumor cell migration and invasion [30]. The finding that
SCGB1D2 promotes the formation of protrusions essential
for cell migration, raises the possibility SCGB1D2 secreted
into the stroma may play a role in PDAC metastasis. Future
studies should evaluate the potential interaction of secreted
SCGB1D2 with PDAC-associated stromal cells, and/or other
stromal components, that coordinate the actin-cytoskeletal
remodeling required for cell migration.
To our knowledge, this is the first report to show
that SCGB1D2 is an independent marker of prognosis in
resected PDACs. The accumulation of SCGB1D2 in the
protrusions of migrating PDAC cells, and its role in the
formation of these structures, indicates that this protein
may be an important contributor to the metastatic process
in this disease.
Acknowledgements
We thank Makiko Tsuboi, Aki Tanouchi, Hiroko
Ohshita and Shunichi Manabe for their excellent technical
assistance. This study was supported by Grants-in-
Aid for Scientific Research (KAKENHI; #24591013 and
#15K14396 to KT).
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J
Clin 2013; 63:11-30. [PMID: 21166]
- Hidalgo M. Pancreatic cancer. N Engl J Med 2010; 362:1605-1617.
[PMID: 0901557]
- Locker GY, Hamilton S, Harris J, Jessup JM, Kemeny N, Macdonald
JS, et al. ASCO 2006 update of recommendations for the use of tumor
markers in gastrointestinal cancer. J Clin Oncol 2006; 24:5313-5327.
[PMID: 17060676]
- Klug J, Beier HM, Bernard A, Chilton BS, Fleming TP, Lehrer RI, et al.
Uterglobin/Clara cell 10 kDa family of proteins: nomenclature committee
report. Ann NY Acad Sci 2000; 923:348-354. [PMID: 11193777]
- Alvarez J, Viñas J, Alonso JM, Albar JP, Ashman K, Domínguez P.
Characterization and cloning of two isoforms of heteroglobin, a novel
heterodimeric glycoprotein of the secretoglobin-uteroglobin family
showing tissue-specific and sex differential expression. J Biol Chem 2002;
277:233-242. [PMID: 11684684]
- Ni J, Kalff-Suske M, Gentz R, Schageman J, Beato M, Klug J. All human
genes of the uteroglobin family are localized on chromosome 11q12.2
and form a dense cluster. Ann N Y Acad Sci 2000; 923:25-42. [PMID:
11193762]
- Watson MA, Fleming TP. Isolation of differentially expressed
sequence tags from human breast cancer. Cancer Res 1994; 54:4598–
4602. [PMID: 8062249]
- Sjödin A, Ljuslinder I, Henriksson R, Hedman H. Mammaglobin and
lipophilin B expression in breast tumors and their lack of effect on breast
cancer cell proliferation. Anticancer Res 2008; 28(3A):1493–1498.
[PMID: 18630503]
- Zafrakas M, Petschke B, Donner A, Fritzsche F, Kristiansen G, Knüchel
R, et al. Expression analysis of mammaglobin A (SCGB2A2) and lipophilin
B (SCGB1D2) in more than 300 human tumors and matching normal
tissues reveals their co-expression in gynecologic malignancies. BMC
Cancer 2006; 6:88. [PMID: 16603086]
- Taniuchi K, Furihata M, Hanazaki K, Saito M, Saibara T. IGF2BP3-
mediated translation in cell protrusions promotes cell invasiveness and
metastasis of pancreatic cancer. Oncotarget 2014; 5:6832-6845. [PMID:
25216519]
- Taniuchi K, Furihata M, Saibara T. KIF20A-mediated RNA granule
transport system promotes the invasiveness of pancreatic cancer cells.
Neoplasia 2014; 16:1082-1093. [PMID: 25499221]
- Tanouchi A, Taniuchi K, Furihata M, Naganuma S, Dabanaka K, Kimura
M, et al. CCDC88A, a prognostic factor for human pancreatic cancers,
promotes the motility and invasiveness of pancreatic cancer cells. J Exp
Clin Cancer Res 2016; 35:190. [PMID: 27919290]
- Japan Pancreatic Society. Classification of pancreatic carcinoma. 2nd
English ed. Tokyo: Kanehara & Co., 2003.
- Sobin LH, Gospodarowicz MK, Witteknd C. TNM classification of
malignant tumors. 7th ed, Wiley-Blackwell, New York, 2009; 132-135.
- Larsson A, Johansson ME, Wangefjord S, Gaber A, Nodin B,
Kucharzewska P, et al. Overexpression of podocalyxin-like protein is an
independent factor of poor prognosis in colorectal cancer. Br J Cancer
2011; 105:666-672. [PMID: 21829192]
- Heby M, Elebro J, Nodin B, Jirström K, Eberhard J. Prognostic
and predictive significance of podocalyxin-like protein expression in
pancreatic and periampullary adenocarcinoma. BMC Clinical Pathology
2015; 15:10. [PMID: 26028992]
- Iwamura T, Katsuki T, Ide K. Establishment and characterization of a
human pancreatic cancer cell line (SUIT-2) producing carcinoembryonic
antigen and carbohydrate antigen 19-9. Jpn J Cancer Res 1987; 78:54-62.
[PMID: 3102439]
- Miyazawa Y, Uekita T, Hiraoka N, Fujii S, Kosuge T, Kanai Y, et al. CUB
domain-containing protein 1, a prognostic factor for human pancreatic
cancers, promotes cell migration and extracellular matrix degradation.
Cancer Res 2010; 70:5136-146. [PMID: 20501830]
- Deer EL, González-Hernández J, Coursen JD, Shea JE, Ngatia J, Scaife
CL, et al. Phenotype and genotype of pancreatic cancer cell lines. Pancreas
2010; 39:425-435. [PMID: 20418756]
- Taniuchi K, Nishimori I, Hollingsworth MA. Intracellular CD24
inhibits cell invasion by posttranscriptional regulation of BART through
interaction with G3BP. Cancer Res 2011; 71:895-905. [PMID: 21266361]
- Taniuchi K, Yokotani K, Saibara T. BART inhibits pancreatic cancer
cell invasion by Rac1 inactivation through direct binding to active Rac1.
Neoplasia 2012; 14:440-450. [PMID: 22745590]
- Tsuboi M, Taniuchi K, Furihata M, Naganuma S, Kimura M, Watanabe
R, et al. Vav3 is linked to poor prognosis of pancreatic cancers and
promotes the motility and invasiveness of pancreatic cancer cells.
Pancreatology 2016; 16:905-916. [PMID: 27453460]
- Baumgart M, Heinmöller E, Horstmann O, Becker H, Ghadimi BM. The
genetic basis of sporadic pancreatic cancer. Cell Oncol 2005; 27:3-13.
[PMID: 15750203]
- Ahrendt SA, Pitt HA. Surgical management of pancreatic cancer.
Oncology 2002; 16:725-734. [PMID: 12088296]
- Gallo G, Letourneau PC. Regulation of growth cone actin filaments by
guidance cues. J Neurobiol 2004; 58:92-102. [PMID: 14598373]
- Eiseler T, Döppler H, Yan IK, Kitatani K, Mizuno K, Storz P. Protein
kinase D1 regulates cofilin-mediated F-actin reorganization and cell
motility through slingshot. Nat Cell Biol 2009; 11:545-556. [PMID:
19329994]
- Stromnes IM, DelGiorno KE, Greenberg PD, Hingorani SR. Stromal
reengineering to treat pancreas cancer. Carcinogenesis 2014; 35:1451-
1460. [PMID: 24908682]
- Xie D, Xie K. Pancreatic cancer stromal biology and therapy. Genes Dis
2015; 2:133-143. [PMID: 26114155]
- McCleary-Wheeler AL, McWilliams R, Fernandez-Zapico ME. Aberrant
signaling pathways in pancreatic cancer: a two compartment view. Mol
Carcinog 2012; 51:25-39. [PMID: 22162229]
- Bramhall SR, Neoptolemos JP, Stamp GW, Lemoine NR. Imbalance of
expression of matrix metalloproteinases (MMPs) and tissue inhibitors of
the matrix metalloproteinases (TIMPs) in human pancreatic carcinoma. J
Pathol 1997; 182:347-355. [PMID: 9349239]




