Keywords
Hypodermoclysis; Pancreas; Pancreatitis
Abbreviations
CI Confidence interval; CRP C-reactive protein; DRG
Diagnosis-related group
INTRODUCTION
Acute pancreatitis is a frequent and potentially lifethreatening
event triggered by a variety of different factors.
In the first phase of the disease, a local inflammation ensues
that is associated with local and systemic complications [1].
By current knowledge, the outcome of the inflammation,
once initiated, cannot be influenced by any common drug.
Aggressive fluid therapy is still recommended to improve
local microcirculation and reduce the risk of necrosis [2].
However, there is no reliable evidence for this approach.
In contrary, high volume resuscitation may rather be
detrimental: Patients with severe acute pancreatitis
treated with more aggressive fluid therapy had higher
APACHE II scores and higher rates of mechanical
ventilation, abdominal compartment syndrome, sepsis, and death [3, 4]. In a series of consecutive patients with
acute pancreatitis, the administration of >4.1 L fluid
within the first 24 hours after admission was associated
with persistent organ failure, acute fluid collections,
respiratory insufficiency, and renal failure [5]. We were
able to demonstrate a continuous rise in disease severity,
rate of local complications, and maximum C-reactive protein
(CRP) throughout the total range of administered volume
in an unselected cohort [6]. In a most recent randomized
study, aggressive therapy with lactated Ringer's solution was
associated with a quicker clinical improvement [7]. However,
the rates of local complications and organ failure were not
reported and patients with risk factors for an unfavorable
outcome were excluded. Moreover, the combined endpoint
"clinical improvement" included the decrease of hematocrit
and blood urea nitrogen. A decrease of these parameters can
be expected when fluid is administered.
Wu and coworkers performed a study comparing
"standard" vs. "goal-directed" fluid resuscitation and
normal saline vs. lactated Ringer's solution [8]. The
study was prematurely discontinued due to a stronger
systemic inflammation (CRP and rate of SIRS) after 24
hour in the normal saline group compared to the lactated
Ringer's solution group. According to previous studies in
experimental sepsis [9], the authors linked the stronger
inflammatory response to a hyperchloremic metabolic acidosis. Larger studies in various cohorts indeed imply
a detrimental effect of high-chloride containing fluids: In
patients undergoing major surgery, the use of infusions
with higher chloride-content was associated with a
higher morbidity and mortality [10]. This was attributed
to a higher rate of postoperative infection, renal failure,
blood transfusion, electrolyte disturbance, and acidosis. A
prospective study on chloride-restrictive intravenous fluid
administration in critically ill patients showed a significant
decrease in renal failure and need for renal replacement
therapy [11].
In a retrospective study on patients with acute
pancreatitis admitted to ICU, mortality was lower and
length of stay in the ICU was longer in patients treated with
low-chloride fluids [12]. No information on inflammatory
response or local and systemic complications was
provided. Another study compared the outcome of
consecutive patients initially treated with 1000 mL of
either lactated Ringer's solution or normal saline [13].
There was no difference in disease severity, occurrence of
necrosis, rate of enteral nutrition, length of hospitalization
or mortality. The present study sought to determine the
impact of chloride on inflammatory response and outcome
parameters in acute pancreatitis. We analyzed a large
cohort with a wide range of administered chloride and
detailed charts.
METHODS
Cases of possible acute pancreatitis treated in the
University Hospital of Schleswig-Holstein, Campus Lübeck
from January 2012 to December 2015 were identified by
Diagnosis-related group (DRG) classification. The charts of
all patients at least 18 years of age were retrieved from the
hospital IT system. Patients who had been transferred from
another hospital were excluded. Cases entered analysis if
data confirmed acute pancreatitis according to the definition
of the revised Atlanta Classification on admission. Cases
of onset of acute pancreatitis during the hospital stay for a
different reason were treated accordingly.
The standard procedure for the initial treatment of
acute pancreatitis during the study period was analgesia
and fluid resuscitation. The standard procedure until
November 2012 was an aggressive fluid resuscitation with
Ringer's solution (chloride concentration 156 mmol/L)
in the early phase of the disease. From November 2012,
we recommended a less aggressive volume therapy with
a solution of lower chloride content (Sterofundin Iso®, B.
Braun, Melsungen, Germany, chloride concentration 127
mmol/L). At no time there were mandatory guidelines for
the amount of fluid or the choice of fluid, and the individual
strategy was under the discretion of the attending
physician. All patients were seen by a gastroenterologist
within 24 hours after admission.
Parameters that the attending physician was aware
of on admission and that might have influenced his or
her decision on fluid administration were documented:
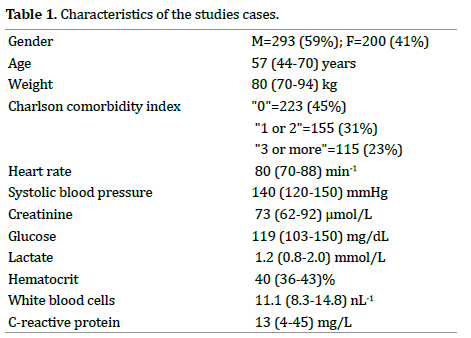
sex, age, weight, Charlson comorbidity index, heart rate, systolic blood pressure, creatinine, glucose, lactate,
hematocrit, white blood cells, initial C-reactive protein.
The choice and the amount of IV fluid and chloride
administration within the first 24 hours after admission
were summed up (including chloride free solutions
and supplementary injectable potassium chloride).
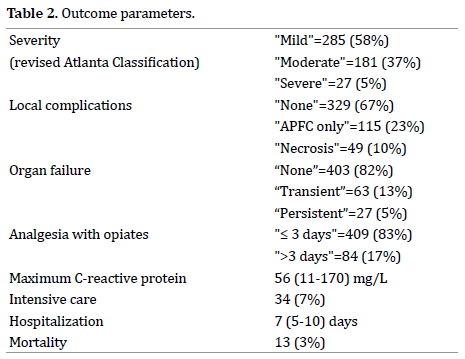
The etiology of the episode and the following outcome
parameters were noted: Maximum measured C-reactive
protein on day 2-7, treatment on intensive care unit, duration
of hospitalization, hospital survival, severity of pancreatitis
by the revised Atlanta Classification, and/or any kind of
local or systemic complication. The pooled data were further
processed without the identification of the patients. The
study was approved by the local ethics committee and was
carried out in accordance with the Declaration of Helsinki.
The anonymity of all participants was guaranteed.
In this presentation numeric parameters are given
as median (1st; 3rd quartile). Where required, continuous
variables were winsorized by fixing extreme values at the
97.5th percentile of the entire distribution. To determine
the impact of chloride administration on outcome,
we defined three major outcome variables: difference
between the C-reactive protein on admission and the
highest measured C-reactive protein on day 2-7 (ΔCRP),
local complications (binary none vs. fluid collection,
necrosis and/or acute pseudocyst), and organ failure
(binary none vs. occurrence of circulatory, respiratory
and/or renal complication at any time). Secondary
outcomes were the evidence of necrosis, of persistent
organ failure (>48 hour), and of renal failure (according
to the definition of the revised Atlanta classification).
We tested whether these outcome parameters could be
predicted by the amount of administered chloride in linear
and logistic regression models where appropriate. For
sensitivity analyses, administered total volume was added
to the resulting models. The results from these models
are given as p-values with Odds ratios (OR) or regression
parameters with 95% Confidence Interval (CI). All analyses
were performed using SPSS and R, version 3.4.0 [14].
RESULTS
Four hundred and ninety-three cases of acute
pancreatitis entered the study. The track of case
identification is given in Figure 1. Etiology was biliary in
204 cases (41%), alcoholic in 139 cases (28%), idiopathic
in 100 cases (20%) and other in 50 cases (10%). In 136
cases (28%) the patient had previously experienced an
acute pancreatitis, in 99 cases (20%) there was evidence for
chronic pancreatitis. Other characteristics of the patients
are given in Table 1. In 268 cases at least one second CRP
was measured during the first week. ΔCRP (defined as the
difference of the initial CRP to the maximum CRP during
the first week) was 69 (16-168) mg/L.
Figure 1: Track of case identification.
The median (1st; 3rd quartile) of the volume administered
in the first 24 hours was 3856 (2400-5000) mL. The median
(1st; 3rd quartile) of the chloride administered in the first 24
hours was 508 (348-666) mmol. Volume administration
was associated with ΔCRP (increase by 13.5 mg/L ΔCRP per 1 L administered volume, 95% CI 6.3; 20.6, p=0.0003; Figure 2 first panel). The administration of 100 mmol
chloride was associated with an increase of 9.0 mg/L
CRP (95% CI 4.1; 13.9, p=0.0004; Figure 2 second panel).
When chloride and volume were both included in the
model as determining variables for ΔCRP, volume showed
the smaller effect even though both effects diminished and
were not significant, and there was no interaction visible
between the two variables.
Figure 2: (a). Relation between the administered volume within the first 24 hours (winsorized) and ΔCRP. (b). Relation between the administered chloride within the first 24 hours and ΔCRP.
Neither volume therapy nor chloride administration had
a measurable impact on the occurrence of complications:
this included the parameters “local complications”,
“necrosis”, “organ failure”, “persistent organ failure”
(Figure 3) as well as “renal failure”. However, there was a
significant relation between ΔCRP and complications. Per
10 mg/L rise in CRP the OR for local complications was
1.064 (95% CI 1.039; 1.089, p<0.001). The respective OR
for necrosis was 1.058 (95% CI 1.027; 1.091; p<0.001). Per
10 mg/L rise in CRP the OR for organ failure was 1.035
(95% CI 1.010; 1.062, p=0.0062). The respective OR for
persistent organ failure was 1.071 (95% CI 1.036; 1.108,
p<0.001).
Figure 3: Amount of administered chloride within the first 24 hours divided by whether the patients developed (a). Local complications, (b). Necrosis, (c). Organ failure, and (d). Persistent organ failure in later course.
DISCUSSION
Several studies have found both more local and systemic
complications in patients with acute pancreatitis treated
with higher volume [3, 4, 5, 6]. While local and respiratory
complications may be explained by edema due to volume
overload, SIRS and renal failure cannot be attributed to fluid
administration itself. These complications may rather be
a consequence of chloride content of the fluid: Chloride is
known to enhance inflammatory response in experimental
sepsis [9] and is associated with renal failure in critical ill
patients [11]. A hyperchloremic metabolic acidosis caused by
chloride rich fluids also impairs renal blood flow [15] and can
cause abdominal discomfort in healthy humans [16].
In line with our previous study from a different
cohort with similar characteristics [6], our present data
show a positive correlation between the amount of fluid
administered within the first 24 hours and systemic
inflammation. In the present study, patients were treated
with a lower amount of fluid (median (1st; 3rd quartile) 3900
(2642; 5100) vs. 5300 (3760; 7100) mL). As a measure for systemic inflammation we now considered the difference
between the CRP on admission and the highest CRP during
the first week (ΔCRP instead of maximum CRP in the
previous study). This may better render the impact of the
initial treatment, especially in cases when CRP was only
measured once on admission (excluded from this analysis).
Our results confirm that fluid therapy indeed enhances the
inflammatory response in acute pancreatitis.
We also found that the amount of administered
chloride related stronger to ΔCRP than the amount of the administered volume. We therefore conclude that
the chloride content of the fluid therapy was primarily
responsible for the increase in inflammatory response.
The results are similar to the small study by Wu and
coworkers [8]. The authors, however, did not report
the baseline CRP. ΔCRP can therefore not be estimated.
In addition, we recorded the highest CRP in the week
after admission instead of the measurement 24 hours
after admission. Despite their differences both studies
document a comparable but small impact of chloride on
CRP in acute pancreatitis. Although our cohort was rather
large, we were unable to find an impact of chloride on
outcome parameters such as local complications, necrosis,
occurrence of organ failure and occurrence of persistent
organ failure (Table 2). In addition, no relation was found
when specifically renal failure was tested. This goes in
line with retrospective study on 103 unselected patients
with acute pancreatitis [13]. In this study, however, the
difference in administered chloride (42 mmol) may a
priori have been small to find an impact. From our results
we conclude that if there was an impact of chloride on
outcome of acute pancreatitis it would be marginal.
The inflammatory response measured by ΔCRP,
however, was related to local and systemic complications.
A rise of CRP on the second day after admission is known
to be associated with the severity of acute pancreatitis [17] and the first CRP after admission with severity and
mortality [18]. There is also a close relationship between
organ dysfunction described by the Marshall score and
the CRP at 48 hours but not the CRP on admission [19].
The fact that the additional inflammatory response
caused by chloride did not affect outcome in our study
could have three reasons. First, local complications such
as acute peri-pancreatic fluid collections might rather
be attributed to volume overload than to the chloride
content of the fluids. In contrast to our previous study [6],
we were now unable to find a relation between volume
therapy and local complications. This may be due to the
smaller amount of administered volume in the present
study. Second, the effect might have been too weak. The
average rise in CRP attributable to chloride in our study
was approximately 32 mg/L with an odds ratio for organ
failure of 1.095. The incidence of organ failure was 14%
(renal failure 7%). These numbers are probably too small
to detect an impact. Third, organ failure itself may promote
inflammation and the tight relation between inflammation
and outcome could be two-sided. In this case, other factors
such as comorbidity would predominantly contribute to
organ failure. Indeed we have recently described a strong
relation between comorbidity and organ failure as well as
mortality in patients with acute pancreatitis [20].
CONCLUSION
In summary, we found that chloride administered by
fluid therapy enhances the inflammatory reaction in acute
pancreatitis. The effect was small and there was no detectable
effect on outcome. There was, however a relation between
the systemic inflammatory response and outcome. Due to
the theoretical disadvantage of systemic inflammation, lowchloride
containing fluids should be advised in the therapy
of acute pancreatitis. A prospective study on fluid therapy in
acute pancreatitis will be inevitable to determine the effect
of fluid and fluid composition on outcome. As pointed out
earlier by Wu and coworkers [8], this study will have to be
multi-centric to achieve adequate power.
Conflict of Interest
All authors are in agreement with the contents of the
manuscript. There is no conflict of interest.
References
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of acute pancreatitis-2012: revision of the Atlanta classification and definitions by international consensus. Gut 2013; 62:102-111. [PMID: 23100216]
- Tenner S. Initial management of acute pancreatitis: critical issues during the first 72 hours. Am J Gastroenterol 2004; 99:2489-2494. [PMID: 15571599]
- Mao EQ, Tang YQ, Fei J, Qin S, Wu J, Li L, et al. Fluid therapy for severe acute pancreatitis in acute response stage. Chin Med J (Engl) 2009; 122:169-173. [PMID: 19187641]
- Mao EQ, Fei J, Peng YB, Huang J, Tang YQ, Zhang SD. Rapid hemodilution is associated with increased sepsis and mortality among patients with severe acute pancreatitis. Chin Med J (Engl ) 2010; 123:1639-1644. [PMID: 20819621]
- de Madaria E, Soler-Sala G, Sanchez-Paya J, Lopez-Font I, Martinez J, Gomez-Escolar L, et al. Influence of fluid therapy on the prognosis of acute pancreatitis: a prospective cohort study. Am J Gastroenterol 2011; 106:1843-1850. [PMID: 21876561]
- Weitz G, Woitalla J, Wellhöner P, Schmidt K, Büning J, Fellermann K. Detrimental effect of high volume fluid administration in acute pancreatitis - a retrospective analysis of 391 patients. Pancreatology 2014; 14:478-483. [PMID: 25451185]
- Buxbaum JL, Quezada M, Da B, Jani N, Lane C, Mwengela D, et al. Early aggressive hydration hastens clinical improvement in mild acute pancreatitis. Am J Gastroenterol 2017; 112:797-803. [PMID: 28266591]
- Wu BU, Hwang JQ, Gardner TH, Repas K, Delee R, Yu S, et al. Lactated Ringer's solution reduces systemic inflammation compared with saline in patients with acute pancreatitis. Clin Gastroenterol Hepatol 2011; 9:710- 717. [PMID: 21645639]
- Kellum JA. Fluid resuscitation and hyperchloremic acidosis in experimental sepsis: improved short-term survival and acid-base balance with Hextend compared with saline. Crit Care Med 2002; 30:300-305. [PMID: 11889298]
- Shaw AD, Bagshaw SM, Goldstein SL, Scherer LA, Duan M, Schermer CR, et al. Major complications. mortality, and resourse utilization after open surgery: 0.9% saline compared to Plasma-Lyte. Ann Surg 2012; 255:821-829. [PMID: 22470070]
- Yunos NM, Bellomo R, Hegarty C, Story D, Ho L, Bailey M. Association between a chloride-liberal vs chloride-restrictive intravenous fluid administration strategy and kidney injury in critically ill adults. JAMA 2012; 308:1566-1572. [PMID: 23073953]
- Aboelsoud MM, Siddique O, Morales Q, Seol Y, Al-Qadi MO. Fluid choice matters in critically-ill patients with acute pancreatitis: lactated Ringer's vs. isotonic saline. R I Med J 2013; 99:39-42. [PMID: 27706278]
- Lipinski M, Rydzewska-Rosolowska A, Rydzewski A, Rydzewska G. Fluid resescitation in acute pancreatitis: Normal saline or lactated Ringer's solution? World J Gastroenterol 2015; 21:9367-9372. [PMID: 26309362]
- R Core Team. R: A language and environment for statistical computing. R Foundation for Statistical Computing, Vienna, Austria. 2017; URL https://www.R-project.org/
- Chowdhury AH, Cox EF, Francis ST, Lobo DN. A randomized, controlled, double-blind crossover study on the effect of 2-L infusions of 0.9% saline and Plasma-Lyte©148 on renal blood flow velocity and renal cortical tissue perfusion in healthy volunteers. Ann Surg 2012; 256:18- 24. [PMID: 22580944]
- Williams EL, Hildebrand KL, McCormick SA, Bedel MJ. The effect of intravenous lactated Ringer's solution versus 0.9% sodium chloride solution on serum osmolality in human volunteers. Anaesth Analg 1999; 88(5):999-1003. [PMID: 10320158]
- Stirling AD, Murray CP, Lee MA. The predictive value of C-reactive protein (CRP) in acute pancreatitis - is interval change in CRP an additional indicator of severity? HPB (Oxford) 2017; 19:874-880. [PMID: 28693979]
- LI Y, Zhao Y, Feng L, Guo R. Comparison of the prognostic values of inflammation markers in patients with acute pancreatitis: a retrospective cohort study. BMJ Open 2017; 3:eo13206. [PMID: 28348184]
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, Parks RW. Association between early systemic inflammatory response, severity of multiorgan dysfunction and death in acute pancreatitis. Br J Surg 2006; 93:738-744. [PMID: 16671062]
- Weitz G, Woitalla J, Wellhöner P, Schmidt KJ, Büning J, Fellermann K. Comorbidity in acute pancreatitis relates to organ failure but not to local complications. Z Gastroenterol 2016; 54:226-230. [PMID: 27043885]




