Emilio Brocchi, Fabio Piscaglia, Miriam Bonora, Natascia Celli, Annamaria Venturi, Lorenzo Fantini, Paola Tomassetti, Roberto Corinaldesi, Raffaele Pezzilli
Department of Internal Medicine and Gastroenterology, Sant’Orsola-Malpighi Hospital, Alma Mater Studiorum, University of Bologna, Bologna, Italy
- *Corresponding Author:
- Raffaele Pezzilli
Department of Internal Medicine
Sant’Orsola-Malpighi Hospital
Via Massarenti, 9
40138 Bologna
Italy
Phone: +39-051.636.4148
Fax: +39-051.549.653
E-mail: pezzilli@aosp.bo.it
Received August 5th, 2005 – Accepted August 24th, 2005
Keywords
Image Enhancement; Pancreatitis, Acute Necrotizing; Tomography, Spiral Computer; Ultrasonography
Abbreviations
CECT: contrast-enhanced computed tomography; EEUS: echo-enhanced ultrasonography
INTRODUCTION
At present, contrast-enhanced computed tomography (CECT) is the technique of choice to confirm the diagnosis of acute pancreatitis; furthermore the computed tomography severity index [1] is at present largely applied to classify the severity of the illness. Echo-enhanced ultrasonography (EEUS) has recently been proposed as a reliable method for staging the severity of acute pancreatitis [2]. We report the imaging of a patient with acute pancreatitis in whom the severity assessment was made by EEUS and confirmed by CECT.
Case Report
An 81-year-old female, was admitted to the our Emergency Room because of persistent epigastric pain of 6-hour duration radiating to the back.
Two months previously, during a check-up examination, a diagnosis of gallstones had been made using ultrasonography. She had been treated with ACE-inhibitors for arterial hypertension and with proton pump inhibitors for non-erosive gastroesophageal reflux disease. She had never smoked, and did not drink coffee or alcohol.
On admission, abdominal examination showed a tenderness of the epigastrium; cardiopulmonary and neurological examinations were normal. Her blood pressure was 130/80 mmHg and the electrocardiogram showed no alterations. The results of a routine blood analysis are reported in Table 1. In particular, increased activity of serum pancreatic enzymes were found. A chest X-ray did not reveal any alterations and plain abdominal X-ray showed an ileus. A microlithiasis of the gallbladder and an enlarged pancreatic gland were found at ultrasonography. The diagnosis of acute pancreatitis was made and the patient was treated medically.
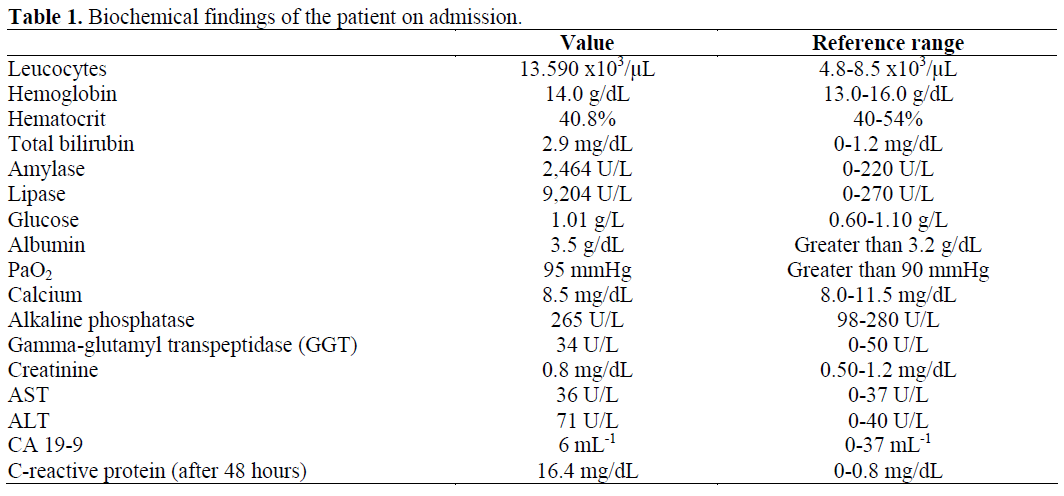
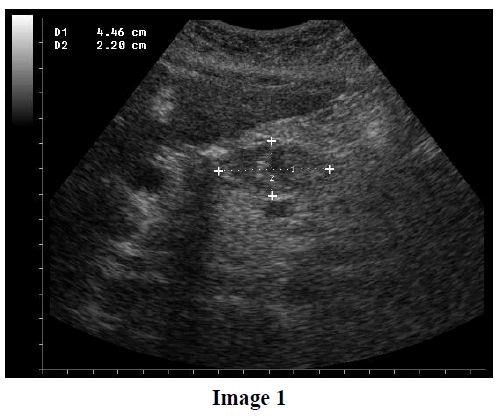
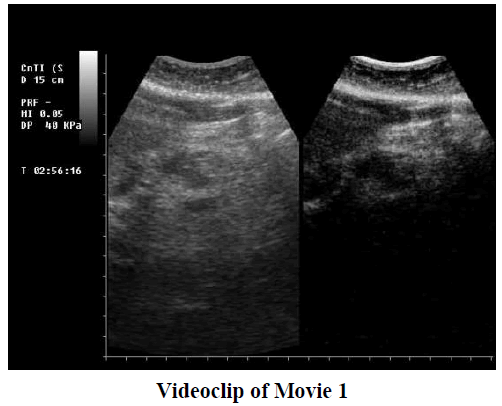
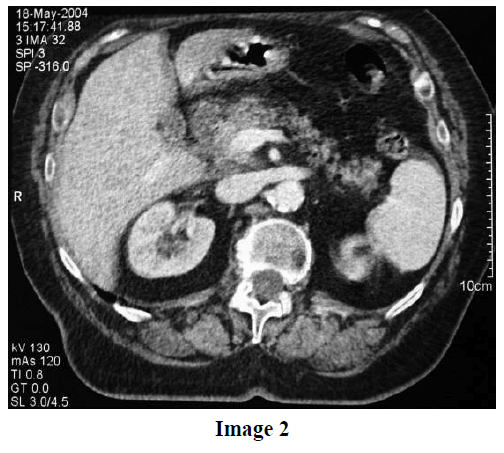
Two days later, due to the persistence of pain and an increased plasma concentration of Creactive protein (16.4 mg/dL, reference range: 0-0.8 mg/dL), but without any physical signs of deterioration, an EEUS was carried out. (Image 1 and Videoclip of Movie 1). Twelve hours later, we also performed a CECT (Image 2).
The pain progressively disappeared over a three day period, and the patient was discharged from the hospital 15 days later. Another EEUS examination was carried out and the patient was cholecystectomized. At present, the patient is still alive; she is in good health, and she has had no relapses of acute pancreatitis.
Imaging Comments
The EEUS showed a hypoechogenic mass of the pancreas of about 45 mm, compatible with necrosis of the pancreatic parenchyma (Image 1 and Videoclip of Movie 1), the Wirsung duct with a diameter of 2.5 mm, an inflammatory lymph node at the hepatic hilus, and complete obstruction of the splenic vein. The CECT (Image 2) performed after 12 hours confirmed the findings seen at EEUS showing an enlarged head of the pancreas with edema of the peripancreatic fat and necrosis of the pancreatic parenchyma.
Conclusions
EEUS may become the imaging technique of choice in assessing the severity of acute pancreatitis since it is easy to perform, safe and lends itself to emergency situations. Most importantly, this technique should be also useful for following-up patients and it may be also an alternative to MRI in those patients in whom CECT cannot be carried out.
References
- Balthazar EJ, Robinson DL, Megibow AJ, Ranson JH. Acute pancreatitis: value of CT in establishing prognosis. Radiology 1990; 174:331-6. [PMID 2296641]
- Rickes S, Uhle C, Kahl S, Kolfenbach S, Moenkemueller K, Effenberger O, Malfertheiner P. Echo-enhanced ultrasound: a new valid initial imaging approach for severe acute pancreatitis. Gut 2005; July 20. [PMID 16033880]

