Kevin Y Wang1, Fatima Fayaaz2, Jeffrey Chi2, Patrick Lee3, Muhammad W Saif4*
1Department of Internal Medicine, Northshore University Hospital, 300 Community Drive, Manhasset NY, USA
2Department of Hematology Oncology, Northshore University Hospital, 300 Community Drive, Manhasset NY, USA
3Department of Radiology, Thomas Jefferson University Hospital, 111S 11th St, Philadelphia, PA, USA
4Professor, Department of Hematology Oncology, Northshore University Hospital, 300 Community Drive, Manhasset NY, USA
- Corresponding Author:
- Muhammad W Saif
Northwell Cancer Institute
Monter Cancer Center
North New Hyde Park, New York, USA
Tel: +6464779400
E-mail: wsaif@northwell.edu
Received Date: July 23rd, 2021; Accepted Date: August 04th, 2021
Keywords
Pancreas; Pancreatic cancer
INTRODUCTION
Pancreatic adenocarcinoma is a significant cause of
morbidity and mortality. While only representing 3.2%
of all new cancer diagnoses in 2021, it is responsible for
7.9% of cancer deaths with a 5 year survival of 10.8%
(2011-2017) [1]. Pancreatic cancer is the 3rd leading cause
of death behind lung cancer (23%) and colorectal cancer
(9%) [1]. The current 5-year relative survival rates for
localized, regional, and advanced stages are 37%, 12%, and
3%, respectively [2] The median overall survival (OS) is
6.7-11.1 months for advanced disease compared to 25-28
months in early-stage disease [3-5]. Even for patients with
locally resectable disease, pancreatic adenocarcinoma
has a high recurrence and metastases rate, with typical
areas being the surgical bed, liver, and lungs [6]. Further
metastatic disease to the bone is rare, usually presenting
as osteolytic metastasis, and is reported to occur in around
3% of cases [7]. Cases of isolated metastatic disease to the
bone is much rarer and is the subject of the following case.
CASE PRESENTATION
An 81-year-old female with a history of mild dementia,
Systemic Lupus Erythematosus, multiple pulmonary emboli and deep venous thrombi, was initially diagnosed
with stage IB pancreatic head adenocarcinoma in the
spring of 2019. She initially presented with symptoms of
abdominal pain. Imaging of the abdomen with ultrasound,
MRI, and CT scans showed double duct sign with no
discrete pancreatic masses. FNA biopsies showed atypical
cell pathology. Endoscopic US showed pancreatic head
mass 11 x 14 mm without evidence of local vessel invasion
[Figure 1]. Ca 19-9 was initially normal, with repeat Ca 19-9
level at >2000 U/mL (reference range 0-37 U/mL). Patient
underwent Whipple surgery with removal of a 3x2.5cm
pancreatic head tumor with negative surgical margins.
Pathology was consistent with invasive moderately
differentiated pancreatic ductal adenocarcinoma. There
were 17 lymph nodes negative for carcinoma consistent
with stage 1B (pT2N0M0) disease. Ca 19-9 returned to
normal levels. Repeat PET-CT and CT scans showed no
signs of recurrent disease.
Figure 1: Endoscopic ultrasound shows a shadowing hypoechoic mass (11x14mm) at the pancreatic head with associated upstream dilatation of the bile ducts.
However, around 1 years after Whipple surgery, the
patient’s Ca 19-9 markers rose to 69 U/mL and then 210
U/mL which prompted a PET-CT scan which showed
mixed sclerotic and lytic lesions with new hyper metabolic
focus in the upper cervical spine [Figure 2]. This prompted
MRI imaging of the cervical and thoracic spine which
showed focal marrow replacing lesions in the C3 as well
as subtle enhancement in the T9 and T11 vertebral bodies
suggestive of osseous metastasis [Figure 3]. Repeat PETCT
also confirmed new metastatic disease [Figure 2].
Correspondingly, the patient developed abdominal pain
and shoulder pain with loss of weight and lack of appetite and was taking oxycodone as needed but the pain became
persistent. Patient and family did not want chemotherapy
and given her mild dementia, would not make a good
candidate. Patient was referred to radiation oncology for
palliative radiation to the bone, and hospice and palliative
care referral for optimization of pain medications and
quality of life.
Figure 2: A) PET scan 13 months after resection of the primary pancreatic tumor shows a mixed sclerotic and lytic lesion with increased metabolic activity at the C3 vertebral body (arrow). (B) A follow-up study 4 months later shows increased size of the FDG avid lesion (arrow) with new extension into the left-sided facet, consistent with metastasis.
Figure 3: (A LEFT TO RIGHT) Sagittal STIR and T1 sequences of the cervical spine show diffuse marrow replacement of the C3 vertebral body (arrow), (C LEFT TO RIGHT) Sagittal post contrast sequences of the thoracic spine show subtle hyperenhancement of focal lesions in the T9 and T11 vertebral bodies suggesting additional sites of metastasis (arrows).
DISCUSSION
In a retrospective analysis of pancreatic cancer with
skeletal metastases, out of 323 patients, 7 patients (2.2%)
were identified with bony metastatic disease [8]. Out of
these 7, none had exclusive bone metastatic disease and
6 presented with concurrent liver metastatic disease
and one with peritoneal metastatic disease. For the bone metastases, most were treated with bisphosphonates.
Systemic chemotherapy was also usually administered
as is the standard for metastatic pancreatic cancer [8].
Palliative radiation is another option in patients presenting
with pain from bony metastases to ameliorate symptoms.
In a retrospective cohort study describing use of palliative
radiation therapy to metastatic pancreatic cancer, 33
patients with bone metastasis were treated with radiation
with most receiving 3000 cGy in 10 fractions with a median
treatment duration of 15 days [9].
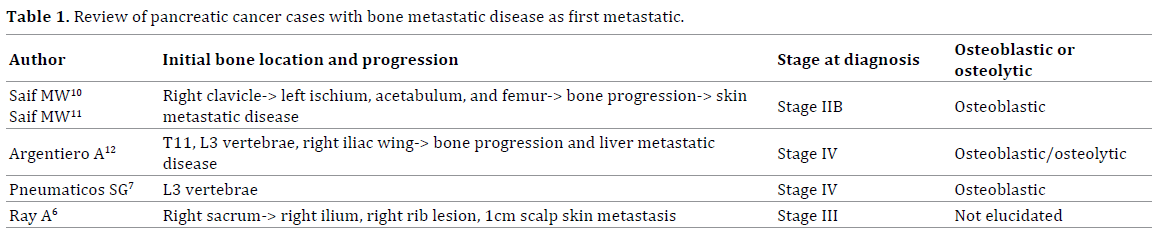
Only three cases of bone metastases without visceral
organ involvement is reported in the literature [Table 1].
Interestingly, two of the cases eventually developed biopsy
proven cutaneous metastatic disease [6, 10, 11]. One case
presented 7 years following Whipple’s surgical resection [6]. Two cases presented with back pain as the initial
presenting symptom [7, 12]. The mechanism for pancreatic
bony metastatic disease is unclear. Two possible theories
include direct posterior extension of the primary tumor to
the lumbar vertebrae or in our case, hematogenous spread
to the Batson’s vertebral vein plexus which bypasses the
liver and the lungs [7, 10].
Unique aspects about our case include having the
earliest stage of disease (stage 1B) prior to development of
bony metastatic disease. However, early stage pancreatic
cancer still has a high recurrence rate and development of
metastatic disease even with potentially curative surgery,
and overall 3 year survival for resected stage 1-2 pancreatic
cancer is around 20-30% compared to 2-19% for stage 3-4
disease [13]. Unlike the above cases, we did not obtain a
bone biopsy to confirm metastatic disease, however the
positive PET-CT and MRI of the spine is highly suggestive
for bone metastases and a bone biopsy in our case would
not change clinical management.
Conclusion
Bone metastasis without visceral organ involvement
is a rare manifestation of pancreatic cancer and back pain
may be the first sign of presentation for pancreatic cancer.
Pancreatic cancer with bone metastasis can occur with any
stage of disease and recurrence is associated with poor
morbidity and mortality as with other metastatic disease
in pancreatic cancer.
Conflicts of Interest
The authors declare no conflicts of interest in
association with the present study.
References
- NIH. Cancer of the pancreas-Cancer Stat Facts. 2021.
- American cancer society. Key statistics for pancreatic cancer. 2021.
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. NEJM. 2013; 369:1691-1703.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med. 2011; 364:1817-1825. [PMID: 21561347].
- Neoptolemos JP, Palmer DH, Ghaneh P, Psarelli EE, Valle JW, Halloran CM, et al. Comparison of adjuvant gemcitabine and capecitabine with gemcitabine monotherapy in patients with resected pancreatic cancer (ESPAC-4): A multicentre, open-label, randomised, phase 3 trial. Lancet. 2017; 389:1011-1024.
- Ray A. Bone metastasis as the only site of disease in a patient 7 years post treatment for a locally advanced pancreatic adenocarcinoma. JOP. 2018; 7.
- Pneumaticos SG, Savidou C, Korres DS, Chatziioannou SN. Pancreatic cancer’s initial presentation: Back pain due to osteoblastic bone metastasis. Eur J Cancer Care (Engl). 2010; 19:137-40. [PMID: 19708936].
- Borad MJ, Saadati H, Lakshmipathy A, Hopper P, Jameson G, Von DD, et al. Skeletal Metastases in Pancreatic Cancer: A retrospective study and review of the literature. Yale J Biol Med. 2009; 82:1-6. [PMID: 19325940].
- Habermehl D, Brecht IC, Debus J, Combs SE. Palliative radiation therapy in patients with metastasized pancreatic cancer-description of a rare patient group. Eur J Med Res 2014; 19:24. [PMID: 24887532].
- Saif MW, Galanina N, Ravage-Mass L, Kaley K, Cornfeld D, Lamb L, et al. Bone metastasis as the only metastatic site in a patient with pancreatic cancer following distal pancreatectomy. Case Rep Med. 2010; 2010:634975. [PMID: 20862374].
- Saif MW, Brennan M, Penney R, Hotchkiss S, Kaley K. Cutaneous metastasis in a patient with pancreatic cancer. JOP. 2011; 3.
- Argentiero A, Calabrese A, Solimando AG, Notaristefano A, Panarelli MMG, Brunetti O. Bone metastasis as primary presentation of pancreatic ductal adenocarcinoma: A case report and literature review. Clin Case Rep. 2019; 7:1972-6. [PMID: 31624620].
- Huang L, Jansen L, Balavarca Y, Babaei M, Geest L, Lemmens V, et al. Stratified survival of resected and overall pancreatic cancer patients in Europe and the USA in the early twenty-first century: A large, international population-based study. BMC Med. 2018; 16:125. [PMID: 30126408].


