Context Predicting the severity of acute pancreatitis early in the course of the disease is still difficult
Objective The value of amylase and lipase levels in serum and peritoneal fluid might be of value in predicting the course of acute pancreatitis.
Design Prospective study.
Patients One-hundred and sixty-seven patients with acute pancreatitis as confirmed by computed tomography scan within 24 hours of admission were studied.
Main outcome measures Each patient was given an enzymatic score which reflected the predominance of serum or peritoneal levels of amylase and/or lipase. Enzymatic score was 0 if neither enzyme was predominant in the peritoneal fluid, 1 if amylase or lipase alone were predominant and 2 if both enzymes were predominant. The predictive value of the enzymatic score or computed tomography scan for a severe attack was determined.
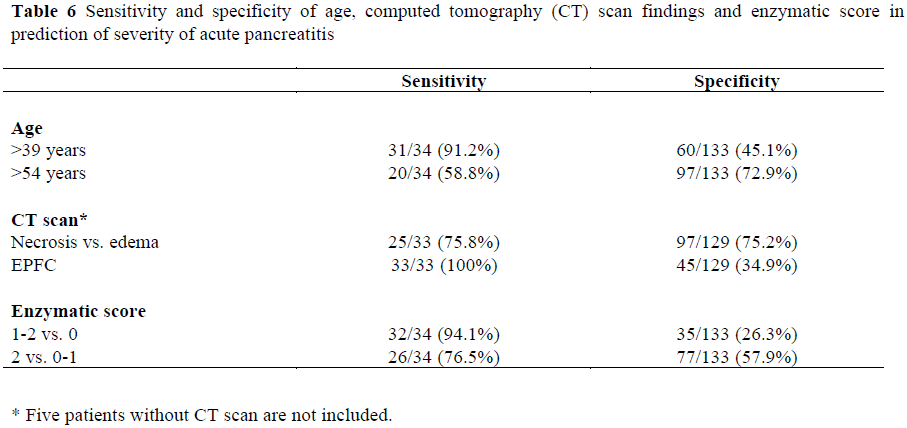
Results One hundred and thirty-three attacks were graded as mild (79.6%) and 34 were considered as severe (20.4%). The frequency of severe acute pancreatitis significantly increased as the enzymatic score increased (5.4%, 12.5%, and 31.7% in 0, 1, and 2 enzymatic score patients, respectively; PP<0.001). An enzymatic score greater than 0 predicted a severe outcome in 32 of 34 patients (sensitivity 94.1%, specificity 26.3%), whereas an enzymatic score of 2 predicted a severe attack in 26 of 34 patients (sensitivity 76.5%, specificity 57.9%). Edema on computed tomography scan was found in 97 of 129 mild attacks (specificity 75.2%) and necrosis in 25 of 33 severe attacks (sensitivity 75.8%), whereas all patients with severe attacks exhibited extrapancreatic acute fluid collection (sensitivity 100%, specificity 34.9%).
Conclusions Peritoneal dialysis is less predictive and more cumbersome than a computed tomography scan in the early prediction of acute pancreatitis.
Keywords
Casuality; Peritoneal Lavage
Abbreviations
AP: acute pancreatitis; CT: computed tomography; EPFC; extrapancreatic acute fluid collection; ES: enzymatic score
INTRODUCTION
The severity of acute pancreatitis (AP) may vary widely: approximately 80% of patients experience mild attacks which are resolved quickly and favorably [1]. The remaining 20%, however, suffer severe attacks [2] associated with mortality rates as high as 20% [3]. If severe attacks were detected at an early stage, aggressive and efficient measures could be resorted to without undue delay. Early clinical findings, such as hypoactive bowel sounds or flank ecchymosis, however, are unreliable in predicting the prognosis of AP and this accounts for the increasing use of prognostic indicators of all types [4, 5].
The relative complexity of multifactorial scales such as the Ranson [6, 7], Imrie [5] and APACHE II [8] scoring systems advocated in the prediction of the severity of AP has prompted many authors to use simpler markers with promising sensibility and specificity ranging between 65-100% and 70-100%, respectively [9-27]. However, these markers are not available in every hospital and some of them proved not to be useful in current clinical practice.
Peritoneal lavage was first proposed in AP by Wall [28] in 1965. The rationale for this procedure arose from the belief that ascites was toxic in AP due to enzymes, and that such toxicity could be partly reduced prior to their absorption into the bloodstream. This appealing concept was seriously questioned, however, when it was found that overall mortality and outcome of severe cases of AP were unaffected by peritoneal lavage. However, peritoneal lavage can provide useful prognostic information in AP. The color of the lavage fluid has been indicated as a sign of severity [29, 30]. Corfield et al [30] used three criteria based on the color and volume of pancreatic ascites to predict more than 50% of severe attacks in a group of 120 dialyzed patients. In a similar fashion, we reasoned that it could be of interest to study the levels of two pancreatic enzymes in the lavage fluid and in serum within 24 hours after admission. The aim of this prospective study was to verify the value of such determinations as prognostic factors in AP.
PATIENTS AND METHODS
From July 1980 to November 1990, 167 patients (111 men and 56 women) suffering from AP were hospitalized in the Clinic of Digestive Surgery and prospectively studied. The characteristics of the population are reported in Table 1.
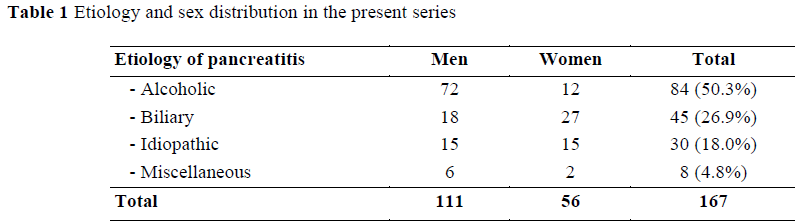
Inclusion criteria were the coexistence of typical abdominal pain and blood amylase levels greater than 235 U/L (normal range: 70-235 U/L); the reason for choosing a diagnostic cut-off level for amylase lower than that in other series was to minimize the number of patients who would have been eliminated had a higher cut-off been chosen. AP was subsequently confirmed by a computed tomography (CT) scan (in 160 patients) according to Balthazar’s scoring system [31, 32], by surgery (in 50 patients) and/or by post-mortem (in 10 patients); the three methods sometimes being used for the same patient. This prospective study was conducted in the late 1980s and since CT scan had just been introduced at that time, we chose to perform an early CT scan. All the results were collected prospectively and attacks of AP were classified as mild, moderate or severe. Then, in the light of new classification systems, we changed the classification retrospectively according to Balthazar scores and the Atlanta criteria. Biliary pancreatitis was suspected when an ultrasound or CT scan showed a common bile duct stone, or when ALAT was higher than twice the normal value. Alcoholism was defined as the daily intake of 80 g of ethanol or more in men, and 60 g in women. Four major causes of AP were identified: alcohol abuse (in 84 patients, 50.3%), biliary lithiasis (in 45, 26.9%), idiopathic causes (in 30, 18.0%) and other miscellaneous causes, such as trauma and postoperative pancreatitis (in 8, 4.8%) (Table 1).
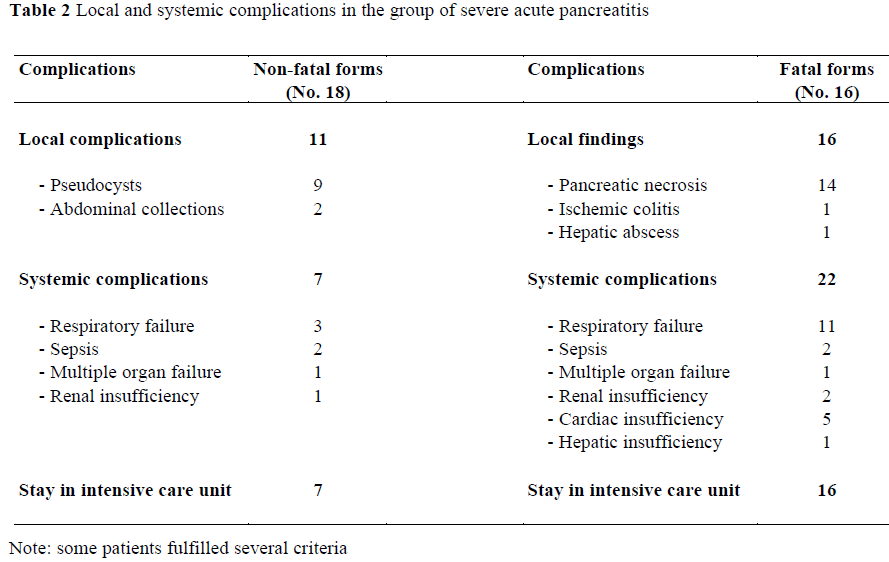
Pancreatitis was defined as mild when the course of the disease was associated only with minimal organ dysfunction and an uneventful recovery. Criteria of severity were based on the Atlanta classification and include the presence of organ failure (including shock, pulmonary insufficiency, renal failure) and/or the presence of local complications (especially pancreatic necrosis, pseudocysts and abscesses).
Within 24 hours of admission, all patients underwent peritoneal lavage. This procedure was always preceded by a CT scan (162 out of 167 patients) to prevent the instilled fluid from disturbing the image (e.g. by producing phantom ascites). CT examinations (third generation Siemens scanner 125 kV, 230 mas, acquisition time 5 seconds) were performed after oral and intravenous administration of contrast media. Eight-mm sections were taken from the level of the diaphragm to the third lumbar vertebra, or further down in the presence of abnormal findings.
Under local anesthesia, a standard peritoneal dialysis catheter was introduced through a small sub-umbilical stab wound. If present, free ascitic fluid was aspirated. Then, isotonic saline serum (1000 cc) was rapidly instilled into the abdominal cavity and left for 30 minutes allowing subsequent collection of 5 cc for amylase and lipase determinations. Amylase and lipase levels were measured simultaneously in blood and peritoneal fluid. Because the range of serum amylase and lipase values were expected to be too wide to be of use as a predictive tool, the patients were thus given an enzymatic score (ES) reflecting the predominance of the serum/and or peritoneal concentrations of the two enzymes. This score was set equal to 0 if neither enzyme was predominant in the peritoneal fluid (peritoneal/serum ratio of amylase and lipase less than 1), 1 if amylase or lipase were predominant therein (peritoneal/serum ratio greater than 1 for one enzyme) and 2 if both enzymes were predominant (peritoneal/serum ratio greater than 1 for both enzymes). The decision to use two enzymes instead of one in the determination of a patient’s ES is based on the poor results obtained using either amylase or lipase alone as previously shown by Robert et al. [33].
ETHICS
The protocol was approved by the Board of the Digestive Surgery Clinic and each patient gave informed consent before enrollment into the study.
STATISTICS
Univariate analyses (Pearson chi-squared, Yates’ corrected chi-squared, chi-squared test for trend, and Spearman rank correlation) were applied. Values of P<0.05 were considered significant. Statistic calculations were done using the SPSS/PC+ Package.
RESULTS
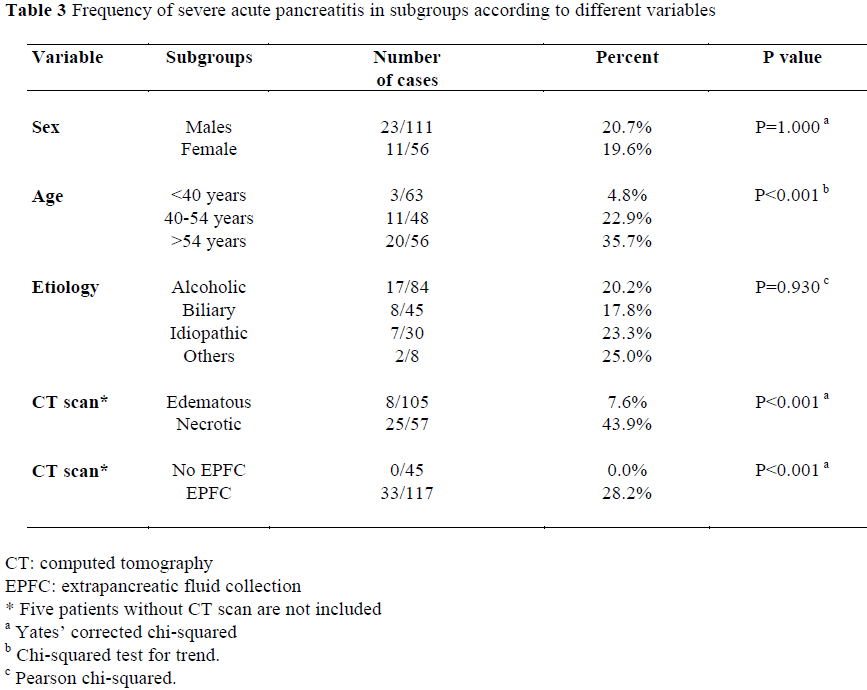
Out of 167 AP patients, 133 attacks were graded as mild (79.6%), while 34 (20.4%) were considered as severe. Local and systemic complications in the group of severe pancreatitis are reported in Table 2. Table 3 compares the characteristics of patients with mild and severe pancreatitis according to different variables such as sex, age, etiology of AP and CT imaging of the pancreas within 24 hours after admission. There was a highly significant tendency for severe attack to increase with age (P<0.001), whereas sex and etiology of AP did not significantly correlate with severity. Pancreatic necrosis and extrapancreatic acute fluid collection (EPFC), both assessed by CT scan, were significantly more frequent in patients with severe AP than in those with mild AP (P<0.001) (Table 3). In our series, all but one case of severe pancreatitis were invariably associated with EPFC.
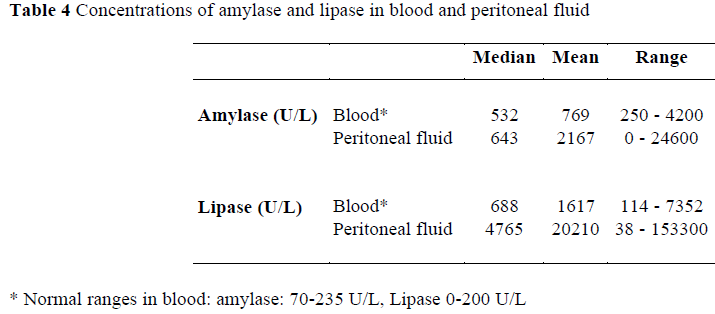
Concentrations of amylase and lipase in blood and peritoneal fluid are shown in Table 4. As expected, the ranges of peritoneal amylase and lipase were extremely wide, particularly for lipase with values as high as 153,300 U/L.
The ES did not appear to vary significantly with either age (P=0.839), or etiology (P=0.065), and it barely varied with sex (P=0.039) (Table 5). A clear significant relationship existed between the ES and CT findings (P<0.001) (Table 5).
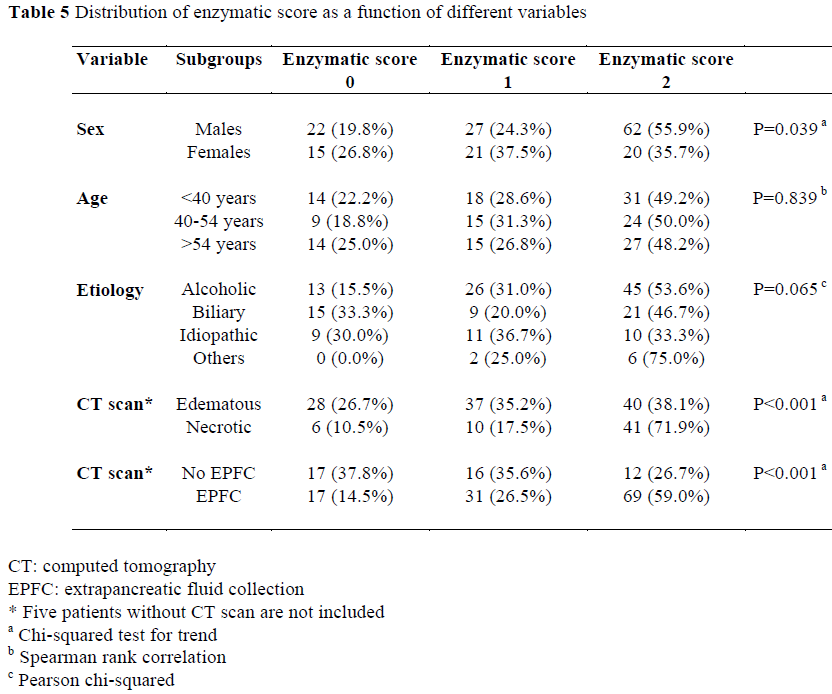
As shown in Figure 1, the ES appeared to be a good indicator of the severity of pancreatitis (P<0.001). In 85 patients with an ES equal to 0 or 1, 9.4% were severe, whereas in 82 patients with ES equal to 2, 31.7% were severe, and mortality was as high as 15.9%. The decision to use two enzymes instead of only one in the determination of a patient’s ES was based on the poor results obtained using either amylase or lipase alone. Sensitivity for amylase alone was 65% whereas sensitivity for the combination of amylase and lipase was 76% in a local preliminary study.
Figure 1. Frequency of severe pancreatitis according to the enzymatic score (P<0.001, Chi-squared test for trend).
In 82 patients with ES equal to 2 mortality was as high as 15.9%.
The ES gains in sensitivity when patients are over 39 years of age. Sensitivity of ES was highest when patients with an ES of 1 or 2 were compared with those with an ES of 0 (Table 6). This is clearly inferior, however, to the information provided by CT imaging of the pancreas. The relevance of EPFC is practically nullified by the low specificity due to the large number of mild attacks found to have EPFC (84/129 patients, 65.1%).
DISCUSSION
Since the work of Ranson [6, 7] in which a scoring system of severity for patients with AP was established, many studies have suggested promising markers to predict the severity of AP [9-27]. However, the complexity of the multifactorial scales and the lack of availability of some new assay kits (for example interleukin-6 and leukocyte elastase) at a reasonable cost have prompted many authors to use simpler and cheaper markers.
Peritoneal lavage can provide useful prognostic information [29, 30]. Numerous studies have determined enzyme concentration in peritoneal effusion and their toxicity in cases of AP [34-36]. Belgian authors [37] have attempted to correlate the serum and peritoneal concentrations of amylase, lipase and lactic dehydrogenase. In their follow-up of 21 cases of severe AP, the peritoneal/serum ratio was invariably greater than 1. In this series, however, all peritoneal enzyme determinations were carried out on free, spontaneously flowing ascites without previous instillation of dialysate. These rough determinations can be expected to be quite elevated. A local study showed that serum and peritoneal determinations appeared to be good indicators of severity [33].
The present study represents an attempt to validate the early predictability of blood and peritoneal determinations of amylase and lipase in AP irrefutably confirmed by CT scan, surgery and/or post-mortem in a large cohort of patients. Our ES appeared to be a good indicator of the severity of the disease, since it is directly and significantly related to the mortality rate and the incidence of EPFC (Balthazar D and E) as demonstrated by a CT scan. However, even though the ES appeared to be correlated to mortality and morbidity, it proved clearly inferior to CT imaging of the pancreas. The presence or absence of EPFC was non-contributory in this study because of the large number of mild attacks found to have EPFC (65% of cases).
For a number of reasons, peritoneal enzyme activity determinations are by no means comparable: 1) the catheters do not always follow the same route and it may be assumed that those which are close to the pancreas will collect fluid with a higher enzyme content and 2) to minimize patient discomfort, the patient position was not changed as often as would have been advisable for ensuring more uniform concentrations. For these reasons, moderate peritoneal enzyme levels may be lower than actual values and should, therefore, be interpreted with some caution, particularly in the case of severe pancreatitis as demonstrated by a CT scan.
The decision to use two enzymes in the establishment of the ES was based on the results of a local preliminary study. It is however possible that the combination of three or more enzymes could slightly improve the sensitivity and specificity of the ES.
In conclusion, peritoneal lavage as a means of closed therapeutic lavage has been shown to be of little value in AP, being excessive in mild attacks and inadequate in severe ones. This study seems to show that as a predictive tool, peritoneal lavage is not worth the trouble either for the patient and or for his doctor. In the light of our results, pancreatitis still represents a challenge for the physician in charge of such patients.
References
- Lankisch PG, Schirren CA, Schmidt H, Schönfelder G, Creutzfeldt W. Etiology and incidence of acute pancreatitis: a 20-year study in a single institution. Digestion 1989; 44:20-5.
- Sauven P, Playforth MJ, Evans M, Pollock AV. Fluid sequestration: an early indicator of mortality in acute pancreatitis. Br J Surg 1986; 73:799-800. [87027188]
- Steer ML. Etiology and pathophysiology of acute pancreatitis. In: Go VLW, DiMagno EP, Gardner JD, Liebentahl E, Reber HA, Scheele GA eds. The pancreas: biology, pathophysiology and disease. 2nd Ed. New York, Raven Press, 593-611.
- Williamson RC. Early assessment of severity in acute pancreatitis. Gut 1984; 25:1331-9. [85077716]
- Imrie CW, Benjamin IS, Ferguson JC, McKay AJ, Mackenzie I, O'Neill J, Blumgart LH. A single-center double-blind trial of Trasylol therapy in primary acute pancreatitis. Br J Surg 1978; 65:337-41. [78166422]
- Ranson JH, Rifkind KM, Turner JW. Prognostic signs and nonoperative peritoneal lavage in acute pancreatitis. SurgGynecolObstet 1976; 143:209-19. [76246498]
- Ranson JHC, Pasternack BS. Statistical methods for quantifying the severity of clinical pancreatitis. J Surg Res 1977; 22:79- 91.
- Knaus WA, Zimmermann JE, Wagner DP, Draper EA, Lawrence DE. APACHE - acute physiology and chronic health evaluation: a physiologically based classification system. Crit Care Med 1981; 9:591-7.
- Fan ST, Lai ECS, Mok FPT, Lo CM, Zheng SS, Wong J. Prediction of the severity of acute pancreatitis. Am J Surg 1993; 166:262-9.
- 10.Viedma JA, Perez-Mateo M, Dominguez JE, Carballo F. Inflammatory response in the early prediction of severity in human acute pancreatitis. Gut 1994; 35:822-7.
- Heath DI, Wilson C, Gudgeon AM, Jehanli A, Shenkin A, Imrie CW. Trypsinogen activation peptides (TAP) concentrations in the peritoneal fluid of patients with acute pancreatitis and their relation to the presence of histologically confirmed pancreatic necrosis. Gut 1994; 35:1311-5.
- Gross V, Scholmerich J, Leser HG, Salm R, Lausen M, Ruckauer K, et al Granulocyte elastase in assessment of severity of acute pancreatitis. Comparison with acute-phase proteins C-reactive protein, alpha 1- antitrypsin, and protease inhibitor 2- macroglobulin. Dig Dis Sci 1990; 35:97-105.
- Appelros S, Thim L, Borgstrom A. Activation peptide of carboxypeptidase B in serum and urine in acute pancreatitis. Gut 1998; 42:97-102.
- Vesentini S, Bassi C, Talamini G, Cavallini G, Campedelli A, Pederzoli P. Prospective comparison of C reactive protein level, Ranson score and contrast-enhanced computed tomography in the prediction of septic complications of acute pancreatitis. Br J Surg 1993; 80:755-7.
- De Beaux AC, Goldie AS, Ross JA, Carter DC, Fearon KCH. Serum concentrations of inflammatory mediators related to organ failure in patients with acute pancreatitis. Br J Surg 1996; 83:349-53.
- Rau B, Cebulla M, Uhl W, Schoenberg MH, Beger HG. The clinical value of human pancreas specific protein procarboxypeptidase B as an indicator of necrosis in acute pancreatitis: comparison to CRP and LDH. Pancreas 1998; 17:134-9.
- Uhl W, Büchler M, Malfertheiner P, Martini M, Beger HG. PMN elastase in comparison with CRP, antiproteases, and LDH as indicators of necrosis in human acute pancreatitis. Pancreas 1991; 6:253-9.
- Funnell IC, Bornman PC, Weakley SP, Terblanche J, Marks IN. Obesity: an important prognostic factor in acute pancreatitis. Br J Surg 1993; 80:484-6.
- Wilson C, Heads A, Shenkin A, Imrie CW. C reactive protein, antiproteases and complement factors as objective markers of severity in acute pancreatitis. Br J Surg 1989; 76:177-81.
- Wilson C, Heath DI, Imrie CW. Predictions of outcome in acute pancreatitis: a comparative study of APACHE II, clinical assessment and multiple factor scoring systems. Br J Surg 1990; 77:1260-4.
- Leser HG, Gross V, Scheibenbogen C, Heinisch A, Salm R, Lausen M, et al. Elevation of serum interleukin-6 concentration precedes acute phase response and reflects severity in acute pancreatitis. Gastroenterology 1991; 101:782-5.
- De Beaux AC, Palmer KR, Carter DC. Factors influencing morbidity and mortality in acute pancreatitis; an analysis of 279 cases. Gut 1995; 37:121-6.
- Inagaki T, Hoshino M, Hayakawa T, Ohara H, Yamada T, Yamada H, et al. Interleukin-6 is a useful marker for early prediction of the severity of acute pancreatitis. Pancreas 1997;14:1-8.
- Millson CE, Charles K, Poon, P, Macfie J, Mitchell CJ. A prospective study of serum pancreatic elastase-1 in the diagnosis and assessment of acute pancreatitis.Scand J Gastroenterol 1998;33:664-8.
- Oezcueruemez-Porsch M, Kunz D, Hardt PD, Fadgyas T, Kress O, Schulz HU, et al. Diagnostic relevance of interleukin pattern, acute-phase proteins, and procalcitonin in early phase of post-ERCP pancreatitis. Dig Dis Sci 1998; 43:1763-9.
- Kaufmann P, Tilz GP, Smolle KH, Demel U, Krejs GJ. Increased plasma concentrations of circulating intercellular adhesion molecule-1 (c-ICAM-1) in patients with necrotizing pancreatitis.Immunobiol 1996; 195:209-19.
- Gross V, Andreesen R, Leser HG, Ceska M, Liehl E, Lausen M, et al. Interleukin-8 and neutrophil activation in acute pancreatitis. Eur J Clin Invest 1992; 22:200- 3.
- Wall AJ. Peritoneal dialysis in the treatment of severe acute pancreatitis. Med J Aust 1965; 2:281-3.
- Mayer AD, McMahon MJ. The diagnosis and prognostic value of peritoneal lavage in patients with acute pancreatitis.SurgGynecolObstet 1985; 160:507-12.
- Corfield AP, Cooper MJ, Williamson RC, Mayer AD, McMahon MJ, Dickson AP, et al. Prediction of severity in acute pancreatitis: prospective comparison of three prognostic indices. Lancet 1985; 2:403-7. [85294815]
- Balthazar EJ. CT diagnosis and staging of acute pancreatitis.RadiolClin North Am 1989; 27:19-37.
- Hill MC, Barkin J, Isikoff MB, Silverstein W, Kalser M. Acute pancreatitis: clinical vs. CT findings. AJR Am J Roentgenol 1982; 139:263-9.
- Robert JH, Meyer P, RohnerA..Can serum and peritoneal amylase and lipase determinations help in the early prognosis of acute pancreatitis? Ann Surg 1986;203:163- 8.
- Dubick MA, Mayer AD, Majumbar APN, Mar G, McMahon MJ, Geokas MC. Biochemical studies in peritoneal fluid from patients with acute pancreatitis. Relationship to etiology. Dig Dis Sci 1987; 32:305-12.
- Bielicki JW, Dlugosz J, Pawlicka E, Gabryelewicz A. The effect of pancreatitis associated ascitic fluid on some functions of rat liver mitochondria. A possible mechanism of the damage of the liver in acute pancreatitis.Int J Pancreatol 1989; 5:145-56.
- Frey CF, Wong HN, Hickman D, Pullos T. Toxicity of hemorrhagicascitic fluid associated with hemorrhagic pancreatitis. Arch Surg 1982; 117:401-4.
- Reynaert M, Otte JB, Kestens PJ. La dialyse péritonéaleet le traitement chirurgical dans 21 cas de pancréatite aigüe nécrotico-hémorragique. Lyon Chir 1980; 76:23-9.


