Keywords
Cholangiopancreatography, Endoscopic Retrograde; Gallstones; Pancreatitis
INTRODUCTION
Persistent ampullary obstruction by an impacted stone or by ampullary edema following stone passage may result in pancreatic edema, inflammation [1], hemorrhage and necrosis with a mortality rate of 13- 50% [2]. Accordingly, early relief of the obstruction is believed to halt the progression of severe attacks as well as prevent the evolution of mild attacks [1]. Early surgical removal of gallstones has been advocated [2]; however, a 1979 study by Ranson showed that surgery within one week of admission in severe pancreatitis was associated with a mortality rate of 67%. This was confirmed by the 1988 randomized controlled trial (RCT) of Kelly and Wagner on 165 patients which showed that surgery within 48 h of admission in severe pancreatitis was associated with a mortality rate of 47.8% as compared to 11.8% with delayed surgery [3]. This led to the abandonment of early surgery. The alternative, endoscopic retrograde cholangiopancreatography with or without endoscopic sphincterotomy, was demonstrated by Classen et al. in 1978 to result in the complete removal of bile duct stones and recovery from pancreatitis in 17 patients [4]
However, difficult cannulation and pancreatic contrast injection during ERCP may potentially worsen pancreatitis. So the question is: would ERCP with or without endoscopic sphincterotomy for biliary obstruction from retained stones or ampullary edema benefit patients with gallstone acute pancreatitis without cholangitis? The results of 7 RCTs comparing early ERCP with or without endoscopic sphincterotomy with conservative treatment yielded contradictory results [1, 2, 5, 6, 7, 8, 9]. We conducted a meta-analysis to determine the effect of early ERCP with or without endoscopic sphincterotomy on the morbidity and mortality of gallstone acute pancreatitis without cholangitis, the latter being an independent indication for early ERCP.
METHODS
Identification and Selection of Studies
Relevant studies were identified and selected by searching the following databases: the Cochrane Library, MEDLINE, EMBASE, the Australasian Medical Index (AMI), Latin American Caribbean Health Sciences Literature (LILACS), and the Health Research and Development Information Network (HERDIN) up to January 11th, 2008 using the search strategy "Gallstone" OR "Gallstone [MESH]" AND "Pancreatitis" OR "Pancreatitis [MESH]" AND "endoscopic retrograde cholangiopancreatography" OR "endoscopic retrograde cholangiopancreatography [MESH]" AND "randomized controlled trial" OR "randomized controlled trial [MESH]" AND "cholangitis" OR "cholangitis [MESH]" where applicable. We also did a full manual search from the reference lists of the trials selected. Authors of the trials retrieved were also contacted for information concerning any trials and relevant unpublished materials. There were no restrictions regarding language, publication date or publication status.
The following selection criteria were applied: 1) study population: gallstone acute pancreatitis patients without cholangitis; 2) intervention: early ERCP with or without endoscopic sphincterotomy vs. conservative treatment within at most 72 h of admission; 3) outcome measures: incidence of morbidity and mortality; 4) study design: randomized controlled trial to guarantee control of selection bias. Papers identified by the searches were evaluated and any papers unrelated to this review were excluded. Decisions at this stage were made based upon the title and abstract. Inclusion decisions were guided by eligibility criteria.
Data Extraction
The following relevant information was also extracted and recorded: country of origin, inclusion and exclusion criteria used, baseline comparability between treatment groups, comparison of types of treatment and number of patients in each arm, drop-outs reported and their reasons, incidence of mortality and morbidity, treatment carried out, and adverse events. In some studies, the reported overall incidence was not used as we had to account for those with baseline cholangitis. One study (Fölsch et al.) [6] did not report mortality and morbidity data according to the severity of baseline pancreatitis. Data reported by the meta-analysis of Ayub et al. [10] as provided by Fölsch et al. were used. Data were entered into Review Manager software (RevMan 4.2, Cochrane Collaboration, Oxford, England, United Kingdom; https://www.cc-ims.net/RevMan).
Quality of Methodology
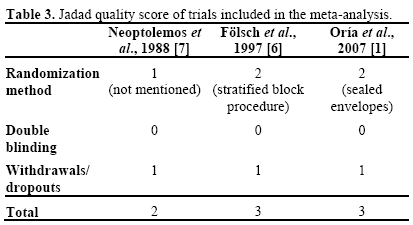
The methodological quality of the studies included in the meta-analysis was scored using the Jadad composite scale. This is a 5-point quality scale, with low-quality studies having a score of less than 3 and high-quality studies having a score ≥ 3. Each study was given an overall quality score based on the above criteria, which was then used to rank the studies.
STATISTICS
The data analysis was carried out using the fixed-effect model with the meta-analysis Review Manager software (RevMan 4.2, Cochrane Collaboration, Oxford, England). The dichotomous mortality and morbidity data were expressed as relative risks (RR), together with 95% confidence intervals (95% CI). The relative risk of adverse events was used for 3 reasons: 1) there is empirical evidence that relative effect measures are, on the average, more consistent than absolute measures; 2) there is also empirical evidence that risk ratios of the adverse outcome are more consistent than ratios of the non-event and 3) it is a concept more familiar to patients and health professionals, and its interpretation is less complicated than for odds. We tested inconsistency between trials with the I2 statistic which describes the percentage of the variability in effect estimates which is due to heterogeneity rather than sampling error (chance), with a value greater than 50% considered as substantial heterogeneity. Funnel plots to address whether there exists publication bias could not be done due to the small number of studies.
RESULTS
Description of Selected Studies
The search strategy yielded 7 studies. Initially, 3 were included (Table 1) and 4 were excluded (Table 2). In general, the studies included involved patients with gallstone acute pancreatitis without cholangitis. Fölsch et al. [6] and Oría et al. [1] specifically excluded acute cholangitis, Neoptolemos et al. [7] provided the information according to the presence or absence of cholangitis.
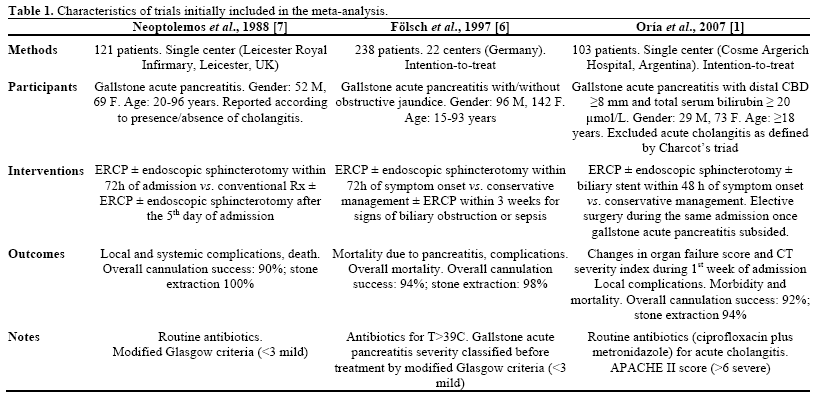

The methodological quality scores of the 3 RCTs included ranged from 2-3 (Table 3): Neoptolemos et al. [7] got a 2 as they did not mention their method of randomization, Fölsch et al. [6] and Oría et al. [1] both got 3. None of them were double blinded. We decided to go ahead with the meta-analyses as ERCP is a complex invasive intervention not amenable to complete blinding. Follow-up and exclusion data are complete. There are no concerns regarding selective reporting.
Meta-Analyses of Clinical Events
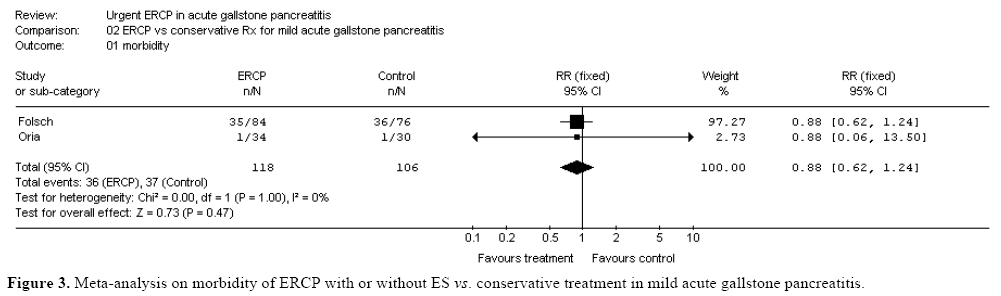
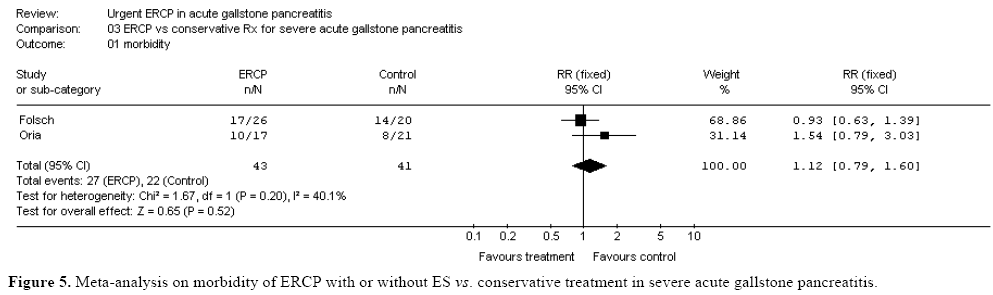
Using a fixed effects model, an overall meta-analysis on the effect of early ERCP with or without endoscopic sphincterotomy on morbidity of acute pancreatitis was inconclusive (RR=0.82, 95% CI: 0.64-1.04). Morbidity meta-analyses for mild and severe pancreatitis were also inconclusive (Table 4).
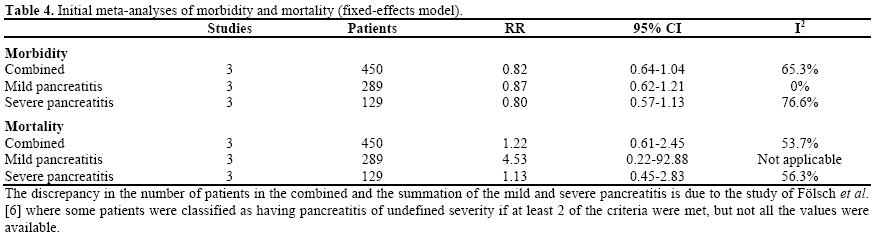
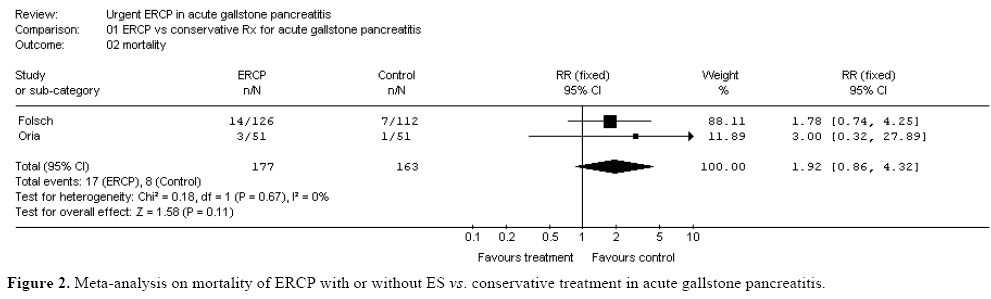
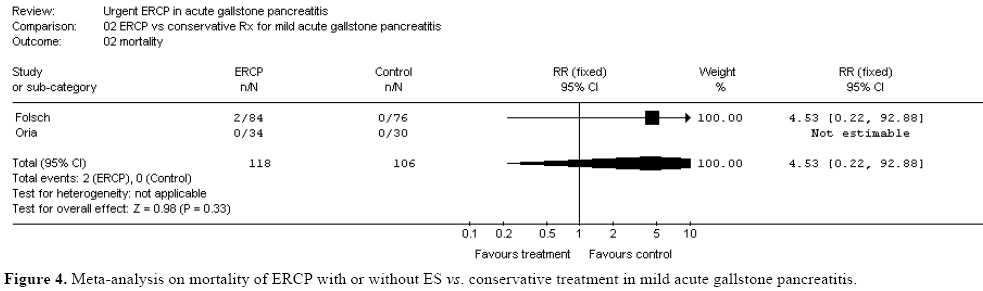
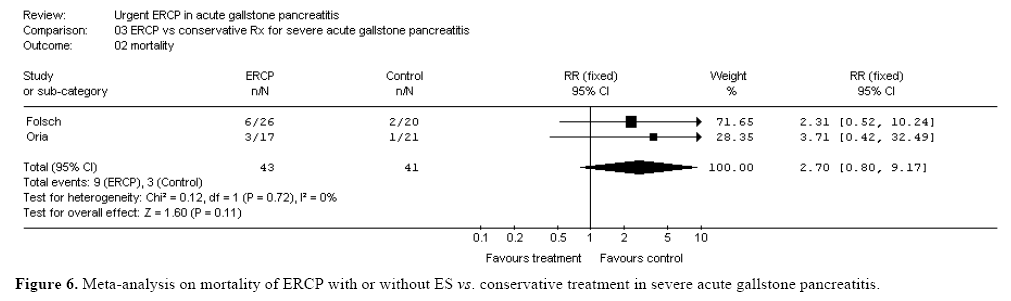
As for mortality, an overall meta-analysis was also inconclusive (RR 1.22, 95% CI: 0.61-2.45). Separate meta-analyses according to the severity of the pancreatitis were also inconclusive for both mild and severe pancreatitis (Table 4).
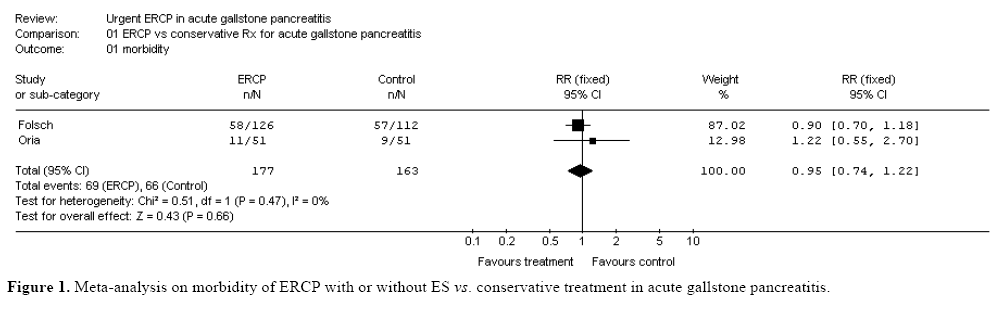
Tests of heterogeneity using the I2 test revealed that the majority of the meta-analyses carried out were heterogeneous. This could be due to the various enrollment criteria of the studies included, i.e., the endoscopic community is hampered by a lack of a strict definition of biliary pancreatitis [3]. A review of these RCTs revealed that the study of Neoptolemos et al. [7] had a relatively lower methodological quality. Furthermore, this study recruited patients “n” hours after admission while the other two studies recruited patients “n” hours after symptom onset. As those who had onset of symptoms long before admission may already have had subsiding gallstone acute pancreatitis, the eventual benefit of ERCP with or without endoscopic sphincterotomy in the study of Neoptolemos et al. may be ascribed to relief of the biliary obstruction, not pancreatitis [1]. This could have biased the outcome in favor of ERCP with or without the endoscopic sphincterotomy group. Therefore, a sensitivity analysis with deselection of the study of Neoptolemos et al. was carried out. Not surprisingly, this yielded more homogenous meta-analyses and different results (Figures 1, 2, 3, 4, 5, 6). Although, overall morbidity meta-analyses were still inconclusive, an overall mortality meta-analysis appeared to be in favor of conservative management. The same applied for meta-analyses performed according to pancreatitis severity.
DISCUSSION
There have been several meta-analyses on the subject. The 1999 meta-analysis of Sharma et al. [4] concluded that ERCP with or without endoscopic sphincterotomy reduces morbidity and mortality in gallstone acute pancreatitis. However, this meta-analysis included the studies of Fan et al. [2] and Nowak et al. [8]. The 2004 meta-analysis of Ayub et al. [10] for Cochrane and the recent 2008 meta-analysis of Moretti et al. [11] both concluded that early ERCP with or without endoscopic sphincterotomy may reduce the odds of having complications in predicted severe gallstone acute pancreatitis, but both also included the study of Fan et al. [2]. Moretti et al. [8] also included the studies of Neoptolemos et al. [7] and Zhou et al. [9]. Moreover just recently in 2008, Petrov et al. [12] reported a metaanalysis which concluded that early ERCP with or without endoscopic sphincterotomy did not reduce complications and mortality of gallstone acute pancreatitis. However, they also included the study of Neoptolemos et al. [7]. The result of this latter metaanalysis was similar to our initial meta-analysis (prior to sensitivity analysis).
The results of our present meta-analysis were different in that they not only suggested that early ERCP with or without endoscopic sphincterotomy might be unnecessary but also that it might possibly lead to higher mortality in both mild and severe gallstone acute pancreatitis. This was not in alignment with current guidelines on the management of gallstone acute pancreatitis which recommend early ERCP for severe gallstone acute pancreatitis [13, 14, 15, 16, 17]. Alhough this is only a trend (P>0.05), it is worth noting that a recent audit revealed that a low compliance of 48% with the UK guideline for 100% ERCP with or without endoscopic sphincterotomy for severe gallstone acute pancreatitis did not increase the complication or mortality rates from severe acute pancreatitis [18].
The following should be considered in the interpretation of the results of this meta-analysis. First, individual patient data were not used.
Second, the cumulative study population is relatively small at 340. The inconclusiveness of the metaanalyses may be due to type II error. Third, the studies included did not have a placebo group.
Fourth, only about half of the patients in the studies included (Fölsch et al. 46% [6], Oría et al. 66% [1]) who underwent a successful ERCP were found to have choledocholithiasis. Indeed, by not excluding patients without choledocholithiasis, these studies may have skewed the possibility of detecting the benefits of early ERCP with or without endoscopic sphincterotomy. Fan et al. [2] showed that, in the presence of confirmed biliary stones, the morbidity rates in the group undergoing early ERCP with or without endoscopic sphincterotomy were significantly lower than those in the conservative-treatment group (P=0.03). They also showed that the mortality rate was lower (P=0.09). The study of Acosta et al. [5] on patients with gallstone acute pancreatitis with ampullary obstruction showed that limiting the duration of the obstruction to not longer than 48 hours by ERCP with or without endoscopic sphincterotomy decreased morbidity. Unfortunately, they did not exclude those with mild cholangitis. In relation to this, the low proportion of patients with confirmed choledocholithiasis reflects the fact that the present definitions of gallstone acute pancreatitis aim to diagnose gallstone acute pancreatitis and not choledocholithiasis. In addition, gallstone acute pancreatitis as we all know, is more often associated with small stones which can transiently obstruct the common bile duct, cause pancreatitis or papillary edema, and pass into the duodenum. Therefore, we need a reliable way of detecting the presence of choledocholithiasis. A recent RCT comparing EUS with or without ERCP with endoscopic sphincterotomy (in the case of choledocholithiasis) to ERCP with or without endoscopic sphincterotomy in 140 patients with gallstone acute pancreatitis showed a more successful examination of the biliary tree with comparable morbidity and mortality risks in patients undergoing EUS with or without ERCP with endoscopic sphincterotomy. Thus, by identifying persistent ampullary obstruction, EUS may spare those who have already passed their stones from an unnecessary invasive procedure, thus preventing the potential risk of ERCP-associated complications [19]. This result was confirmed by Polkowski et al. [20] and Lee et al. [21]. These studies support the recommendations of the British Society of Gastroenterology guidelines that EUS or MR be used to confirm the presence of choledocholithiasis taking into account accessibility and local expertise. They perform better than ultrasound or CT scan [17].
Fifth, the two studies selected included different types of gallstone acute pancreatitis patients. Fölsch et al. [6] excluded all patients with obstructive jaundice while Oría et al. [1] excluded patients with cholangitis, but included those with obstructive jaundice. The fact that, in terms of mortality, the study of Fölsch et al. [6] has more of a trend in favor of the control group than does the study of Oría et al. [1] does could be due to the absence of the need for ERCP with or without endoscopic sphincterotomy in patients without obstructive jaundice.
Finally, it should be noted that gallstone acute pancreatitis by itself may also present with signs of cholangitis-like right upper quadrant pain, fever and jaundice [22]. Moreover, the diagnosis of cholangitis is often problematic because signs and symptoms pointing to the biliary tract as the source of sepsis are often absent in the critical early period of the disease. More importantly, of all the complications of gallstones, cholangitis kills the most swiftly [23].
Adequately powered randomized placebo-controlled multicenter studies using patients diagnosed with a standardized definition of gallstone acute pancreatitis plus confirmed choledocholithiasis but without obstructive jaundice and/or acute cholangitis presenting within a clearly defined period after onset of the disease should be carried out in the future in order to explore the effect of early ERCP or EUS on specific local and systemic complications of gallstone acute pancreatitis. Alternatively, a meta-analysis using individual patient data may provide an opportunity to analyze this. In the meantime, it might be prudent not to carry out early ERCP with or without endoscopic sphincterotomy in patients with gallstone acute pancreatitis unless there is at least a slight suspicion of cholangitis or persistent ampullary obstruction.
Potential conflict of interest
None known
References
- Oría A, Cimmino D, Ocampo C, Silva W, Kohan G, ZandalaziniH, et al. Early endoscopic intervention versus early conservative management in patients with acute gallstone pancreatitis and biliopancreatic obstruction: a randomized clinical trial. Ann Surg 2007; 245:10-7. [PMID 17197959]
- Fan ST, Lai EC, Mok FP, Lo CM, Zheng SS, Wong J. Early treatment of acute biliary pancreatitis by endoscopic papillotomy. N Engl J Med 1993; 28:228-32. [PMID 8418402]
- Behrns KE, Ashley SW, Hunter JG, Carr-Locke D. Early ERCP for gallstone pancreatitis: for whom and when? J Gastrointest Surg 2008; 12:629-33. [PMID 17846851]
- Sharma VK, Howden CW. Metaanalysis of randomized controlled trials of endoscopic retrograde cholangiography and endoscopic sphincterotomy for the treatment of acute biliary pancreatitis. Am J Gastroenterol 1999; 94:3211-4. [PMID 10566716]
- Acosta JM, Katkhouda N, Debian KA, Groshen SG, Tsao-Wei DD, Berne TV. Early ductal decompression versus conservative management for gallstone pancreatitis with ampullary obstruction: a prospective randomized clinical trial. Ann Surg 2006; 243:33-40. [PMID 16371734]
- Fölsch UR, Nitsche R, Lüdtke R, Hilgers RA, Creutzfeldt W. Early ERCP and papillotomy compared with conservative treatment for acute biliary pancreatitis. The German Study Group on Acute Biliary Pancreatitis. N Engl J Med 1997; 23:237-42. [PMID 8995085]
- Neoptolemos JP, Carr-Locke DL, London NJ, Bailey IA, James D, Fossard DP. Controlled trial of urgent endoscopic retrograde cholangiopancreatography and endoscopic sphincterotomy versus conservative treatment for acute pancreatitis due to gallstones. Lancet 1988; 2:979-83. [PMID 2902491]
- Nowak A, Nowkowska-Dulawa E, Marek TA, Rybicka J. Final results of the prospective, randomised, controlled study on endoscopic sphincterotomy versus conventional management in acute biliary pancreatitis. Gastroenterology 1995; 108:A380.
- Zhou MQ, Li NP, Lu RD. Duodenoscopy in treatment of acute gallstone pancreatitis. Hepatobiliary Pancreat Dis Int 2002; 1:608-10. [PMID 14607696]
- Ayub K, Imada R, Slavin J. Endoscopic retrograde cholangiopancreatography in gallstone-associated acute pancreatitis. Cochrane Database Syst Rev 2004; (4):CD003630. [PMID 15495060]
- Moretti A, Papi C, Aratari A, Festa V, Tanga M, Koch M, Capurso L. Is early endoscopic retrograde cholangiopancreatographyuseful in the management of acute biliary pancreatitis? A metaanalysisof randomized controlled trials. Dig Liver Dis 2008; 40:379-85. [PMID 18243826]
- Petrov MS, van Santvoort HC, Besselink MG, van der HeijdenGJ, van Erpecum KJ, GooszenHG. Early endoscopic retrograde cholangiopancreatography versus conservative management in acute biliary pancreatitis without cholangitis: a meta-analysis of randomized trials. Ann Surg 2008; 247:250-7. [PMID 18216529]
- Banks PA, Freeman ML; Practice Parameters Committee of theAmerican College of Gastroenterology. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID 17032204]
- Eisen GM, Dominitz JA, Faigel DO, Goldstein JL, Kalloo AN, Petersen BT, et al. An annotated algorithm for the evaluation ofcholedocholithiasis. Gastrointest Endosc 2001; 53:864-6. [PMID 11375619]
- Forsmark CE, Baillie J; AGA Institute Clinical Practice and Economics Committee; AGA Institute Governing Board. AGA Institute technical review on acute pancreatitis. Gastroenterology 2007; 132:2022-44. [PMID 17484894]
- Working Party of the British Society of Gastroenterology; Association of Surgeons of Great Britain and Ireland; Pancreatic Society of Great Britain and Ireland; Association of Upper GI Surgeons of Great Britain and Ireland. UK guidelines for the management of acute pancreatitis. Gut 2005; 54(Suppl 3):1-9. [PMID 15831893]
- Williams EJ, Green J, Beckingham I, Parks R, Martin D, Lombard M; British Society of Gastroenterology. Guidelines on the management of common bile duct stones (CBDS). Gut 2008; 57:1004-21. [PMID 18321943]
- Mofidi R, Madhavan KK, Garden OJ, Parks RW. An audit of the management of patients with acute pancreatitis against national standards of practice. Br J Surg 2007; 94:844-8. [PMID 17330929]
- Liu CL, Fan ST, Lo CM, Tso WK, Wong Y, Poon RT, et al. Comparison of early endoscopic ultrasonography and endoscopicretrogradecholangiopancreatography in the management of acute biliary pancreatitis: a prospective randomized study. Clin Gastroenterol Hepatol 2005; 3:1238-44. [PMID 16361050]
- Polkowski M, Regula J, Tilszer A, Butruk E. Endoscopic ultrasound versus endoscopic retrograde cholangiography for patients with intermediate probability of bile duct stones: a randomized trial comparing two management strategies. Endoscopy 2007; 39:296-303. [PMID 17427065]
- Lee YT, Chan FK, Leung WK, Chan HL, Wu JC, Yung MY, et al. Comparison of EUS and ERCP in the investigation with suspected biliary obstruction caused by choledocholithiasis: a randomized study. Gastrointest Endosc 2008; 67:660-8. [PMID 18155205]
- Steinberg WM. Acute pancreatitis. In: Feldman M, Friedman LS, and Brandt LJ (eds). Sleisenger&Fordtran's Gastrointestinal and Liver Disease: Pathophysiology / Diagnosis / Management 8th edn. Philadelphia: Saunders-Elsevier; 2006: 1250-1251.
- Browning JD, Sreenarasimhaiah J. Gallstone disease. In: Feldman M, Friedman LS, and Brandt LJ (eds). Sleisenger&Fordtran's Gastrointestinal and Liver Disease: Pathophysiology / Diagnosis / Management 8th edn. Philadelphia: Saunders-Elsevier; 2006: 1412.

