Keywords
Drug Interactions; Enteral Nutrition; Malnutrition; Pancreatic Neoplasms; Parenteral Nutrition
Conflict of interest
The authors have no potential conflicts of interest
Malnutrition and cachexia are frequent complaints in neoplastic disease [1, 2]. Nutritional support and pain treatment still remain the main treatment option for the majority of patients with cancer, particularly for those affected by pancreatic cancer who very often present an advanced stage of the disease at moment of first diagnosis [3, 4, 5]. Therefore, in their clinical practice, physicians are faced with the need for parenteral or enteral nutrition and with the contemporary requirement of several drugs capable of interfering with the components of the nutritional admixture. Different drawbacks may arise from these drug/nutrient interactions, nullifying the pharmacological effect and/or the nutritional value [6]. The aim of this review is to summarize possible drug/nutrient interaction in neoplastic patients, particularly in those with pancreatic cancer, during external food supplementation.
Enteral Nutritional Support
Factors capable of influencing drug/nutrient interactions in enteral nutrition may be related to the patient, to the drug or to the modality of enteral nutrition. These factors are listed in Table 1.
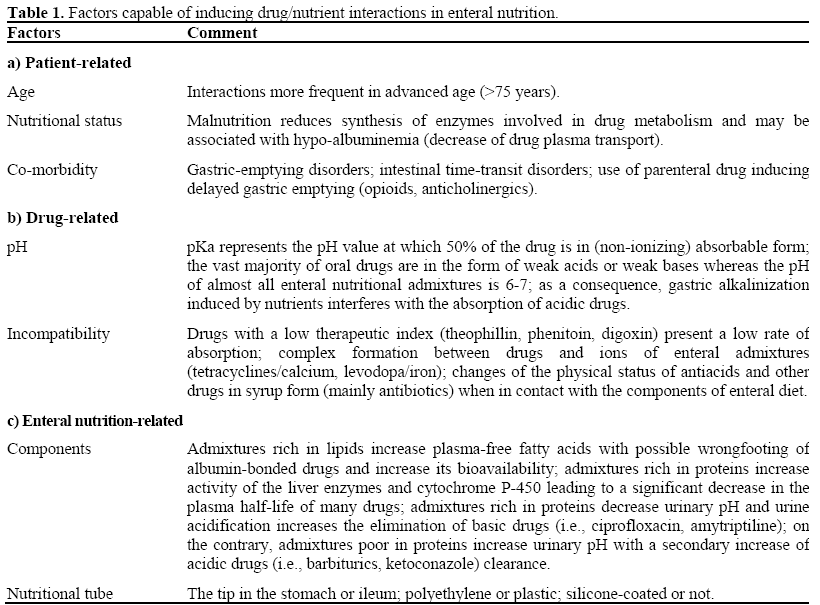
A critical point which has to be stressed is that not all kind of drugs can be added ‘directly’ to the enteral nutritional bag [7]. Direct addition into the nutritional admixture is advised for different reasons: i) there is insufficient information currently available regarding the chemical-physical stability of the admixture when an external component (drug) is added; ii) single components of the enteral diet could interact with a single drug; iii) there is a very high risk of pharmacokinetics changes and microbial contamination, and iv) there is a high risk of naso-gastric/jejunal tube occlusion [8]. Therefore, if we need to administer a drug through the enteral tube, we have to temporarily interrupt the nutrition. Another important point to consider is that specific pharmaceutical formulations for nasogastric/ jejunal tube administration are not commercially available; consequently, we have to adapt different already-disposable oral preparations to our needs.
Theoretically speaking, all liquid formulations are suitable for trans-tube administration; nevertheless, some questions on this matter must be addressed. Syrup formulations contain a variable amount of sorbitol (i.e., up to 10-25 g of sorbitol for one dose of 300 mg of theophylline) with a potential sharp increase of the osmolarity, and a secondary risk of tube occlusion [9]. Moreover, syrup with a pH less than 4 can destroy the emulsion, causing occlusion of the feeding tube. In addition, for adult purposes, pediatric syrups must be used in large volumes in order to gain sufficient drug concentration. Suspensions are generally much too viscose and require elaborate dilutions. The majority of tablets, pills, and hard gelatin capsules may be administered through the feeding tube; however, tablets and pills must be crushed, capsules opened and then the powder obtained must be suspended in sterile water. On the contrary, sublingual tablets, coated pills or capsules, retard/controlled-release and gastro-resistant formulations are not suitable for administration through the enteral feeding tube. A practical multi-step list to optimize multiple oral drug administration in a patient receiving enteral feeding is summarized in Table 2. In addition, Figure 1 shows a plausible flow-chart for the administration of oral drugs through an enteral feeding tube.
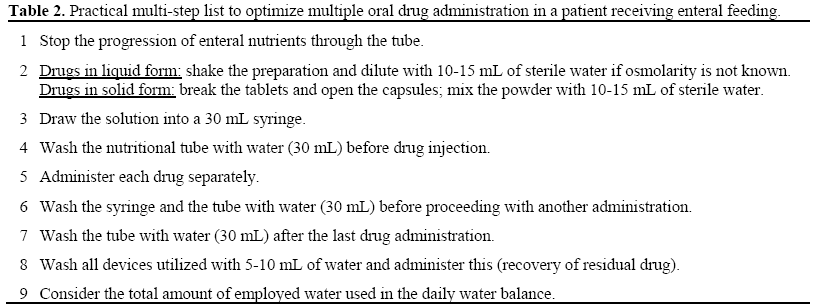
Figure 1. Flow-chart for the administration of oral
drugs through a feeding enteral tube.
EN: enteral nutrition
GI: gastrointestinal
In patients suffering from pancreatic cancer, enteral nutrition is more rarely utilized in comparison with total parenteral nutrition. Duodenal involvement in the locallyadvanced stage of the disease renders the correct placement of a nutritional tube very difficult; therefore, enteral nutrition is virtually impossible in these patients without cutaneous ileostomy. Some oral drugs could be more frequently required in these patients. Among protonic pump inhibitors, lansoprazole and omeprazole may be administered (open the capsules, do not break the granules and suspend them in 8.4%- sodium bicarbonate, keep sheltered from light, store in fridge) but esomeprazole and rabeprazole are not compatible [10]. Morphine sulphate may be administered in liquid form only; as a rule, an increasing frequency of administration according to pain control is required.
Intravenous Nutritional Support
Neoplastic patients on partial or total parenteral nutrition (TPN) usually receive many medications via the parenteral route. This represents the rule for patients with advanced pancreatic cancer who receive TPN as unique means of maintaining nutritional status and may simultaneously require several drugs for treating the cancer-related symptoms or critical co-morbidities. However, simply because a drug is customarily administered via the parenteral route does not make it suitable for addition to the nutritional medium. Combining drugs with nutrient solutions is for reasons of convenience, efficiency, and a reduced potential for infection. However, for these benefits to be realized, a drug must maintain its pharmacologic effect during continuous infusion, infrequent dosage adjustment is required, and it should be intended for chronic rather than intermittent treatment [9]. Even when these demanding criteria are met, a drug must, above all, be compatible with the nutrition admixture. Incompatibility is based upon all chemical and physical phenomena arising from the direct interaction between the single drug and the nutritional components. The frequency and extent of incompatibility rise sharply as temperature is increased; nevertheless, compatibility is commonly evaluated when drug-containing solutions are held below room temperature (during or after maintenance under refrigeration). In parenterally nourished cancer patients, TPN and underlying cancer can produce different effects on compatibility and stability (Figure 2). As a consequence, pharmacologic response to a drug may be increased, unchanged or decreased depending on the net effect of these individual changes. In addition, little information from scientific literature is currently available on the direct interaction between drugs and parenteral nutritional components as comprehensive studies are often impossible in the clinical setting. Evidence exists regarding the incompatibility of all kinds of drugs with ‘single’ preparations of: i) lipid emulsions; ii) high-concentration glucose solutions; iii) amino acid solutions; iv) sodium bicarbonate solution; and v) hypertonic solutions [11]. Finally, we must keep in mind that current TPN admixtures, consisting of multiple components (glucose, amino acids, lipids, trace elements, vitamins) are already highly unstable and that morbidity and mortality can occur from unrecognized precipitate formation in all-in-one parenteral nutrition admixtures [12].
Figure 2. Relationship between parenteral nutrition,
drugs, pharmacological response and cancer.
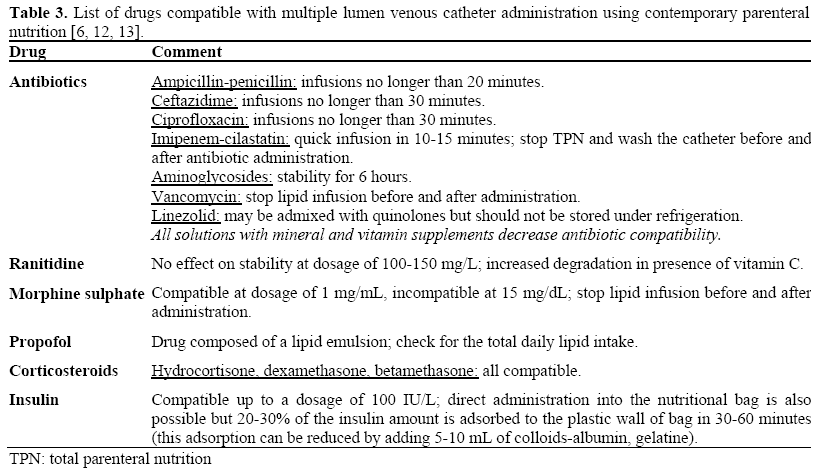
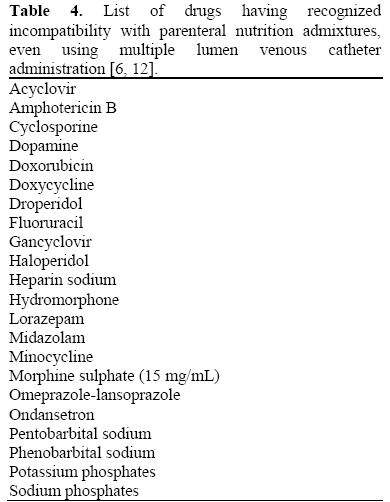
For the above-mentioned reasons, for the maximum safety, “drugs should be administered through a different venous access” than that of the TPN. But, separate administration is not always possible and the line being used to infuse TPN continuously may be the only intravenous access available. Even if multiple lumen catheters are used, the numbers of parenteral doses required in highintensity therapeutic settings, such as cancer chemotherapy or intensive care, may make simultaneous administration with a parenteral nutrition admixture necessary, if not inevitable. During the simultaneous Y-site administration of two infusions, contact does not occur until they reach the common Y-site. Contact times of the admixtures from that point through the remainder of the tubing until they reach the patient’s bloodstream are typically 15 to 30 minutes but can reach 60 minutes in slow administration situations. Recent studies on multiple lumen venous catheters showed that it is possible to recognize which drugs can be administered (Table 3) and which cannot (Table 4) due to problems of incompatibility [6, 12, 13]. Therefore, in clinical practice and for compatible drugs only, this method of administration may be very useful when the central line for TPN represents the only available venous access.
Conclusions
In recent decades enteral nutrition and TPN have developed into a therapeutic modality not only for transient nutritional support but also for patients with advanced cancer for whom no other means are available for maintaining nutritional status. [9, 10, 11, 12]. Contemporary administration of several drugs to control cancer symptoms and/or treat comorbidities represents a very frequent event in clinical practice. Physicians should be on the alert for possible interactions between the components of enteral/parenteral nutrition admixtures and various drugs as considerable risks do exist nullifying both the effect of the drug and the nutritional value, resulting in serious adverse effects. In this regard, pharmacist play an important role in helping physicians in their daily practice. The various tasks of pharmacist managing such patients on artificial nutrition are: advising suitable routes for drug administration, formulation or alternative preparations; monitoring loss of efficacy, or toxicity due to drug interactions with the nutritional component; checking for reduced absorption due to feeding tube problems; educating the nursing staff regarding administration techniques and contributing to in-service training; planning collaboration between hospital and community pharmacies regarding formulations and appropriate administration technique once the patient is discharged.
References
- Walker PK. The anorexia/cachexia syndrome. Primary Care Cancer 2001; 21:13-7.
- Inui A. Cancer anorexia-cachexia syndrome: current issues in research and management. Cancer J Clin 2002; 52:72-91. [PMID 11929007]
- Ellison MM, Chevlen E, Still CD, Dubagunta S. Supportive care for patients with pancreatic adenocarcinoma: symptom control and nutrition. HematolOncolClin North Am 2002; 16:105-21. [PMID 12063822]
- Li D, Xie K, Wolff R, Abbruzzese JL. Pancreatic cancer. Lancet 2004; 363:1049-57. [PMID 15051286]
- Uomo G, Gallucci F, Rabitti PG. Anorexiacachexia syndrome in pancreatic cancer: recent development in research and management. JOP. J Pancreas (Online) 2006; 7:157-62. [PMID 16525199]
- Trissel LA, Gilbert DL, Martinez JF, Baker MB, Walter WV, Mirtallo JM. Compatibility of medications with 3-in-1 parenteral nutrition admixtures. JPEN J Parenter Enteral Nutr 1999; 23:67-74. [PMID 10081995]
- DeLegge MH. Enteral feeding. CurrOpinGastroenterol 2008; 24:184-9. [PMID 18301269]
- Roberts E. Nutritional support via enteral tube feeding in hospital patients. Br J Nurs 2007; 16:1058- 62. [PMID 18026050]
- Total parenteral nutrition. In: Lebenthal E, ed. Raven Press, New York, USA: 1986.
- Thomovsky E, Backus R, Reniker A, Mann FA, Dodam JR. Parenteral nutrition: formulation, monitoring, and complications. CompendContinEduc Vet 2007; 29:88-102. [PMID 17727159]
- Koretz RL. Parenteral nutrition and urban legends. CurrOpinGastroenterol 2008; 24:210-4. [PMID 18301273]
- American Society for Parenteral and Enteral Nutrition (A.S.P.E.N.) Board of Directors and Nurses Standards Revision Task Force, DiMaria-Ghalili RA, Bankhead R, Fisher AA, Kovacevich D, Resler R, Guenter PA. Standards of practice for nutrition support nurses. NutrClinPract 2007; 22:458-65. [PMID 17644701]
- Zhang Y, Xu QA, Trissel LA, Williams KY. Compatibility and stability of linezolid injection admixed with three quinolone antibiotics. Ann Pharmacother 2000; 34:996-1001. [PMID 10981243]



