Keywords
Australia; Pancreatitis, Acute Necrotizing /etiology; Prescriptions
Abbreviations
DM: diabetes mellitus; PCOS: polycystic ovarian syndrome
INTRODUCTION
Acute pancreatitis is associated with morbidity and even the risk of mortality [1, 2]. In the absence of a specific therapeutic agent [3], removal of the offending agent, fluids resuscitation [4], and antibiotic therapy (when indicated) constitute the best chance of cure. Alcohol and gallstones are the most important causes of acute pancreatitis around the world [5, 6, 7], as well as in Australia [8].
Routine prescription drugs have been linked to the causation of acute pancreatitis [9, 10]. However, the precise nature of this association (incidence and pathogenesis) is unclear owing to the fact that much of our current knowledge of drug-induced acute pancreatitis has been obtained from case reports [11]. A few large studies from Europe [12, 13, 14] have estimated the percentage of drugs as a cause for acute pancreatitis to be between 0.3 to 5.3%.
To date, there is no study elucidating the incidence of drug-induced acute pancreatitis in adult Australians. The aim of this study was to determine the incidence, presentation, course and outcome of drug-induced acute pancreatitis amongst patients admitted to a public hospital in Australia.
METHODS
A retrospective search of a prospectively maintained electronic database of the Modbury Hospital, South Australia was undertaken. International Classification of Diseases (ICD) codes for acute pancreatitis for a 64- month period, from January 2006 to April 2011 were analysed with the aim of identifying all patients admitted to the hospital with acute pancreatitis. ‘Acute pancreatitis’, ‘biliary acute pancreatitis’, ‘idiopathic acute pancreatitis’, ‘alcohol-induced acute pancreatitis’, ‘drug-induced acute pancreatitis’, ‘acute pancreatitis unspecified’ codes were included in the search amongst others. This resulted in a total of 7 ICD codes being used with 429 admissions being identified. Each admission was reviewed within the electronic database for patient admission details. The case records of patients identified to have acute pancreatitis were manually reviewed.
Acute pancreatitis was diagnosed by the concurrence of at least two of the following findings [15]: 1) acuteonset epigastric abdominal pain; 2) elevated serum amylase and/or lipase levels more than 3 times the upper level of normal range; and 3) imaging evidence of pancreatic inflammation. Disease severity was classified on the basis of the Atlanta Classification [16].
Cases of drug-induced acute pancreatitis were defined after a careful analysis using an algorithm previously published [17]. In all patients, a history of an alcohol binge or prior admission for alcohol-related acute pancreatitis was obtained. Additionally, all patients underwent an ultrasound to confirm/rule out gallstones as a cause. A history for new onset diabetes mellitus was sought. Trauma as a cause was ruled out based on history. All patients had complete biochemical investigations including serum calcium and triglyceride levels. Based on these investigations, if a cause for acute pancreatitis could not be found, a computed tomography (CT) scan of the abdomen was performed to rule out malignancies. In case of suspected malignancies, serum CA 19-9 levels were performed. Despite this, if no cause could be found, a magnetic resonance cholangiopancreatography was performed to rule out congenital malformations/autoimmune pancreatitis. If all the above were unremarkable, the patients drug history was sought and the relationship between the commencement of the drug and the attack of acute pancreatitis was noted. If all this failed to reveal the aetiology, the patient was labelled as having idiopathic acute pancreatitis. Viruses were considered as a cause for acute pancreatitis when the patients developed a severe viral illness necessitating admission and who went on to develop abdominal pain and CT findings consistent with acute pancreatitis. In some of our patients with drug-induced acute pancreatitis, the causality of the drug was directly considered as the patients presented with acute pancreatitis with the only positive history being consumption of the offending drug prior the attack and no confounding history of alcohol and lack of gallstones on ultrasound. In the only patient with suspected autoimmune pancreatitis based on imaging, the entire screen for markers including immunoglobulin 4 (IgG4) and autoantibodies as well as an endoscopic ultrasonography and fine needle aspiration were performed which were inconclusive for autoimmune pancreatitis. The drugs were classified based on the review of drug-induced acute pancreatitis by Badalov et al. [18].
If drug reaction was suspected to be an aetiological factor and all other causative factors were excluded by appropriate diagnostic methods, the WHO Probability Scale for the evaluation of causality relationship between acute pancreatitis and the suspected drug therapy was used case-by-case [14]. Drug aetiology was definitively assessed only if the case met the criteria of certain, probable, or possible causality of adverse drug reaction [19].
ETHICS
No approval of the institutional review committee was needed because the data of the present study were collected in the course of common clinical practice and, accordingly, the signed informed consent was obtained from each patient for any surgical and clinical procedure. The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
STATISTICS
All statistical analyses were performed using the Statistical Product and Service Solutions, SPSS 14.0 for Windows. Nominal data is provided as absolute and relative frequencies and continuous data as median (range).
RESULTS
A total of 429 admissions over the 64-month period were identified for further analysis. Three-hundreds and 28 patients, confirmed to have acute pancreatitis, accounted for these 429 admissions (indicating that more than one patient had multiple admissions) and were included in the final analysis.
Overall Cohort of Acute Pancreatitis
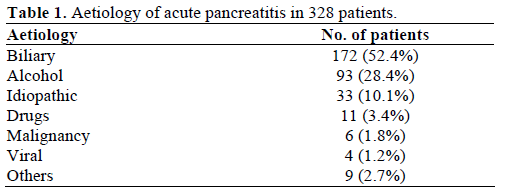
Biliary disease (52.4%) and alcohol (28.4%) were the most common aetiological factors for acute pancreatitis in the overall cohort. The other causes for acute pancreatitis have been listed in Table 1. Acute pancreatitis was found to be more common in women (177; 54.0%) as compared to men (151; 46.0%). The median age for the disease was 54 years (range: 16-98 years) with a median hospital duration stay of 4 days (range: 1-27 days).
Drug-Induced Acute Pancreatitis
Eleven out of 328 patients (3.4%) were diagnosed with drug-induced acute pancreatitis. These included 9 female and 2 male patients with a median age of 59 years (range: 17-70 years). These included 5 cases of codeine-, 2 cases of azathioprine- (in patients with Crohn’s disease), and 1 case each of chlorothiazide-, valproic acid-, oestradiol- and rosuvastatin-induced acute pancreatitis (Table 2).
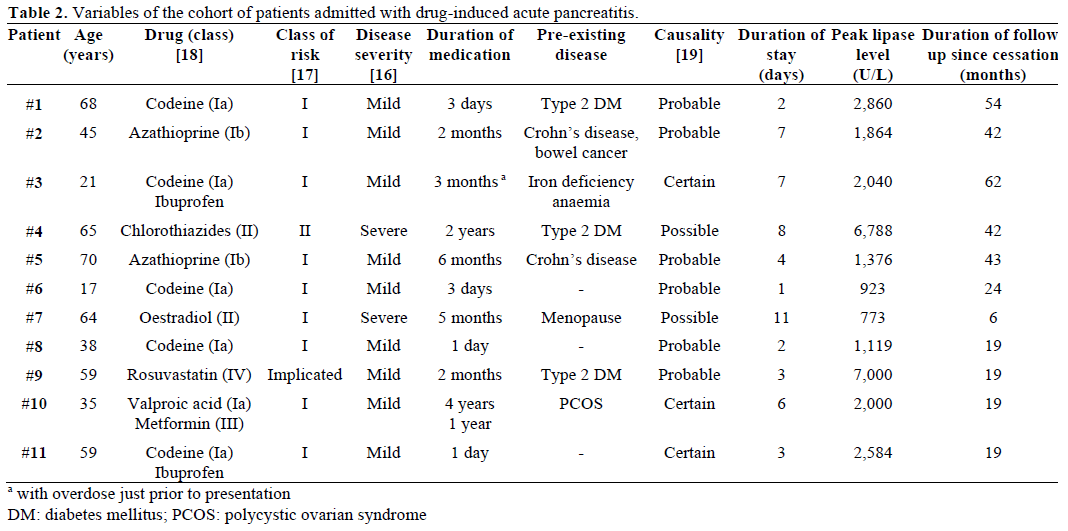
Nine of these 11 patients (81.8%) had a mild disease while 2 patients had severe acute pancreatitis with a median hospital stay of 4 days (range: 1-11 days). Three patients (Patient #1, #2 and #5; Table 2) had undergone a cholecystectomy prior to their presentation with the attack of acute pancreatitis.
Withdrawal of the drug resulted in cessation of the attacks in all patients with no further episodes of follow-up. The median follow-up in this series was 24 months (range: 6-62 months).
Drug Re-Challenge
Owing to the retrospective nature of the study, as well as for ethical reasons, a re-challenge could not be undertaken in all patients. However, failure to recognise the drug as a cause for the attack of acute pancreatitis resulted in an inadvertent re-challenge in 3 patients with a replication of the symptoms.
Patient #3 (Table 2) was admitted with mild acute pancreatitis following recent increase in the number of tablets consumed of a combination of codeine and ibuprofen for treating her migraines. At that time, the association was not considered significant. Six months later, when she restarted herself on codeine again for migraines, she developed another attack of acute pancreatitis necessitating admission. It was at this admission that the drug was recognised as the cause for acute pancreatitis.
Patient #10 (Table 2) was on valproic acid for treatment of her psychiatric problems for 4 years and was started on metformin for management of her polycystic ovarian syndrome disease. One year into the combination treatment, she presented with an attack of acute pancreatitis (confirmed on computed tomography scan) and metabolic acidosis. Recognising the potential of valproic acid to cause acute pancreatitis, the drug was ceased temporarily. However, in order to manage her psychiatric complaints, the drug was restarted resulting in the patient representing with acute pancreatitis one month later. At this time, the drug was permanently replaced by lithium.
Similarly, Patient #11 (Table 2) was admitted with mild acute pancreatitis following treatment with a combination medication of codeine and ibuprofen. At that time, the association was not considered significant. One year later, when prescribed the combination again for pain, she developed another attack of acute pancreatitis necessitating admission. It was at this admission that the drug was recognised as the cause for acute pancreatitis.
DISCUSSION
The incidence of acute pancreatitis is increasing around the world [20]. While alcohol and gallstones account for the most important aetiological factors [6, 7], the impact of other agents, such as prescribed drugs, is being increasingly appreciated owing to the accumulating evidence in published literature [9, 10, 17, 18]. Our study demonstrates an important role for prescription drugs in the causation of acute pancreatitis in Australian adults similar to a previous report in children [21]. The patients tended to be older females. Codeine was the drug most commonly associated with the causation of acute pancreatitis. Our study also indicates that biliary diseases and alcohol are the predominant causes of acute pancreatitis in Australia. Current understanding of drug-induced acute pancreatitis is largely based on case reports and critical reviews [11]. The importance of population-based studies in understanding this disease entity has been emphasized [11].
The incidence of drug-induced acute pancreatitis in our study of 3.4% compares with other large studies of drug-induced acute pancreatitis [12, 13, 14]. On comparing our results with these reports from Europe, drug-induced acute pancreatitis in our patients was more common in older patients (median age of 59 years) as compared to a mean age of 39-42 years noted in those studies [13, 14]. The female preponderance noted in our study appears to be similar to other studies.
Codeine, a class Ia drug associated with acute pancreatitis [18], caused an attack of acute pancreatitis in 5 patients in our series. The putative mechanisms by which codeine causes acute pancreatitis have been opined to be due to a spasm of the sphincter of Oddi [22]. Only one of these patients had had a prior cholecystectomy.
Two patients in our series were suffering from Crohn’s disease and following treatment with azathioprine (a class Ib drug), developed acute pancreatitis, necessitating a change of the drug. An immunemediated mechanism or a hypersensitivity to the drug is postulated in the pathogenesis of azathioprineinduced acute pancreatitis [23].
Although the effect of oestrogens on plasma triglycerides has been postulated as a potential mechanism for its causation of acute pancreatitis, our patient with acute pancreatitis secondary to oestradiol had normal triglyceride levels. The exact cause at this time is not clear but appears similar to a previous report [24] that suggested a different mechanism responsible for oestrogen-induced acute pancreatitis.
In the case of chlorothiazide-induced acute pancreatitis, the potential mechanisms involved in the causation of acute pancreatitis include thiazide-induced hyperparathyroidism, hypelipidaemia and hypercalcaemia or hypotension-inducing pancreatic ischaemia [25]. In the case of the patient reported in our series, neither hyperlipidaemia nor hypercalcaemia were noted. The duration of therapy to the occurrence of the acute pancreatitis has been variable and reported to be even up to 1 year [25].
Acute pancreatitis as a complication of valproic-acid therapy has been well documented in children [26]. The exact mechanism is unclear although idiosyncratic reactions have been postulated to be a cause [26]. Cases of acute pancreatitis developing even after 10 years of therapy have been reported [27].
The role of statins in the causation of acute pancreatitis has been well documented. There has been one prior case report of acute pancreatitis following treatment with rosuvastatin [28]. The exact mechanism responsible for the causation of acute pancreatitis by statins remains unclear.
CONCLUSIONS
Routine prescription drugs, as an aetiological factor, accounted for 3.4% of cases of acute pancreatitis. The disease appeared to be more common in middle-aged women. It is likely that the overall incidence of this entity is under-reported owing to the stringent criteria needed to conclusively determine a causal relationship.
Acknowledgements
The authors wish to acknowledge Martin Moyse, Heather Hills and Emma Venning for their assistance in the data collection
Sources of support
None
Grant support
Nil
Conflicts of interest
None declared
References
- Barreto SG, Rodrigues J. Comparison of APACHE II and Imrie Scoring Systems in predicting the severity of Acute Pancreatitis. World J EmergSurg 2007; 2:33. [PMID 18067678]
- Barreto SG, Rodrigues J. Acute pancreatitis in Goa - a hospitalbased study. J Indian Med Assoc 2008; 106:575-6. [PMID 19552084]
- Barreto SG, Bazargan M, Zotti M, Hussey DJ, Sukocheva OA, Peiris H, et al. Galanin receptor 3: a potential target for acute pancreatitis therapy. NeurogastroenterolMotil 2011; 23:e141-51. [PMID 21303427]
- Solanki NS, Barreto SG. Fluid therapy in acute pancreatitis. A systematic review of literature. JOP. J Pancreas (Online) 2011; 12:205-8. [PMID 21386654]
- Barreto SG, Jardine D, Phillips P, Bhatia M, Saccone GT. Can by-products in country-made alcohols induce acute pancreatitis? Pancreas 2010; 39:1199-204. [PMID 20531242]
- Barreto SG, Saccone GT. Alcohol-induced acute pancreatitis: the 'critical mass' concept. Med Hypotheses 2010; 75:73-6. [PMID 20181433]
- Toouli J, Brooke-Smith M, Bassi C, Carr-Locke D, Telford J, Freeny P, et al. Guidelines for the management of acute pancreatitis. J GastroenterolHepatol 2002; 17(Suppl.):S15-39. [PMID 12000591]
- Chiang DT, Anozie A, Fleming WR, Kiroff GK. Comparative study on acute pancreatitis management. ANZ J Surg 2004; 74:218- 21. [PMID 15043731]
- Ksiadzyna D. Drug-induced acute pancreatitis related to medications commonly used in gastroenterology. Eur J Intern Med 2011; 22:20-5. [PMID 21238888]
- Nitsche CJ, Jamieson N, Lerch MM, Mayerle JV. Drug induced pancreatitis. Best Pract Res ClinGastroenterol 2010; 24:143-55. [PMID 20227028]
- Tenner S. Drug-induced acute pancreatitis: underdiagnosis and overdiagnosis. Dig Dis Sci 2010; 55:2706-8. [PMID 20686844]
- Andersen V, Sonne J, Andersen M. Spontaneous reports on drug-induced pancreatitis in Denmark from 1968 to 1999. Eur J ClinPharmacol 2001; 57:517-21. [PMID 11699619]
- Lankisch PG, Dröge M, Gottesleben F. Drug induced acute pancreatitis: incidence and severity. Gut 1995; 37:565-7. [PMID 7489946]
- Vinklerova I, Prochazka M, Prochazka V, Urbanek K. Incidence, severity, and etiology of drug-induced acute pancreatitis. Dig Dis Sci 2010; 55:2977-81. [PMID 20499176]
- Banks PA, Freeman ML. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID 17032204]
- Bradley EL 3rd. A clinically based classification system for acute pancreatitis. Summary of the International Symposium on Acute Pancreatitis, Atlanta, Ga, September 11 through 13, 1992. Arch Surg 1993; 128:586-90. [PMID 8489394]
- Trivedi CD, Pitchumoni CS. Drug-induced pancreatitis: an update. J ClinGastroenterol 2005; 39:709-16. [PMID 16082282]
- Badalov N, Baradarian R, Iswara K, Li J, Steinberg W, Tenner S. Drug-induced acute pancreatitis: an evidence-based review. ClinGastroenterolHepatol 2007; 5:648-61. [PMID 17395548]
- Edwards IR, Aronson JK. Adverse drug reactions: definitions, diagnosis, and management. Lancet 2000; 356:1255-9. [PMID 11072960]
- Lowenfels AB, Maisonneuve P, Sullivan T. The changing character of acute pancreatitis: epidemiology, etiology, and prognosis. CurrGastroenterol Rep 2009; 11:97-103. [PMID 19281696]
- Nydegger A, Heine RG, Ranuh R, Gegati-Levy R, Crameri J, Oliver MR. Changing incidence of acute pancreatitis: 10-year experience at the Royal Children's Hospital, Melbourne. J GastroenterolHepatol 2007; 22:1313-6. [PMID 17489962]
- Hastier P, Buckley MJ, Peten EP, Demuth N, Dumas R, Demarquay JF, et al. A new source of drug-induced acute pancreatitis: codeine. Am J Gastroenterol 2000; 95:3295-8. [PMID 11095359]
- Pitchumoni CS, Rubin A, Das K. Pancreatitis in inflammatory bowel diseases. J ClinGastroenterol 2010; 44:246-53. [PMID 20087199]
- Blake WE, Pitcher ME. Estrogen-related pancreatitis in the setting of normal plasma lipids: case report. Menopause 2003; 10:99- 101. [PMID 12544683]
- Bedrossian S, Vahid B. A case of fatal necrotizing pancreatitis: complication of hydrochlorothiazide and lisinopril therapy. Dig Dis Sci 2007; 52:558-60. [PMID 17219076]
- Sinclair DB, Berg M, Breault R. Valproic acid-induced pancreatitis in childhood epilepsy: case series and review. J Child Neurol 2004; 19:498-502. [PMID 15526953]
- Tobias JD, Capers C, Sims P, Holcomb GW 3rd. Necrotizing pancreatitis after 10 years of therapy with valproic acid. ClinPediatr (Phila) 1995; 34:446-8. [PMID 7586914]
- Singh S, Nautiyal A, Dolan JG. Recurrent acute pancreatitis possibly induced by atorvastatin and rosuvastatin. Is statin induced pancreatitis a class effect? JOP. J Pancreas (Online) 2004; 5:502-4. [PMID 15536291]

