Amit Bahl1*, Rakesh Kapoor1, Parsee Tomar1, Oinam Arun Singh1, Rajesh Gupta2 and Suresh C Sharma1
1Department of Radiation Oncology, Post Graduate Institute of Medical Education and Research (PGIMER). Chandigarh, India
2Department of Surgery, Post Graduate Institute of Medical Education and Research (PGIMER). Chandigarh, India
- *Corresponding Author:
- Amit Bahl
Department of Radiation Oncology and Regional Cancer Center
Post Graduate Institute of Medical Education and Research (PGIMER)
Sector 12; Chandigarh, 160012; India
Phone +91-887.201.6102
Fax +91-172.274.4401
E-mail dramitbahl@yahoo.com
Received September 11th, 2012 – Accepted October 15th, 2012
Keywords
Pancreatic Neoplasms; Radiotherapy; Radiotherapy, Conformal; Radiotherapy, Intensity-Modulated
Abbreviations
3DCRT: 3D conformal radiotherapy; CTV: clinical target volume; DVH: dose volume histogram; intensity modulated radiotherapy; PTV: planning target volume
INTRODUCTION
Periampullary cancers include tumors arising from ampullary, pancreatic, bile duct and duodenal regions. These tumors lie within 1 cm of the ampulla of Vater [1, 2]. The exact incidence of these tumors is not well documented as they are clubbed with pancreatic cancers for treatment. The incidence and mortality of pancreatic cancers is better documented with 35,240 deaths reported in the United States in 2009. Pancreatic cancer is one of the sites where survival has not improved in last 30 years [3]. The prognosis of periampullary cancers though better than pancreatic body cancers, still remains poor. Majority of periampullary cancers patients present with operable tumors. Treatment involves Whipples surgery followed by adjuvant radiotherapy and chemotherapy. Postoperative radiotherapy is particularly useful in managing high risk patients (tumors involving the pancreas, poorly differentiated histology, involved lymph nodes and positive margins). Postoperative radiotherapy doses of 40-50 Gy using conventional radiotherapy have been used in treatment of these patients [4]. The common cause of treatment failure in these patients is recurrence in the tumor bed, regional lymph nodes and liver metastasis. A treatment approach aiming to increase the local control rate, by escalating radiation dose is likely to decrease locoregional failures and translate into a better survival. Few recent trials are now focusing on dose escalation using conformal radiation techniques [5, 6]. The purpose of the present study was to do a dosimetric analysis of the doses received by organs at risk in postoperative radiotherapy using a dose of 45Gy in 25 fractions and to assess the feasibility of radiation dose escalation.
METHODS
Study Design and Setting
This dosimetric analysis was carried out at the Department of Radiotherapy at Post Graduate Institute of Medical Education and Research, Chandigarh, India, which is a multispecialty tertiary care referral center.
Radiotherapy Planning
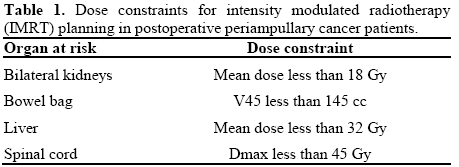
Ten postoperative patients of periampullary cancers were selected for this dosimetric analysis comparing doses to organs at risk using 3D conformal radiotherapy (3DCRT) versus intensity modulated radiotherapy (IMRT). All patients had undergone Whipple’s surgery. Planning CT scans films were taken for the patients with proper immobilization using a multislice CT scanner with slice thickness of 2.5 mm using a multislice CT scanner (GE Healthcare Technologies, Wankesha, WI, USA). The images were transferred to EclipseTM treatment planning system (v.8.6, Varian Associates, Palo Alto, CA, USA). Conturing for treatment volumes was done as per published Radiotherapy and Oncology Group (RTOG) guidelines [7]. The clinical target volume (CTV) included the postoperative tumor bed and draining lymph nodal areas. A 1 cm margin was taken around the CTV to generate the planning target volume (PTV). Critical structures contoured for evaluation included bowel bag, bilateral kidneys, liver, stomach and spinal cord. Two sets of IMRT and 3DCRT plans were generated for each patient. IMRT plans were generated using seven field coplanar beams and 3DCRT planning was done using one anterior and two lateral fields (Figures 1 and 2). A dose of 45 Gy in 25 fractions was prescribed to the planning target volume in both treatment groups. Six MV photons were used for all treatment planning. The plans were optimized to deliver 45 Gy in 25 fractions to the PTV and the optimization was constrained to deliver the prescription dose to greater than 95% of the PTV. Dose volume histograms were generated for all the organs at risk. The dose constraints used for IMRT treatment planning are listed in Table 1. Dosimetric evaluation of doses to organs at risk was done using quantitative analysis of normal tissue effects in clinics (QUANTEC) parameters [8].
Figure 1. Three field 3D conformal radiotherapy (3DCRT) for
treating periampullary cancers.
Figure 2. Intensity modulated radiotherapy (IMRT) fields for
periampullary cancers.
ETHICS
Oral informed consent was obtained from patients for this dosimetric analysis and study conforms to the ethical guidelines of the "World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. The IRB approval was not collected because this study was a dosimetric analysis only and it did not involve any actual patient treatments under the study.
STATISTICS
For statistical analysis the data was arranged in Statistical Program for Social Sciences (SPSS version 18). Descriptive data analysis was conducted for the dosimetric data. Summary statistics including mean, standard deviation and range were obtained in both techniques. A paired t-test was used to compare the average doses between the study groups. A two-tailed P value of less 0.05 was considered significant.
RESULTS
Dose to the bowel bag was less using IMRT versus 3DCRT with a V45 of 80.9±57.4 cc versus 212.3±159.0 cc (P=0.033) (Figure 3). The mean doses to the liver, stomach, spinal cord, right kidney and left kidney using 3DCRT and IMRT are shown in Table 2. The dose volume histogram (DVH) comparing the two techniques is shown in Figure 4. The V28 dose analysis for bilateral kidneys showed a mean volume of 32.7±23.5 cc versus 7.9±7.4 cc for 3DCRT versus IMRT (P=0.013) (Figure 5). The V20 for bilateral kidneys showed a mean volume of 45.9±27.7 cc versus 42.4±32.5 cc for 3DCRT versus IMRT, respectively (P=0.821). The D60 for liver using 3DCRT and IMRT was 28.4±8.6 Gy and 19.9±3.2 Gy, respectively (P=0.020) (Figure 6).The V30 analysis for liver showed a mean volume of 592.5±218.6 cc versus 338.0±139.7 cc for 3DCRT versus IMRT, respectively (P=0.015) (Figure 7).
Figure 3. Box plot showing V45 for bowel bag using 3D conformal radiotherapy (3DCRT) versus intensity modulated radiotherapy
(IMRT) (P=0.033).
Figure 4. Dose volume histogram (DVH) comparing doses to organs at risk between intensity modulated radiotherapy (IMRT) and 3D conformal
radiotherapy (3DCRT). (Squares represent 3DCRT and triangles represent IMRT).
Figure 5. Box plot showing V28 bilateral kidneys using 3D
conformal radiotherapy (3DCRT) versus intensity modulated
radiotherapy (IMRT) (P=0.013).
Figure 6. Box plot showing D60 liver using 3D conformal
radiotherapy (3DCRT) versus intensity modulated radiotherapy
(IMRT) (P=0.020).
Figure 7. Box plot showing V30 liver using 3D conformal
radiotherapy (3DCRT) versus intensity modulated radiotherapy
(IMRT) (P=0.015).

DISCUSSION
A review of the pattern of recurrences in periampullary and pancreatic cancers show that local recurrences contribute significantly to treatment failures. Tepper et al. reported a 50% local recurrence rate in operated pancreatic cancers [9]. In a retrospective analysis of 118 patients with carcinoma of the ampulla of Vater Kim et al. reported a 17% overall locoregional failure rate using a radiation dose of 40 Gy in 2 Gy fractions with a planned treatment break. They showed that adjuvant chemoradiation may enhance locoregional control and overall survival after curative resection, especially in those with nodal involvement [10]. Kayahara M et al. reported a postoperative local recurrence rate of 80% and lymph nodal recurrence of 47% in 45 patients of head of pancreas cancer undergoing surgery [11]. Yovinio et al. showed a locoregional failure rate of 19% in resected pancreatic cancers using IMRT with a median dose of 50.4 Gy (range: 50.4-59.4 Gy) [8]. Higher T stage (T3, T4) is an adverse prognostic factor in ampullary cancers and adjuvant chemoradiotherapy has shown benefit in overall survival in these patients (median survival 35.2 versus 16.5 months, P=0.06) [5]. Postoperative high risk features for periampullary cancers includes high tumor grade, positive nodes, positive margins and pancreatic invasion. These patients benefit from adjuvant therapy and have better 5-year survival rate compared to surgery alone (83% versus 50%) [12].
The presence of surrounding organs at risk, like bowel, liver, kidneys, stomach and spinal cord, limits the delivery of radiation doses to the postoperative tumor bed. Radiation doses of 40 to 50 Gy have been used in conventional radiotherapy [12]. With improved radiotherapy delivery techniques, like intensity modulated radiotherapy (IMRT), the doses to surrounding organs at risk can be controlled and radiation doses escalated in the tumor bed and nodal areas. IMRT has been successfully implemented in other gastrointestinal tract malignancies with encouraging results reported in anal canal cancer and esophageal cancers [13, 14].
There are a few reports of use of IMRT in pancreatic and ampullary cancers with doses up to 60 Gy which have shown significant decrease in doses received by small bowel [7, 15]. Brown et al. evaluated integrated boost IMRT with dose escalation up to 64.8 Gy with a superior dose distribution in organs at risk as compared to IMRT and 3DCRT [16]. Bouchard et al. correlated pancreatic tumor location to modality for radiation dose escalation and found that IMRT allows more conformal dose escalation in high dose region and proton therapy reduces low dose region to organs at risk [17]. Geld et al. found no significant additional dose reduction to organs at risk using 4D CT based respiratory gated treatment plans over IMRT plans [18].
Dose escalation is likely to impact local control and translate to an improved survival rate. The profiles of doses received by organs at risk in our analysis are well within the prescribed limits and leave ample scope of dose escalation.
CONCLUSIONS
Conventional postoperative radiotherapy protocols have treated periampullary cancers with doses ranging from 40 to 50.4 Gy with a median dose of 40 Gy in many studies. Few recent trials have addressed the issue of dose escalation. Our results show that with a commonly dose schedule of 45 Gy in 25 fractions the dose to bowel bag is significantly reduced using IMRT compared to 3DCRT. The doses received by other organs are lower with IMRT compared to 3DCRT with significant differences in doses received in liver and kidneys. The profile of doses received by organs at risk leaves ample scope of dose escalation in postoperative patients using IMRT. We propose dose escalation up to 60 Gy in conventional fractionation for postoperative periampullary cases presenting with high risk features. Further studies will be required to evaluate long term impact of such a dose escalation.
Conflict of interest
The authors have no potential conflict of interest
References
- Offerhaus GJ, Giardiello FM, Krush AJ etal.The risk of upper gastrointestinal cancer in familial adenomatous polyposis. Gastroenterology 1992; 102:1980-82. (PMID:1316858)
- Jagelman DG, DeCosse JJ, Bussey HJ. Upper gastrointestinal cancer in familial adenomatous polyposis .Lancet 1988; 1:1149-51.(PMID:2896968)
- Jemal A, Siegal R, Ward E et al. Cancer statistics 2009. Ca Cancer J Clin 2009;59:225-49. (PMID:19474385)
- Krishnan S, Rana V, Evans DB et al. Role of adjuvant chemoradiation therapy in adenocarcinomas of the ampulla of vater. Int.J. Radiation Oncol Biol Phys 2008;70:735-43. (PMID:17980502)
- Yovino S, Poppe M, Jabbour S etal.Intensity modulated radiation therapy significantly improves acute gastrointestinal toxicity in pancreatic and ampullarycancers.Int.J. Radiat Oncol Biol Phys 2011; 79:158-62. PMID:20399035
- YovinoS,Maidment BW, Herman JM et al. Analysis of local control in patients receiving IMRT for resected pancreatic cancers. Int.J. Radiat Oncol Biol Phys 2011. PMID:22284684
- Goodman KA, Regine WF, Dawson LA etal.Radiation therapy oncology group consensus panel guidelines for the delineation of the clinical target volume in the postoperative treatment of pancreatic head cancer. Int J Radiat Oncol Biol Phys. 2012 Jul 1;83(3):901-08. PMID: 22483737
- Marks LB,YorkeED,Jackson A et al.Use of normal tissue complication probability models in the clinic. Int J Radiat Oncol Biol Phys. 2010;76:s10-s19. PMID:20171502
- Tepper J, Nardi G, Suit H. Carcinoma of the pancreas: Review of the MGH experience from 1963 to1973. Cancer 1976;37:1519-24. PMID:1260670
- Kim K, Chie EU,Jang JY et al. Role of adjuvant chemoradiotherapy for ampulla of vater cancer. Int.J. Radiat Oncol Biol Phys 2009; 75:436-41. PMID:19394162
- KaayaharaM,Nagakwa T, Ueno K et al.An evaluation of radical resection for pancreatic cancer based on mode of recurrence as determined by autopsy and diagnostic imaging.Cancer1993;72:2118-23. PMID:8104092
- WilletCG, Warshaw AL, Convery K, et al. Patterns of failure after pancreaticoduodenectomy for ampullary carcinoma. Surg Gynecol Obstet. 1993;176:33– 38.
- Kachnic LA, Tsai HK, Coen JJ et al. Dose-painted intensitymodulatedradiation therapy for anal cancer: a multi-institutional report of acute toxicity and response to therapy. Int J Radiat Oncol Biol Phys. 2012;82:153-58. PMID:21095071
- Welsh J, Palmer MB, Ajani JA et al. Esophageal cancer doseescalation using a simultaneous integrated boost technique Int J Radiat Oncol Biol Phys. 2012;82:468-74. PMID:21123005
- Landry JC, Yang GY, Ting JY et al. Treatment of pancreatic cancer tumors with intensity-modulated radiation therapy (IMRT) using the volume at risk approach (VARA): employing dose-volume histogram (DVH) and normal tissue complication probability (NTCP) to evaluate small bowel toxicity. Med Dosim 2002;27:121–29. PMID:12074463
- Brown MW, Ning H, AroraB, et al. Adosimetric analysis of dose escalation using two intensity-modulated radiation therapy techniques in locally advanced pancreatic carcinoma. Int J Radiat Oncol Biol Phys. 2006 May 1;65(1):274-83. PMID: 16618582
- Bouchard M, Amos RA, Briere TM, Beddar S, Crane CHDoseescalation with proton or photon radiation treatment for pancreatic cancer. Radiother Oncol. 2009 ;92:238-43. PMID:19454367
- van der Geld YG, van Triest B, Verbakel WF et al. Evaluation of four-dimensional computed tomography-based intensitymodulatedand respiratory-gated radiotherapy techniques for pancreatic carcinoma. Int J Radiat Oncol Biol Phys. 2008 Nov 15;72(4):1215-20. PMID:18954715








