Keywords
access and evaluation, healthcare quality,
outcome and process assessment, patient care
planning, primary health care
Introduction
Demographic changes in Western society are generating
a growing number of people with chronic
diseases and co-morbidity needing long-term care from different caregivers in complex care situations.
Moreover, a growing number of people needing
complex care, such as people with dementia, are being cared for at home.[1] It is important to ensure quality of
care in these complex home care situations. Although
there has been interest for quality in home care for
decades,[2–4]more critical research in this field is required
and to date it has received little attention and discussion.
[5,6]Discussions about quality of care have proved
difficult because of the wide range of definitions used.
The most basic definition states that quality of care can
be measured by the client’s satisfaction.[7] The Institute
of Medicine covers items such as efficiency, efficacy,
continuity of care and safety.[8] These items have also
been included in Flemish lawwhen referring to quality
of care. Donabedian and Campbell argue that quality
is related to structures, processes and outcome of
health care, based both at the individual and the
population level, and that efficacy and availability
should be taken into account.[9,10]
The organisation of care in Flanders is complex.[11]
Both the federal and regional governments have jurisdiction
and provide financial resources. Different
disciplines, involved in the care for the same patient,
are organised and financed in different ways. Historically,
there have been different trends in the northern
part of Belgium (Flanders) and the southern (Wallonia).
Because patients can choose healthcare professionals
freely, home care teams are very variable. To ensure
integrated care, a system of subsidised care plans was
developed some 15 years ago, stipulating norms and
finances for multidisciplinary teams. If coordination
of care is needed, the patient or one of the caregivers in
the team can initiate a care plan involving all caregivers.
A multidisciplinary team consists of at least
three caregivers, including a general practitioner and
one or more professionals.
A literature search of several databases (including
Medline, CINAHL, BNI, PsychINFO and ISI Citation
Indexes) provided 6044 articles about patient care
planning, of which 179 were selected based on title
and abstract. Most papers were in the form of expert
opinions. Only 12 articles dealt with the impact of a
care plan.[12–23] Moreover, studies in which the effect of
a care plan was analysed did not consider home care.[24]
Different studies used different definitions of a care
plan.[25–28] An unambiguous definition is needed. Since
this study was limited to Flanders, care plans were
defined according to Flemish legislation: care plans
are multidisciplinary plans intended to provide care
which improves the independence and functioning of
the patient and supports the (formal and informal)
caregivers involved. Flemish legislation considers care
plans as a written communication tool between all
involved. Care plans include identification of the
patient and the caregivers involved, a description of
the caregivers’ tasks, arrangements for care and an
evaluation of the patient’s situation. Each care plan,
developed in accordancewith the legislation, is funded by the regional government,with a maximum funding
per region for three per 1000 inhabitants.
The aim of this study was to investigate whether
care plans have a significant effect on the perceived
quality of home care according to the patients, family
caregivers and healthcare professionals involved.
Methods
A multicentre, non-randomised control group design
was used to measure the differences in the perceived
quality of care in situations with and without a care
plan. From each of the five provinces of Flanders, one
region in which the funded care plans were used to
organise complex care situations was included in our
study as an intervention region. In these intervention
regions, care situations with registered care plans were
selected. To select control regions in each of these five
provinces, a region in which care plans were not used
was selected. Only in three provinces did a regionmeet
this selection criterion. Nursing care plans of all
patients meeting the criteria of the funded care plans
in 2005 were included. All those involved in the selected
care plans, patients, family caregivers and healthcare
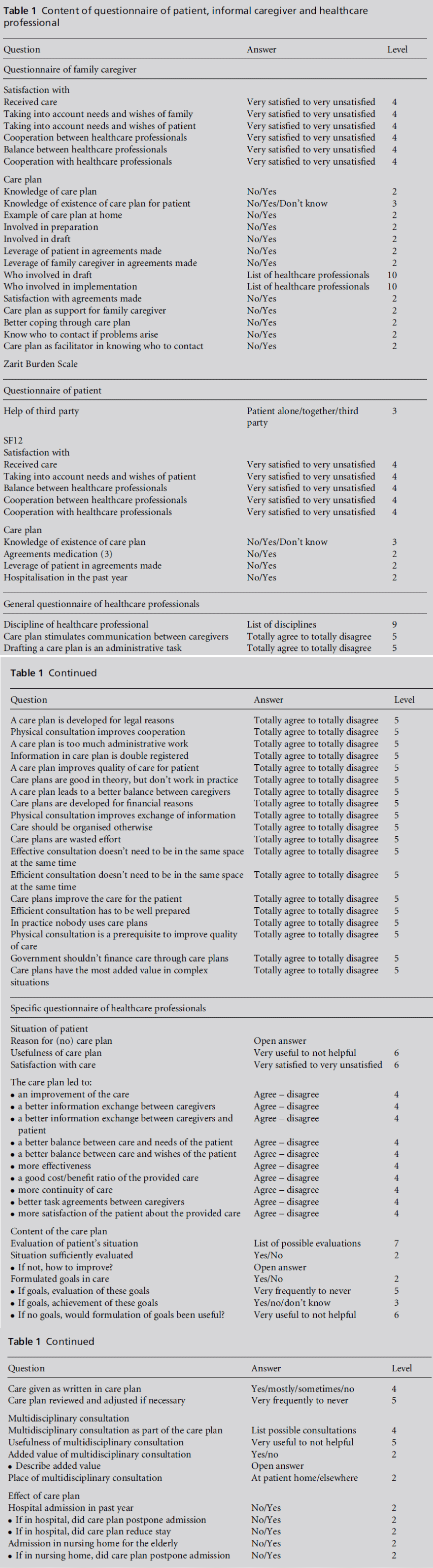
professionals, received a postal questionnaire (Table 1).
The postal questionnaires contained indicators of
the different concepts of quality of care: satisfaction;
structure, process and outcome; and items relating to
efficacy, efficiency, cost-effectiveness and continuity
of care. These indicators were also covered by the local
legislation about quality of care standards.[8] The structure
and availability of services was studied by interviewing
stakeholders in the selected regions. The results
of these interviews are reported elsewhere.[29]
Patient questionnaire
The patient questionnaire measured satisfaction and
registered hospitalisation. Global health functioning
was measured with the SF12.[30,31] Because the patients
being questioned were elderly, they could choose to fill
in the questionnairewith the help of a third party. This
was indicated on the questionnaire.
Informal caregivers’ questionnaire
The informal caregivers involved (family members,
friends, neighbours) identified in the care plans received
a questionnaire with outcome quality items, namely
satisfaction, and the Zarit Burden Scale, measuring the
degree of burden caused by the caring process.[32,33]
Healthcare professionals’
questionnaire
The healthcare professionals involved were invited to
fill in two written questionnaires: one with 21 general
statements about the care plan and multidisciplinary
meetings and another covering quality items related to
the patient’s specific care plan.
An informed consent form was signed according to
the current regulations.[34] The protocol was approved
by the Ethics Committee of the Faculty of Medicine,
Katholieke Universiteit Leuven.
Before the study a formal power calculation was
done with Epi-Info1. For a score of 25%, a difference
of 15% and a response rate of 50%, a minimumof 330
care plans in each group was estimated to be needed.
Data were imported into an Access database and
analysed with SAS V8. All data from the intervention
regions were analysed against all data from the control
regions. Data were calculated in proportions. Contingency
tables were evaluated by the chi-square test. A
value ofP<0.05was considered significant.ABonferroni
correction was used to adjust for multiple testing.
Results
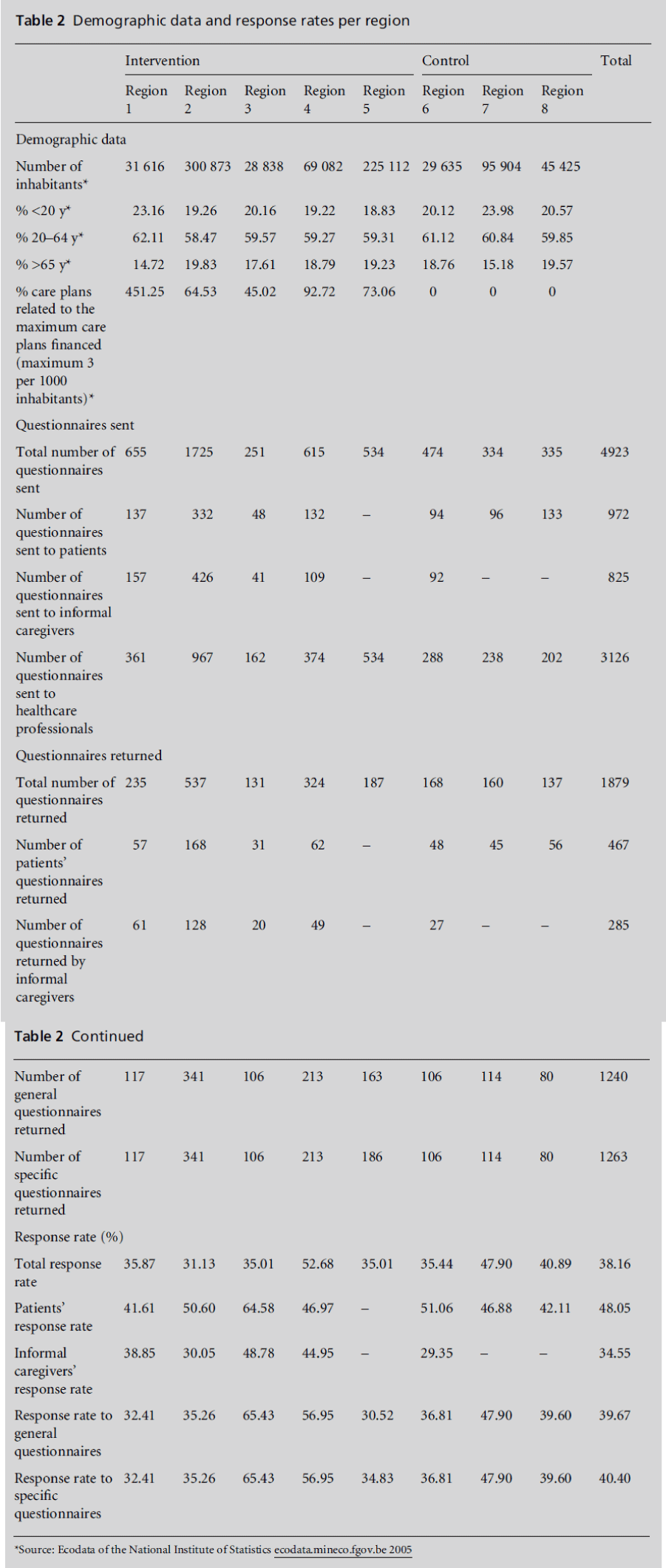
Demographic data
A comparison of intervention versus control regions
yielded relatively similar populations. However, there
were large differences in the use of funded care plans in
the intervention regions, ranging from 45.02% to 451.25%
of the maximum financed care plans (Table 1). In the intervention regions 1022 funded care plans were
selected. In the control regions the selection consisted
of 323 nursing care plans. Due to privacy agreements,
the information from patients in one region was not
registered. In three regions information on the informal
caregiver had not been registered. In these regions
the patients and informal caregivers could not be
questioned. In total, 1879 of the 4923 questionnaires
sent were returned, representing a total response rate
of 38%.
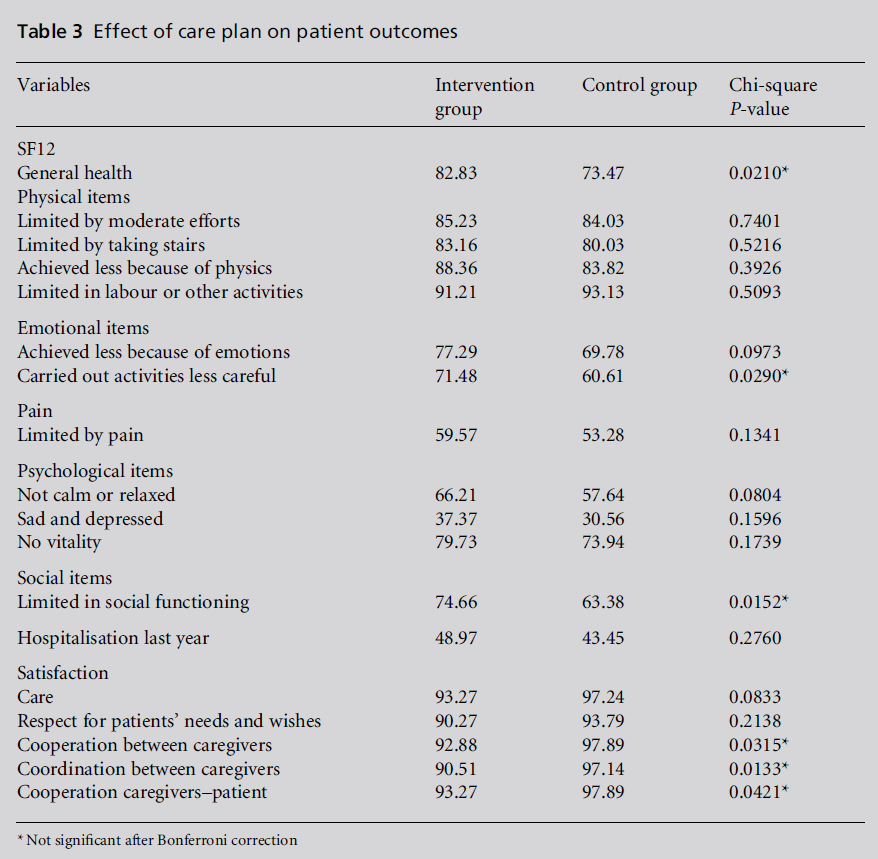
Patient questionnaire (n=972)
A total response rate of 48.1% (n=467) was achieved
(Table 2). Only 18.3% of patients completed the
questionnaire themselves; 53.3% received assistance
from an informal caregiver and in 28.4% of cases the
informal caregiver had completed it.
There were no significant differences between the
intervention and the control groups in satisfaction
with the involvement, coordination and cooperation.
A care plan had no effect on the number of registered
hospitalisations during the last year or on patients’
global functioning measured with the SF12 (Table 3).
Informal caregivers’ questionnaire
(n=825)
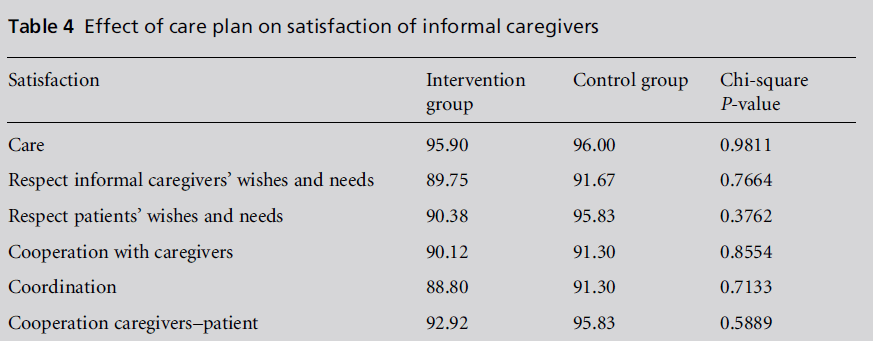
The research team received 34.6% completed questionnaires
from informal caregivers (n=285). No differences
between the intervention and control groups
were found in the satisfaction of informal caregivers
with care, in the involvement of patient and informal
caregiver and in the coordination and cooperation
between professionals and with the informal caregiver (Table 4). Most informal caregivers experienced a high
burden of care, measured with the Zarit Burden Scale
(90.4% scoring >10). There was no significant difference
between the control and intervention groups
(P=0.7).
Healthcare professionals’ general
questionnaire (n=3126)
The general questionnaire was completed by nurses
(32.8%), GPs (31.2%), social workers (11.4%), home
care providers (4.5%) and others (20.0%) with a
global response rate of 39.7% (n=1240; Table 2). For
six out of the 21 items the outcome was significantly
different in the intervention group compared with the
control group.
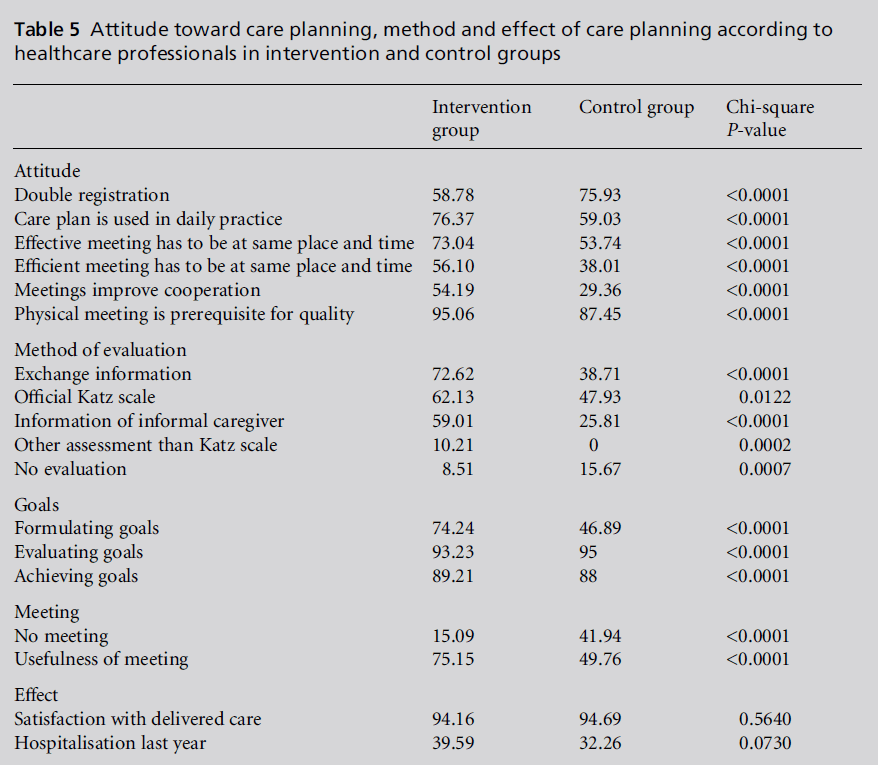
Healthcare professionals in the control group
perceived significantly more double registrations of
information in the care plan. Healthcare professionals
who had already used care plans, responded significantly
more often that care plans were used in practice.
They also agreed that for meetings to be efficient and
effective all healthcare professionals involved should
meet at the same place and at the same time.Moreover, significantly more healthcare professionals from the
intervention group agreed that multidisciplinary
meetings improved cooperation and were a prerequisite
for high quality care (Table 5). Further analyses
showed that the more experienced the people in multidisciplinary
teams, the more they were convinced of
the quality improving effect of team meetings.
Healthcare professionals’ questionnaire
related to specific care plan (n=3126)
Of the questionnaires related to a specific care plan
situation, 1263 (40.4%)were returned (Table 2).Most
healthcare professionals questioned in both the intervention
and control groups indicated that the care
situation was sufficiently evaluated (88.1% and 86.5%
respectively). However, there was a significant difference
in the method of evaluation. The intervention
group evaluated significantly more often by means of
information exchange, gathering information from
the informal caregivers and using assessment other
than the official dependency scale to measure the
patient’s care needs. Significantly more healthcare professionals in the control group stated that the care
situation was not evaluated (Table 5).
There was a significant difference between intervention
and control regions concerning the formulation,
evaluation and achievement of goals. In the intervention
group goals were more frequently formulated and achieved. Healthcare professionals in the control
group stated more often that formulated goals are
evaluated.
The healthcare professionals inthe intervention group
met significantly more other professionals involved in
the same care situation in person and had a more positive attitude about the usefulness of team meetings
than those in the control group. According to
healthcare professionals from both the intervention
and the control groups, the main added value of team
meetings was the interdisciplinary contact, the collaboration
and the coordination of care.
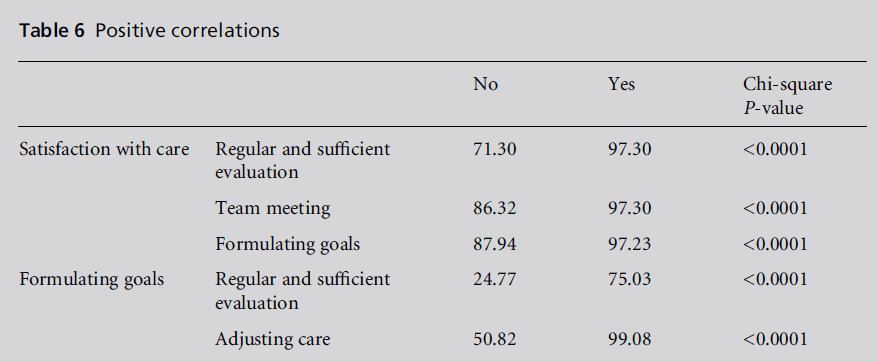
Overall, the satisfaction of healthcare professionals
about the care delivered did not differ significantly
between control and intervention groups. However,
there was a positive correlation between the satisfaction
with care delivered and regular and sufficient
evaluation of the care situation, team meetings and
formulation of goals. The more healthcare professionals
indicated that they had formulated goals, the
more they perceived that the care was sufficiently
evaluated and the more they evaluated and adjusted
the care (Table 6).
As to the effect of the care plan, the number of
patient hospitalisations registered by healthcare professionals
did not differ significantly between intervention
and control groups (Table 5).
Discussion
Main findings
The caring process in situations with home care plans
differs significantly with respect to the formulation
and achievement of goals from those without care
plans. Moreover, healthcare professionals in the intervention
group participated significantly more often
in team meetings, had a more positive attitude towards
these and considered them as a prerequisite for the
quality of care. There was a positive correlation between
satisfaction on the one hand, and regular and sufficient
evaluation, team meetings and formulation of
goals on the other.
Nonetheless, there was no significant effect on the
measured outcome, namely the satisfaction of all
involved, on registered hospitalisations, on perceived
general health of the patient and on the experience of
burden of the informal caregiver.
Comparison with previous literature
Previous international literature emphasises the formulation
of care goals as a crucial element in the
development of a care plan.[25–28] From our study it can
be concluded that the formulation of care goals, the
evaluation of these goals and better communication
between healthcare professionals are crucial in providing
adequate home care. A care plan stimulates
these elements.
A face-to-face meeting with all healthcare professionals
involved at the same place at the same time is
very valuable. Nonetheless, healthcare professionals
emphasise that it is not feasible to participate in a
multidisciplinary meeting for every patient. Meetings
should be organised only if useful. In a study in Flanders
about views concerning team meetings, GPs described
these to be useful in terms of being purposeful meetings
with time well spent on concrete items that needed
work and attention, providing GPs with the opportunity
to get to know the other professionals, having a
commitment to improving care and having the involvement
of both patients and informal caregivers.[35]
Moreover, GPs who had positive experiences with
team meetings acknowledged the added value of this
activity. Our results confirm the findings of this study.
Quality of care is often misunderstood as satisfaction.
This study uses a multilevel concept of quality of
care taking into account perceptions and views of all
those involved, and compares them with those from a
control group. Moreover, to measure functional outcome
the Zarit Burden Scale and SF12 were integrated
in the questionnaires. The results of this quantitative
study were confirmed by the results of the interviews
with healthcare professionals from the selected regions.
These data can be important for policy makers, to help
them optimise the system.
Against a background of scarce previous research,
this study establishes that, in a given healthcare system,
implementing care plans and organising home
care teams is beneficial for those in need of home care.
Even in studies covering a clearly defined clinical area
such as diabetes care, no important differences were
detectable.[36] Also, in a randomised controlled trial
studying the possible benefit of dementia medication,
no proven benefits in hard end points were shown.[37]
Limitation of this study
The data collection was difficult. In many regions data
were recorded on paper instead of digitally. Handwriting
sometimes had to be deciphered and not all
data were complete. Many strategies were used to
complete the data.
Using care plans in home care is regarded as a
complex intervention, with many factors influencing
the care process. Despite existing legislation in Flanders,
practice in primary care is diverse.29 In order to control
for this diversity an intervention and control region
were selected in every province. Nevertheless, only
three provinces in each region met the selection criteria.
Moreover, because of the variation in numbers of care
plans, some regions gained more weight in the results.
Owing to privacy reasons, one region did not
register the data of the patients. In three regions the
data of informal caregivers were not available. It was not possible to retrieve these data. The response rate
could also have been better. Owing to time pressure on
the sponsor it was not possible to send participants a
reminder. Therefore the number of care plans obtained
was sufficient for the healthcare professionals, but
insufficient for patients and informal caregivers. If
the required number of care plans were achieved for
these groups the results would have been more valid.
This study was performed in Flanders. The results
can be generalised to other healthcare systems with
variable teams in complex home care situations. In
Flanders every team is organised on an ad hoc basis as
a result of the freedom of choice of professional
caregivers by patients and their relatives. We are in
doubt as to what the result would have been if fixed
teams had been questioned. Experiences in Canada
teach us that in order to hold a chaotic world together
clustered care is needed rather than very complex
structures.[38–41] The Dutch Health Council states that
primary care is essentia1.[42–44] In Belgium, there is
growing evidence that coordinated care generates a
better outcome.45 Given the growing need for home
care, in-depth research is required to learn more about
the most effective and high-quality way to care for
people at home.
References
- Alzheimer Europe. Dementia in Europe. Yearbook 2006.
Luxembourg: Alzheimer Europe, 2006.
- Hughes S, Weaver F, Giobbie-Hurder A et al. Effectiveness
of team-managed home-based primary care.
Journal of the American Medical Association 2000;284:
2877–85.
- Beswick AD, Rees K, Dieppe P et al. Complex interventions
to improve physical function and maintain
independent living in elderly people: a systematic review
and meta-analysis. The Lancet 2008;371:725–35.
- Landi F, Onder G, Tua E et al. Impact of a new
assessment system, the MDS-HC, on function and
hospitalization of homebound older people: a controlled
clinical trial. Journal of the American Geriatrics
Society 2001;49:1288–93.
- McMurdo ME and Witham MD. Health and welfare of
older people in care homes. BMJ 2007;334:913–14.
- Edwards N and Lang A. Importance of the home care
sector and the critical need for research on home care.
Canadian Journal of Nursing Leadership 2007;20:4–5.
- Harteloh P and Casparie A. Kwaliteit van Zorg: van een
zorginhoudleijke benadering naar een bedrijfskundige
aanpak. Den Haag, Lochum: VUGA/De Tijdstroom
1991.
- Institute of Medicine. Measuring the Quality of Health
Care. Washington, DC: National Academy Press, 1999.
- Donabedian A. The quality of care. How can it be
assessed? Archives of Pathology and Laboratory Medicine
1997;121:1145–50.
- Campbell SM, Roland MO and Buetow SA. Defining
quality of care. Social Science and Medicine 2000;51:
1611–25.
- De Lepeleire J, Falez F, Ylieff M, Fontaine O, Paquay L
and Buntinx F. The evolution of the organization of
homecare in Flanders, Wallonia and Brussels. Archives of
Public Health 2004;62:197–208.
- Newcomer R, Maravilla V, Faculjak P and Graves MT.
Outcomes of preventive case management among highrisk
elderly in three medical groups: a randomized
clinical trial. Evaluation and the Health Professions
2004;27:323–48.
- Segal L, Dunt D, Day SE, Day NA, Robertson I and
Hawthorne G. Introducing co-ordinated care (1): a
randomised trial assessing client and cost outcomes.
Health Policy 2004;69:201–13.
- Ferguson JA and Weinberger M. Case management
programs in primary care. Journal of General Internal
Medicine 1998;13:123–6.
- Moloney R and Maggs C. A systematic review of the
relationships between written manual nursing care
planning, record keeping and patient outcomes. Journal
of Advanced Nursing 1999;30:51–7.
- Shepperd S, Parkes J, McClaren J and Phillips C. Discharge
planning from hospital to home. Cochrane
Database of Systematic Reviews 2004;1:CD000313.
- Morishita L, Boult C, Boult L, Smith S and Pacala JT.
Satisfaction with outpatient geriatric evaluation and
management (GEM). Gerontologist 1998;38:303–8.
- Bernabei R, Landi F and Gambassi G. Randomised trial
of impact of model of integrated care and case management
for older people living in the community. BMJ
1998;316:1348–51.
- Renholm M, Leino-Kilpi H and Suominen T. Critical
pathways. A systematic review. Journal of Nursing Administration
2002;32:196–202.
- Nakatani H and Shimanouchi S. Factors in care management
affecting client outcomes in home care. Nursing
and Health Sciences 2004;6:239–46.
- Long M and Marshall B. What price an additional day
of life? A cost-effectiveness study of case management.
American Journal of Managed Care 2000;6:881–6.
- Gagnon AJ, Schein C, McVey L and Bergman H.
Randomized controlled trial of nurse case management
of frail older people. Journal of the American Geriatrics
Society 1999;47:1118–24.
- Bedell JR, Cohen NL and Sullivan A. Case management:
the current best practices and the next generation of
innovation. Community Mental Health Journal 2000;36:
179–94.
- De Lepeleire J, Van Houdt S, Aertgeerts B and Buntinx F.
Het effect van een multidisciplinair zorgplan in de
thuiszorg. Leuven: Academisch Centrum Huisartsgeneeskunde
KULeuven, 2007. Report No.: ISBN
9789075828177.
- Marelli T and Hilliard L. Documentation and effective
patient care planning. Home Care Provider 1996;1:198–
201.
- Dees JP and Anderson NL. Case management: a management
system for quality and cost effective outcomes.
American Association of Occupational Health Nurses
Journal 1996;44:385–90.

