Keywords
Acute Disease; Early Diagnosis; Pancreatitis /radiography; Severity of Illness Index; Tomography, X-Ray Computed
Abbreviations
BUN: blood urea nitrogen; SIRS: systemic inflammatory response syndrome
INTRODUCTION
In a prior report from our institution involving patients with hemoconcentration at admission, those with necrotizing pancreatitis presented significantly earlier than those with interstitial disease [1]. This result suggests that duration of abdominal pain prior to presentation may have prognostic significance in acute pancreatitis. However, the majority of patients in this study were transferred from other hospitals. Therefore, it remains unclear whether this result is applicable to patients presenting directly to our institution. Our hypothesis was that patients who seek medical attention more promptly for their abdominal pain have more severe pancreatic injury as evidenced by an increased prevalence of local complications on radiographic imaging, and that hemoconcentration in the setting of an earlier presentation would be a more reliable risk factor for pancreatic necrosis.
The aim of the present study was to determine whether the duration of abdominal pain impacts the severity of acute pancreatitis among patients who were admitted directly to our institution. Our secondary aim was to make this determination in the subset of patients with hemoconcentration at admission.
METHODS
A cohort study was performed using data collected on all patients admitted directly to Brigham and Women’s Hospital with their first episode of acute pancreatitis between June 2005 and June 2010. Patients with acute pancreatitis who were transferred from other hospitals, those whose hospitalization occurred directly after undergoing an ERCP, and those whose acute pancreatitis developed during the hospitalization were excluded. Acute pancreatitis was defined by at least two of the following criteria: characteristic abdominal pain, serum amylase and/or lipase values exceeding three times the upper limit of normal, and a computed tomography (CT) scan or magnetic resonance imaging (MRI) demonstrating characteristic changes of acute pancreatitis [2].
Data collected included: age; prognostic markers of severity including admission hematocrit, blood urea nitrogen (BUN), and systemic inflammatory response syndrome (SIRS) in the first 24 hours; and outcome measures including pancreatic necrosis, need for admission to the intensive care unit, length of hospitalization, and death. SIRS scores were calculated for all patients based on the most extreme laboratory value or clinical measurement obtained during the initial 24 hours of hospitalization. Mortality was defined as death occurring during hospitalization. Pancreatic necrosis was defined by findings of parenchymal nonenhancement on at least one contrastenhanced CT scan according to the criteria set forth by the Atlanta symposium [2]. Patients who did not have a contrast-enhanced CT or MRI scan performed during hospitalization were considered to have interstitial pancreatitis.
Among patients with admission hematocrit equal to, or greater than, 44% who underwent a contrast-enhanced CT scan within 48 h of admission, an evaluation of the radiologic extent of the pancreatic and peripancreatic inflammatory changes was made in accordance with the Balthazar-Ranson scoring system: grade A: normal pancreas; grade B: pancreatic enlargement; grade C: pancreatic inflammation and/or peripancreatic fat inflammation; grade D: single peripancreatic fluid collection; grade E: 2 or more fluid collections and/or retroperitoneal air [3]. For purpose of this evaluation, we did not include additional points based on the presence or extent of pancreatic necrosis because of the difficulty in grading the extent of pancreatic necrosis during the early stages of acute pancreatitis [4]. In addition, our major interest was in the extent of the peripancreatic inflammatory response that might correlate with intravascular volume depletion resulting in hemoconcentration. All radiographic images were independently reviewed by study radiologists who were blinded to the aims of the study.
Patients with an admission hematocrit of 44% or more were dichotomized into a less than 12 h group or a 12 h or more group in accordance with the time lapse between the onset of their abdominal pain and presentation to our hospital. Information regarding the time lapse was gathered either on the basis of an interview on the day of admission or by a careful review of the medical records.
ETHICS
This study was approved by the Partners Institutional Review Board. The study protocol conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008. Written informed consent was obtained from each patient.
STATISTICS
Data are reported as frequencies, mean±SD, or median and interquartile range (IQR). The Fisher’s exact test was used for all categorical variables and the Mann- Whitney/Wilcoxon rank sum test was used for all continuous variables. All statistical analysis was performed using SAS® v.9.1 (SAS Institute, Cary, North Carolina, USA). Two-tailed P values less than 0.05 were considered significant.
RESULTS
A total of 847 patients with acute pancreatitis were evaluated, of whom 529 patients (62.5%) were excluded according to aforementioned criteria (Figure 1). In particular, 303 patients (35.8%) were excluded because they had experienced one or more prior episodes of acute pancreatitis, 140 (16.5%) because they had been transferred from other hospitals and 86 (10.2%) for other reasons. Only the 318 patients (37.5%) who presented directly to our hospital were enrolled into this study. Of these 318 patients, 62 (19.5%) patients had an admission hematocrit equal to, or greater than, 44%.
Figure 1. Selection of eligible patients with acute pancreatitis (AP).
Table 1 presents a comparison of parameters of disease severity among the 318 patients who presented directly to our hospital: 111 patients (34.9%) were admitted within 12 h and 207 (65.1%) 12 h or more from the onset of pain. There were no statistically significant differences observed between the two groups in any parameter of disease severity. In addition, severity of acute pancreatitis was evaluated among the 82 patients whose time of pain onset was confirmed prospectively on the day of admission (36 patients (43.9%) within 12 h vs. 46 patients (56.1%) 12 h or more). There were no statistically significant differences between the two groups in any of the parameters of disease severity (data not shown).
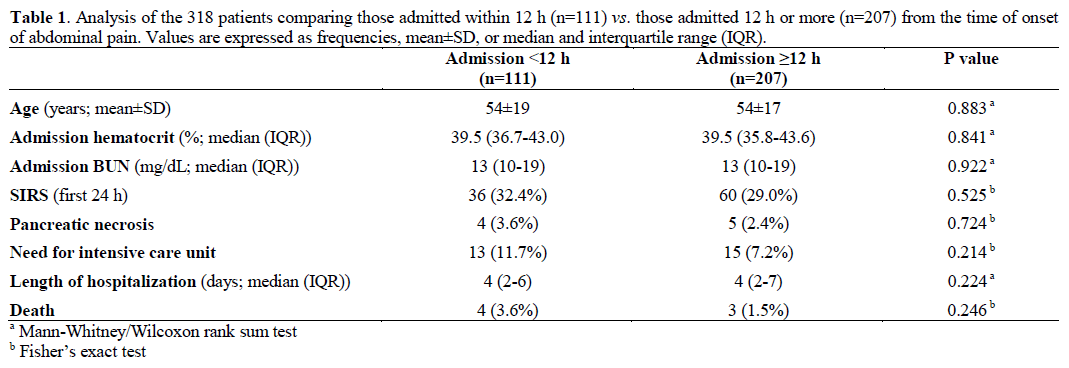
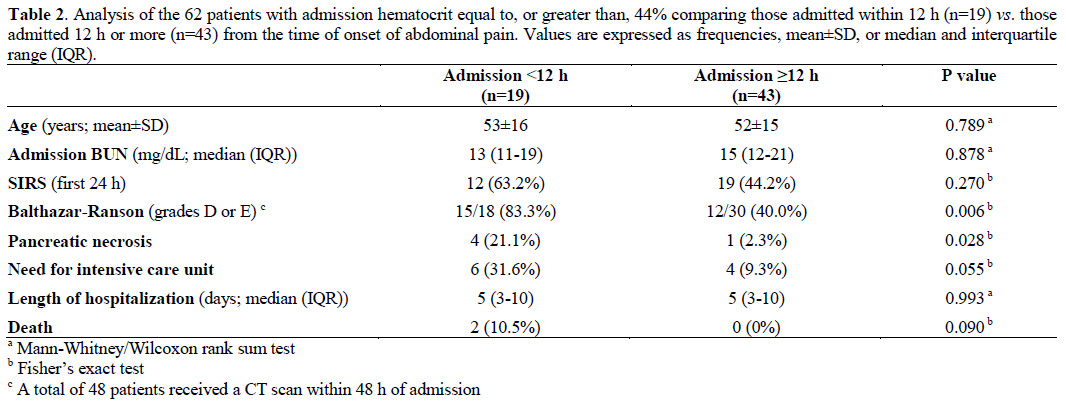
Table 2 presents a comparison of parameters of disease severity among the 62 patients with hemoconcentration: 19 (30.6%) were admitted within 12 h and 43 (69.4%) were admitted 12 h or more from the onset of pain. Patients admitted within 12 h had a significant increase in the prevalence of pancreatic necrosis compared to those admitted 12 h or more (4/19, 21.1% vs. 1/43, 2.3%; P=0.028). In addition, among the 48 patients (77.4%) who received a CT scan within 48 h of admission based on the discretion of the treating physician, those who presented within 12 h had a significant increase in radiologic severity within 48 h of admission compared to those admitted 12 h or more (Balthazar-Ranson grades D or E: 15/18, 83.3% vs. 12/30, 40.0%; P=0.006).
DISCUSSION
In the present study, patients with hemoconcentration at admission had more radiologically severe acute pancreatitis within 48 h of admission and a significant increase in the prevalence of pancreatic necrosis if they presented within 12 h from onset of abdominal pain when compared to patients presenting 12 h or more from the start of their pain.
The accuracy of hemoconcentration as a prognostic marker of severity has undergone considerable study in the past 15 years [5, 6, 7, 8, 9]. Whereas initial studies concluded that hemoconcentration was an early prognostic marker for necrotizing pancreatitis [5, 6] and organ failure [6], more recent studies have concluded that early hemoconcentration is associated with pancreatic necrosis [7] and increased mortality [8] only among transferred patients as opposed to direct admissions to a hospital [7, 8, 9].
There are important differences between these earlier studies and our present study. First, none of the previous studies evaluated the impact of duration of abdominal pain prior to admission on the development of pancreatic necrosis. Secondly, several of these earlier studies included patients with previous episodes of acute pancreatitis [7, 8]. Since the initial episode of acute pancreatitis is generally the most severe [2, 10], studies of possible prognostic markers of severity should be restricted to the initial episode.
The present study establishes the importance of hemoconcentration and duration of pain as prognostic markers of severity among directly admitted patients experiencing their initial episode of acute pancreatitis.
In a prior study utilizing artificial neural networks [11], hemoconcentration and duration of abdominal pain prior to admission have also been shown to correlate with the severity of acute pancreatitis. Among 6 risk variables that correlated most strongly with severity of acute pancreatitis, the most significant one was a shorter duration of pain prior to admission and the third most significant was hemoconcentration at admission [11]. Accordingly, there is increasing evidence linking hemoconcentration with duration of pain as prognostic markers of severity.
There is also evidence that the absence of hemoconcentration at admission correlates strongly with the development of mild acute pancreatitis [12] including a recent scoring algorithm entitled the Harmless Acute Pancreatitis Score (HAPS) [13]. In that report, the absence of hemoconcentration was associated with severity of acute pancreatitis in only 2% [13]. In the present study, only 1.6% (4/256) of patients without hemoconcentration developed necrotizing pancreatitis.
Prognostic markers of pancreatic necrosis are extremely important in the care of patients with acute pancreatitis due to the high mortality associated with necrotizing pancreatitis (approximately 15%) [14] compared to interstitial pancreatitis (approximately 3%) [15]. In previous reports, an increased BUN at admission was a prognostic marker of mortality in acute pancreatitis [16, 17]. However, there have been no prior studies that have evaluated admission BUN as a prognostic marker of pancreatic necrosis. Also, in a previous report, the development of SIRS in the initial 24 h of hospitalization was a prognostic marker of pancreatic necrosis [18]. In the present study, however, there was no significant difference in admission BUN and prevalence of SIRS when comparing patients admitted within 12 h versus those admitted 12 h or more from pain onset, either in the entire cohort of patients (Table 1) or among those with hemoconcentration (Table 2).
Patients in our study who sought medical attention within 12 h from the start of their pain had more widespread peripancreatic inflammatory response visualized on their CT scans compared to those presenting 12 h or more. More widespread peripancreatic inflammation may have caused an increase in the intensity of abdominal pain, thereby necessitating an earlier presentation to the hospital. A more robust peripancreatic inflammatory response may also have resulted in an accelerated intravascular volume depletion, resulting in more severe impairment of the pancreatic microcirculation.
For the purpose of our study, we graded the radiologic severity on contrast-enhanced CT scans obtained during the first 48 h based only on the extent of the peripancreatic inflammatory response, without adding additional score for the presence or extent of pancreatic necrosis. Our primary interest was in the correlation of severity of the peripancreatic inflammatory response to the development of hemoconcentration and necrotizing pancreatitis. Furthermore, the accuracy of the Balthazar-Ranson scoring system has been found to be similar to the accuracy of other CT scoring systems for assessing the radiographic severity of acute pancreatitis [19].
There are several strengths to our study. First, we included only patients experiencing their first episode of acute pancreatitis. In general, the first episode of acute pancreatitis is more severe when compared to subsequent episodes [2, 10]. Also, patients with prior episodes of acute pancreatitis might present earlier to obtain more timely relief of abdominal pain. Second, we excluded patients whose characteristics would confound the relationship between duration of abdominal pain and severity of acute pancreatitis. In particular, we excluded patients who had been transferred from other hospitals because as a group they generally have more severe disease than those who are direct admissions [2, 8].
There are several limitations to our study. First, the sample size is small. Observed trends are more robustly demonstrated with a large patient population. Second, information regarding duration of abdominal pain prior to arrival to our hospital was obtained retrospectively in many patients. Data obtained retrospectively may not be as accurate as data obtained prospectively. Because of this concern, we conducted a subset analysis of Table 1 restricted only to those patients whose time to arrival was obtained prospectively on the day of admission. In this subset analysis, there was also no statistical difference in any variable when comparing the less than 12 h group with the 12 h or more group. Third, we were not able to evaluate the impact of differences in intravenous fluid resuscitation in our results. At present, there is no consensus regarding the optimal rate of fluid resuscitation to prevent local complications (such as pancreatic necrosis) but not increase the risk of systemic complications (such as pulmonary edema) [20, 21, 22]. In conclusion, among patients with hemoconcentration who were experiencing their first episode of acute pancreatitis, those admitted within 12 h after the onset of abdominal pain compared to those admitted 12 h or later had more severe pancreatic injury as evidenced by an increased prevalence of pancreatic necrosis. Duration of abdominal pain prior to admission impacts the severity of acute pancreatitis among patients with hemoconcentration at presentation.
Conflicts of interest
None
References
- Brown A, Baillargeon JD, Hughes MD, et al. Can fluid resuscitation prevent pancreatic necrosis in severe acute pancreatitis? Pancreatology 2002; 2: 104-7. [PMID: 12123089]
- Banks PA, Freeman ML. Practice Guidelines in Acute Pancreatitis. Am J. Gastroenterol 2006; 101: 2379-2400. [PMID: 17032204]
- Balthazar EJ. Acute pancreatitis: assessment of severity with clinical and CT evaluation. Radiology 2002; 223: 603-613. [PMID: 12034923]
- Spaier BWM, Nio Y, van der Hulst RWM, Tuynman HARE, Dijkgraaf MGW, Bruno MJ. Practice and yield of early CT scan in acute pancreatitis: a Dutch observational multicenter study. Pancreatology 2010; 10: 222-228. [PMID: 20484959]
- Baillargeon JD, Oray J, Ramagopal V, Tenner SM, Banks PA. Hemoconcentration as an early risk factor for necrotizing pancreatitis. Am J Gastroenterol 1998; 93: 2130. [PMID: 9820385]
- Brown A, Orav J, Banks PA. Hemoconcentration is an early marker for organ failure and necrotizing pancreatitis. Pancreas 2000; 20: 367-372. [PMID: 10824690]
- Wu BU, Conwell DL, Singh VK, Repas K, Maurer R, Bollen TL, Mortele KJ, Banks PA. Early hemoconcentration is associated with pancreatic necrosis only among transferred patients. Pancreas 2010; 39: 572-576. [PMID: 20182394]
- Wu, BU, Johannes RS, Conwell DL, Banks PA. Early hemoconcentration predicts increased mortality only among transferred patients with acute pancreatitis. Pancreatology 2009; 9: 639-643. [PMID: 19657219]
- Gardner TB, Olenec CA, Chertoff JD, Mackenzie TA, Robertson DJ. Hemoconcentration and pancreatic necrosis. Further defining the relationship. Pancreas 2006; 33: 169-173. [PMID: 16868483]
- Yadav D, Lowenfels, AB. Trends in the epidemiology of the first attack of acute pancreatitis. Pancreas 2006; 33: 323-330. [PMID: 17079934]
- Andersson B, Andersson R, Ohlsson M, Nilsson J. Prediction of severe acute pancreatitis at admission to hospital using artificial neural networks. Pancreatology 2011; 11: 328-335. [PMID: 21757970]
- Muddana V, Whitcomb DC, Khalid A, Slivka A, Papachristou GI. Elevated serum creatinine as a marker of pancreatic necrosis in acute pancreatitis. Am J Gastroenterol 2009; 104; 164-70. [PMID: 19098865]
- Lankisch PG, Weber-Dany B, Hebel K, Maisonneuve P, Lowenfels AB. The harmless acute pancreatitis score: a clinical algorithm for rapid initial stratification of nonsevere disease. ClinGastroenterolHepatol 2009; 7: 702-705. [PMID: 19245846]
- Van Santvoort HC, Bakker OJ, Bollen TL, Besselink MG, et al. A conservative minimally invasive approach to necrotizing pancreatitis improves outcome. Gastroenterol 2011; 141: 1254-1263. [PMID: 21741922]
- Singh VK, Bollen TL, Wu BU, Repas K, Rie M, Song Y, Moretle KJ, Conwell DL, Banks PA. An assessment of the severity of interstitial pancreatitis. ClinGastroenterolHeptalol 2011; 9: 1098- 1103. [PMID: 21893128]
- Wu BU, Johannes RS, Sun X, Conwell DL, Banks PA. Early changes in blood urea nitrogen predict mortality in acute pancreatitis. Gastroenterol 2009; 137: 129-135. [PMID: 19344722]
- Wu BU, Bakker Oj, Papachristou GI, Besselink MG, Banks PA, et al. Blood urea nitrogen in the early assessment of acute pancreatitis. Arch Intern Med 2011; 1711 669-676. [PMID: 21482842]
- Singh VK, Wu BU, Bollen TL. Repas K, Maurer R, Mortele KJ, Banks PA. Early systemic inflammatory response syndrome is associated with severe acute pancreatitis. ClinGastroenterolHepatol 2009; 7: 1247-1251. [PMID: 19686869]
- Bollen TL, Singh VK, Mauer R, Repas K, van Es HW, Banks PA, Mortele KJ. A comparative evaluation of radiologic and clinical scoring systems in the early prediction of severity in acute pancreatitis. Am J Gastroenterol 2012; 107: 612-619. [PMID: 22186977].
- Trikudanathan G, Navaneethan U, SwaroopVege S. Current controversies in fluid resuscitation in acute pancreatitis. A systematic review. Pancreas 2012; 41: 827- 834. [PMID: 22781906]
- Haydock MD, Mittal A, Wilms HR, Phillips A, Petrov MS, Windsor JA. Fluid therapy in acute pancreatitis. anybody's guess. Ann Surg. 2012; (in press) [PMID:23207241]
- Fisher JM, Gardner TB. The “golden hours” of management in acute pancreatitis. Am J Gastroenterol 2012; 107: 1146-1150.[PMID: 22858994]


