Keywords
Colorectal Neoplasms; Drug Therapy; gemcitabine; gemcitabineoxaliplatin regimen; oxaliplatin; Pancreatic Neoplasms; Peripheral Nervous System Diseases
Abbreviations
DDC: duration of disease control; FF: 5-fluorouracil plus folinic acid or leucovorin (FA); FOLFOX: oxaliplatin plus 5-fluorouracil (5-FU) plus leucovorin; GemOx: gemcitabine and oxaliplatin; OFF: 5- fluorouracil plus folinic acid or leucovorin plus oxaliplatin; OPTIMOX: optimizing oxaliplatin-induced neuropathy ("stop-andgo" approach)
Dear Sir
Since 1997, gemcitabine remains the only standard chemotherapy approved by the US FDA for the treatment of advanced pancreatic cancer , which showed superior clinical benefit to single-agent 5-fluorouracil [1]. Numerous new agents, both cytotoxic and targeted, have been tested against and in combination with this standard. Many combination therapy regimens showed encouraging results in phase II settings, which led to more than 12 randomized phase III trials in the last decade [2]. The combination of gemcitabine and erlotinib is the first combination therapy to demonstrate survival benefits in pancreatic cancer in a phase III study albeit a modest one [3]. Some trials showed improved response rates or progression-free survival, but there was no clear improvement in survival. Among these combinations, the combination of gemcitabine plus platinum agents showed improved progression-free survival or time-to-tumor progression, but failed to demonstrate a survival advantage over gemcitabine [4]. This combination has regained attention after a recent pooled analysis and a meta-analysis suggested a survival benefit of gemcitabineplatinum doublets when compared with single agent gemcitabine [4, 5]. Moreover, this regimen seems to be a reasonable option in patients with excellent performance status [4]. Sensory neurotoxicity is a potentially limiting factor in many patients who might otherwise achieve good results with oxaliplatin therapy, but it may be overcome in several ways [6]. Prevention or cure is one option, for which glutathione, carbamazepine and gabapentin have already been investigated [6]. Another option is to administer a limited number of cycles of oxaliplatin at an optimal dose intensity, but to suspend treatment after delivering a total dose below that of the oxaliplatin cumulative toxic dose and before the development of resistance, thus enabling later reintroduction of the drug [7, 8]. Such a strategy is termed as optimizing oxaliplatininduced neuropathy (OPTIMOX: "stop-andgo" approach). This strategy seems to be successful when used as a first-line approach, rather than being held in reserve until chemotherapy based on another agent fails in patients with metastatic colorectal cancer. However, no data exists to support OPTIMOX strategy in pancreatic cancer. We here describe the first report of a patient with metastatic pancreatic cancer in whom OPTIMOX strategy allows her to manage the toxicity as well as achieve long-term disease control.
Case Report
A 69-year-old woman with unremarkable past medical history presented in November 2006 with insidious onset of abdominal pain and bloating. A CT scan showed a liver cyst as large as 4.4 cm, the omentum studded with soft tissue densities and nodules, a leiomyomatous uterus, a right adnexal mass versus leiomyoma. The patient was unable to tolerate the vaginal ultrasound, but an abdominal ultrasound revealed the presence of the right adnexal mass. She was referred to gynecological oncologist for possible ovarian cancer versus a primary peritoneal carcinoma. On January 25th, 2007, she underwent total abdominal hysterectomy, bilateral salpingooophorectomy, total omentectomy, tumor debulking, lysis of adhesions, peritoneal biopsies, right pelvic wall resection as well as peritoneal stripping. The intraoperative report revealed findings including 200 mL of bloody ascites, the cul-de-sac covered with numerous tumor nodules extending up the right uterosacral ligament; the right pelvic sidewall covered with tumor nodules as well as the right side of the bladder serosa. The omentum additionally was noted to have very large tumor measuring 12x10 cm, and numerous small lesions were appreciated on the dome of the liver. Additional masses were appreciated within the greater stomach curvature and the lesser omentum. The tumor was strongly positive for cytokeratin-7 (CK7) with focal strong staining for cytokeratin-20 (CK20) and was negative for estrogen receptor, progesterone receptor, and CA 125. The overall impression was that of metastatic disease more than a primary adnexal process. A repeat CT scan on February 5th, 2007 revealed an ill-defined mass within the pancreatic tail and involving the splenic hilum measuring 2.6x3.3 cm. Peritoneal implants involving the greater omentum were again demonstrated measuring in the range of 1.3- 1.8 cm. On February 8th, the patient underwent an endoscopic ultrasound which described a normal size pancreatic duct throughout the head, uncinate process, and body of the pancreas, and then disappearing within a mass appreciated within the tail of the pancreas. The mass measured 27.4x32.7 mm. Under ultrasound guidance a fine needle aspiration was performed with the pathology consistent with pancreatic adenocarcinoma. Her CEA level was elevated at 8.6 U/L (reference range: 0-3 U/L) (Table 1) and CA 19-9 was within normal limits.
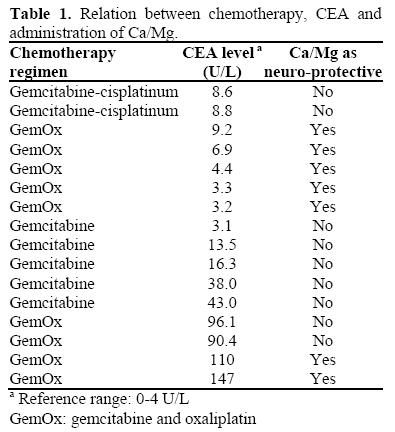
She was begun on treatment with gemcitabine/cisplatin on February 27th, 2007, for two cycles. Therapy was then changed to GemOx consisting of gemcitabine (1,000 mg/m2 i.v.) and oxaliplatin (85 mg/m2 i.v.) every two weeks on April 2nd, 2007. The regimen was modified to GemOx as per institutional practice (see discussion section) [9]. Patient received calcium and magnesium 1 g m each before and after oxaliplatin as per institutional practice. Oxaliplatin discontinued in August 2007 (cumulative dose: 765 mg/m2) due to cumulative thrombocytopenia/anemia and peripheral neuropathy. Patient was continued on single agent, gemcitabine at dose of 1,000 mg/m2 i.v. over 30 minutes for two weeks out of three weeks till she developed progressive disease in January 2008 (duration: 5.5 months) and elevated CEA level of 38 U/L (Table 1). Since patient has no thrombocytopenia and only grade 1 peripheral neuropathy, it was decided to reintroduce oxaliplatin in February 2008. A CT scan after 2 months (April 2008) showed stable disease along with stable CEA at 43 U/L. However, a repeat CT scan in June 2008 showed progressive disease with an elevated CEA of 110 U/L (duration: 4 months; total dose: 260 mg/m2). Overall, the patient received a total of 1,025 mg/m2.
Discussion
Unlike cisplatin neurotoxicity, oxaliplatin sensory neurotoxicity is reversible, even where it persists for several months, but requires discontinuation of treatment. Since oxaliplatin-related neurotoxicity is reversible, this raises the question of whether oxaliplatin reintroduction is beneficial in patients who are withdrawn from treatment prior to developing resistance to oxaliplatin. Here, we reported our experience of reintroducing oxaliplatin in patients with advanced pancreatic cancer who achieved disease control for a total of 17 months.
Because neuromodulatory agents have shown rather disappointing activity in the prevention of oxaliplatin-induced neurotoxicity [6], the so-called OPTIMOX approach remains the preferred strategy when oxaliplatin-based therapy is used first-line in the palliative setting. OPTIMOX-2 study, which was a follow up to OPTIMOX-1 study, looked at the question of giving patients who have responded to chemotherapy and are stable a chemotherapy-free period in patients with metastatic colorectal cancer [7, 8]. OPTIMOX-1 evaluated the feasibility of an oxaliplatin-free interval (not a chemotherapyfree period) and found that patients who were treated with this “stop-and-go” approach for oxaliplatin fared every bit as well, in terms of overall survival, as those individuals on FOLFOX (oxaliplatin/5-fluorouracil (5- FU)/leucovorin) who did not have an oxaliplatin-free interval. So, OPTIMOX-2 took this question to the next level and asked whether we can give a patient a chemotherapy-free period. FOLFOX7 (a version of FOLFOX regimen consisting of oxaliplatin (130 mg/m2) infused with leucovorin (400 mg/m2) over 2 h on day 1, followed by bolus 400 mg/m2 and a 46-h infusion of 5-FU (2,400 g/m2), every 2 weeks) was given for 6 cycles to patients in both arms, but then patients in the experimental arm, instead of continuing on 5-FU/leucovorin maintenance (as in OPTIMOX-1), received no maintenance until progression, when chemotherapy with FOLFOX7 was reintroduced.
The OPTIMOX-2 study was initially designed as a 600-patient, phase 3 trial, but when bevacizumab became available in France, the trial was downgraded to a phase 2 study with an accrual goal of 200 patients. The primary objective was the duration of disease control (DDC), calculated as the sum of the duration of the progression free survival (PFS) induced with the initial FOLFOX therapy and with the subsequent reintroduction of FOLFOX (Figure 1). One important characteristic of OPTIMOX-2 was that after induction of a response, metastases were allowed to progress back to baseline levels before FOLFOX was reintroduced. In terms of efficacy, continuing treatment with a maintenance protocol resulted in longer progression free survival, compared with pausing treatment altogether (8.7 vs. 6.9 months; P=0.009). However, the duration of disease control was almost identical in both arms (12.9 vs. 11.7 months; P NS).
Figure 1. OPTIMOX trials: the duration of disease
control (DDC) concept (modified from [7]).
PD: progressive disease
PFS: progression free survival
PR: partial response
It has to be emphasized, however, that duration of disease control is not a validated endpoint in clinical trials and that its relevance for clinical practice is not yet established, and data on overall survival are available for OPTIMOX-2 did show decreased over all survival in patients who had chemotherapy free interval.
However, chemotherapy free intervals are applicable for certain patients, especially patients with favorable tumor biology and especially in diseases like advanced pancreatic cancer. Future studies are warranted to explore OPTIMOX-2 strategy in patients with pancreatic cancer who are candidates for gemcitabine plus a platinum based regimen. Moreover, the role of maintenance therapy, not with chemotherapy, but with targeted drugs also needs to be explored akin to the DREAM-OPTIMOX3 study in colon cancer [10].
With these data, some patients can be given time off treatment from drugs causing toxicities while maintaining the other agent (OPTIMOX-1 like strategy), allowing them to resolve toxicities, to have time spent out of the hospital, out of the clinic, traveling, on vacation, allowing their normal tissue time to recover. It is very much appreciated by patients, and that is the bottom line.
As shown in the case report, this patient received a simplified D1-D1 (day 1 - day 1) GemOx regimen (S-GemOx) presented by Andre T et al. at the ASCO 2007 annual meeting [9]. In this study, patients with advanced pancreatic cancer were 2:1 randomly assigned for first-line treatment to S-GemOx (arm A: gemcitabine 1,000 mg/m2, 100 min infusion day 1, immediately followed by oxaliplatin 100 mg/m2, 120 min infusion) or to GemOx (arm B: gemcitabine day 1 and oxaliplatin day 2). Treatment was repeated in each arm every 2 weeks until disease progression. Among 57 patients enrolled (A: n=37; B: n=20) response rate was 27% in arm A and 10% in arm B. Median progression free survival was 4.0 and 2.5 months in arm A and B, respectively. Median overall survival was 7.6 and 3.2 months in arm A and B, respectively. S-GemOx was more toxic than GemOx for grade 3-4 neutropenia (20% vs. 0%) and thrombocytopenia (16% vs. 10%). Other toxicities were comparable. However, since more cycles were administered in arm A (median: 8.5, range: 1-29; vs. median: 5.8, range: 2-12), grade 3 oxaliplatin-induced neuropathy was higher in arm A (21.6% vs. 0%). Based on this study, we at the Yale Cancer Center modified S-GemOx to gemcitabine 1,000 mg/m2, 30 min infusion day 1, immediately followed by 120 min infusion of oxaliplatin 85 mg/m2, and found it safe and efficacious (unpublished data).
This issue of OPTIMOX gains more significance after a recent study presented at the annual meeting of ASCO 2008. The CONKO-003 study [11] randomized 165 patients to FF (5-FU 2 g/m2 (24 h) plus folinic acid or leucovorin (FA) 200 mg/m2 (30 min) on days 1, 8, 15, and 22) or OFF (FF plus oxaliplatin 85 mg/m2, days 8 and 22). OFF resulted in significantly longer progression free survival (P=0.012) and overall survival (P=0.014) vs. FF. OFF also results in substantially greater clinical benefit in patients with poor prognostic features. The authors suggested that OFF should be considered standard second-line treatment in patients who progress on gemcitabine.
In conclusion, the results of this study suggest that reintroduction of oxaliplatin following a break for neurotoxicity or to delay the development of resistance is safe and proves clinically beneficial in selected cases.
Conflict of interest
The authors have no potential conflicts of interest
Acknowledgement
I would particularly like to thank my daughter Nawal Wasif, who has taken time and effort to work on the preparation of this manuscript as her summer project, in special creating the Tables.
References
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J ClinOncol 1997; 15:2403-13. [PMID 9196156]
- Saif MW. Pancreatic cancer: is this bleak landscape finally changing? Highlights from the '43rd ASCO Annual Meeting'. Chicago, IL, USA. June 1-5, 2007. JOP. J Pancreas (Online) 2007; 8:365-73. [PMID 17625289]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007; 25:1960-6. [PMID 17452677]
- Saif MW, Kim R. Role of platinum agents in the management of advanced pancreatic cancer. Expert OpinPharmacother 2007; 8:2719-2. [PMID 17956194]
- Heinemann V, Labianca R, Hinke A, Louvet C. Increased survival using platinum analog combined with gemcitabine as compared to single-agent gemcitabine in advanced pancreatic cancer: pooled analysis of two randomized trials, the GERCOR/GISCAD intergroup study and a German multicenter study. Ann Oncol 2007; 18:1652-9. [PMID 17660491]
- Saif MW, Reardon J. Management of oxaliplatininduced peripheral neuropathy. TherClin Risk Manag 2005; 1:249-58. [PMID 18360567]
- Tournigand C, Cervantes A, Figer A, Lledo G, Flesch M, Buyse M, et al. OPTIMOX1: a randomized study of FOLFOX4 or FOLFOX7 with oxaliplatin in a stop and go fashion in advanced colorectal cancer -- a GERCOR study. J ClinOncol 2006; 24:394-400. [PMID 16421419]
- Maindrault-Goebel F, Lledo G, Chibaudel B, Mineur L, Andre T, Bennamoun M, et al. Final results of OPTIMOX2, a large randomized phase II study of maintenance therapy or chemotherapy-free intervals (CFI) after FOLFOX in patients with metastatic colorectal cancer (MRC): A GERCOR study. J ClinOncol 2007; 25(18S, 20 Supplement):4013.ASCO Annual Meeting Proceedings.
- Andre T, Afchain P, Lledo G, Nguyen S, Paitel J, Mineur L, et al. First-line simplified GemOx (D1-D1) versus classical GemOx (D1-D2) in metastatic pancreatic adenocarcinoma (MPA). A GERCOR randomized phase II study. J ClinOncol 2007; 25(18S, 20 Supplement):4592.ASCO Annual Meeting Proceedings.
- Tournigand C, Lledo G, Delord J, André T, Maindrault-Goebel F, Louvet C, et al. Modified (m)Folfox7/bevacizumab (B) or modified (m)Xelox/bevacizumab with or without erlotinib (E) in first-line metastatic colorectal cancer (MCRC): Results of the feasibility phase of the DREAM-OPTIMOX3 study (GERCOR). J ClinOncol 2007; 25(18S, 20 Supplement):4097.ASCO Annual Meeting Proceedings.
- Pelzer U, Kubica K, Stieler J, Schwaner I, Heil G, Gorner M, et al. A randomized trial in patients with gemcitabine refractory pancreatic cancer. Final results of the CONKO 003 study. J ClinOncol 2008; 26(20 Supplement):4508.ASCO Annual Meeting Proceedings


