Keywords
Biopsy, Fine-Needle; Cytological Techniques;
Endoscopic Ultrasound-Guided Fine Needle Aspiration;
Endosonography; Pancreatic Neoplasms; Pancreatitis, Chronic
INTRODUCTION
Endoscopic ultrasound (EUS) allows excellent
visualization of the pancreas and the adjacent organs
and has evolved as a sensitive staging modality for
pancreatic malignancy [1, 2, 3, 4]. The addition of EUS
guided fine needle aspiration (FNA) allows cytological
diagnosis of solid pancreatic masses. This has been
shown in published series to be highly accurate in
diagnosing pancreatic masses with sensitivities ranging
from 64 to 91% [5, 6, 7, 8]. The presence of an in room
cytopathologist has been suggested as an important
measure to improve the adequacy of the aspirate and
therefore the diagnostic yield [9, 10]. There is robust
data available from non pancreaticobiliary FNA
literature on the role of onsite adequacy assessment
[11, 12, 13, 14].
However, it is not clear if these benefits will be realised using a cytotechnologist (i.e. a biomedical scientist) for
adequacy assessment or the impact of this on an
established and experienced pancreatic EUS-FNA
service.
The aim of this study is to assess the impact on
diagnostic performance of introduction of an in room
cytotechnologist to an established pancreatic EUS
service.
MATERIAL AND METHODS
This study includes all patients with solid
pancreaticobiliary lesions who underwent EUS-FNA
over an 18-month period from April 2009 to September
2010. Patients were retrospectively identified from a
prospectively maintained EUS database. All the
procedures were performed by either K.O. or M.K.N.
The unit is a tertiary referral centre for pancreaticobiliary
diseases for the North East of England serving a
population of 3.5 million. We perform in excess of 250
pancreaticobiliary EUS-FNA of solid and cystic lesions
per annum. We have been performing EUS-FNA since
2003 but did not have an in room cytotechnologist till
this time period. During this period the in room
cytotechnologist attended only two of the four EUS
lists as there was funding available only for these lists.
Patients were allocated to lists in turn and there was no
influence of the presence or otherwise of the cytotechnologist. Therefore there were two groups
identified:
Group 1: cytotechnologist absent;
Group 2: cytotechnologist present.
All patients were managed via a dedicated
pancreaticobiliary multidisciplinary meeting. Patients
with mixed solid/cystic lesions were excluded from this
analysis.
EUS-FNA Technique
Patients received conscious sedation with combinations
of intravenous midazolam, and pethidine under
appropriate cardiorespiratory monitoring. EUS and
EUS-FNA was performed using an echoendoscope
(EG383OUT, Pentax, Slough, United Kingdom) and
ultrasound workstation (EUB 7500; Hitachi Medical
Systems, Wellingborough, United Kingdom). Twentytwo
G and 25 G needles (Cook Ireland, Limerick,
Ireland) were used. A standard technique was followed.
The mass was identified and after staging assessment
and the use of Doppler to assess for vessels, the FNA
needle was passed into the lesion under EUS control.
Suction was used and the needle moved within the
tumour for 6-10 throws. The needle was removed and
the stylet replaced to express tissue onto glass slides.
One spread slide was prepared per pass and the
remaining aspirate placed into cytofix red solution (BD
Surepath, Bioscience Healthcare, Nottingham, United
Kingdom) and processed by liquid based cytology in
the cytology laboratory. The cytofix red solution lyses
red blood cells and reduces debris, subsequent
preparation produces a round 13 mm cellular
homogenous thin layer of cells largely free from
fixation and drying artefacts. On the days a
cytotechnologist was present, the prepared air dried
slide was stained with Diff Quick (Diff-Quick; BD
Surepath; Bioscience Healthcare, Nottingham, United
Kingdom) stain and their adequacy assessment based
on this material. Punctures were repeated until the
cytotechnologist considered the sample as adequate for
providing a diagnosis. The adequacy assessment by the
cytotechnician was based on the presence of
pancreaticobiliary tissue. If no tissue was present then
the sample was reported as inadequate. If the sample
was reported as adequate then the cytotechnician would
be able to comment on whether the sample had benign
cells, i.e. normal tissue, atypical cells, cells highly
suspicious or diagnostic of malignancy. In the absence
of the cytotechnologist, it was the endosonographers
discretion and assessment of the sample which helped
him decide on the number of passes. The slides were
air dried by the endosonographers and sent to the
cytopathology department with the liquid based
cytology needle rinsings for reporting.
Cytological Reporting
The final reporting was done by one of the six
experienced consultant cytopathologists. Samples were
graded as follows: inadequate, benign atypical, highly
suspicious of malignancy, and malignant.
For the purposes of this study; highly suspicious and
malignant samples were categorised as malignant.
Follow up
Final diagnosis of a malignant or benign mass was
based on the following reference methods:
1) surgical histology or other biopsy methods (e.g.,
percutaneous sampling of the primary tumour);
2) positive cytology result combined with clinical and
radiological follow-up that provided further evidence
of malignancy;
3) clinical, biochemical and radiological follow-up for
at least 12 months for a diagnosis of benign disease in
non operated cases with benign cytology.
ETHICS
Written informed consent was obtained from all
patients prior to the procedures. All procedures were
done as a part of standard patient care and not to a
research protocol and data collection was performed as
part of our ongoing clinical audit (quality monitoring).
Therefore institutional review body approval was not
required. Normal NHS Clinical Audit Practice was
observed. All aspects of the study were conducted in
accordance with the Declaration of Helsinki 1964, as
revised in Tokyo 2004.
STATISTICS
Frequencies, mean, standard deviation (SD) and range
were reported as descriptive statistics. The Mann-
Whitney, the Pearson chi-square, and the Fisher’s exact
tests were applied. Sensitivity, specificity, positive and
negative predictive values, and accuracy were
determined for the two groups. Diagnostic accuracy
was defined as the frequency of cases correctly
classified. The exact 95% confidence intervals (95%
CI) of frequencies were calculated by means of the
binomial distribution [15] and differences in diagnostic
performance between the two groups were identified
by using the Fisher’s exact test. The statistical
significance was assessed at the 0.05 level (two-tailed).
Statistical analysis was performed using MedCalc
(version 11.3.1.0; MedCalc Software, Mariakerke,
Belgium; https://www.medcalc.be/).
RESULTS
The demographic data and final diagnosis are as shown
in Tables 1 and 2. There was equal sex distribution in
both the groups. When Groups 1 and 2 were compared,
none of the parameters, including inadequate aspirate
rates and mean number of passes, reached statistical
significance (P values greater than 0.05). The
pancreatic masses were predominantly in the head and
body of pancreas in both the groups. Biliary lesions
were predominantly in the lower and mid common bile
duct. Majority of the lesions in both groups (more than
70%) were primary ductal adenocarcinoma. The mean
follow up for patients with suspected benign pathology
were 17.5 months (range: 15-35 months; n=9) and 17.1
months (range: 15-32 months; n=18) in Group 1 and
Group 2, respectively (P=0.942).
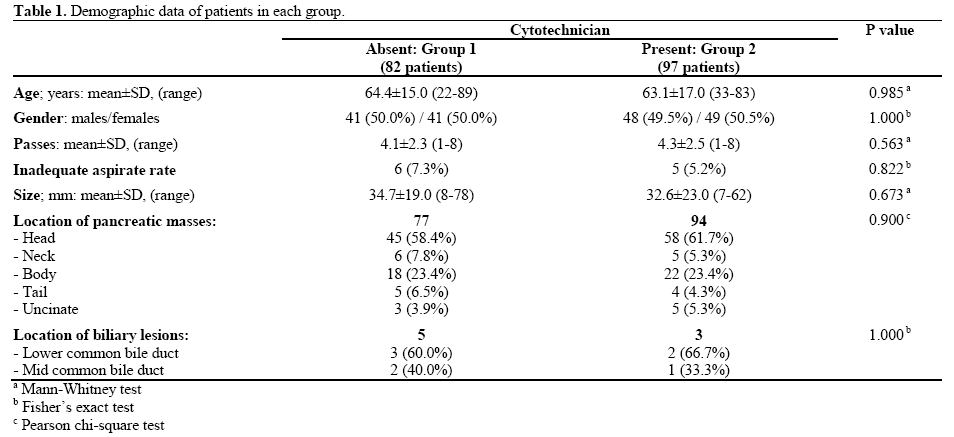
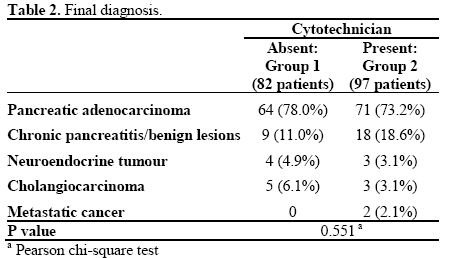
Table 3 shows statistical data including all solid
pancreaticobiliary lesions. There was no statistically
significant difference in accuracy, sensitivity,
specificity, positive predictive value and negative
predictive value between the two groups though the
negative predictive value was numerically higher in
Group 2.
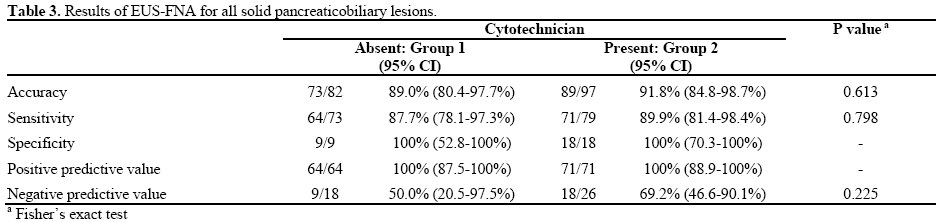
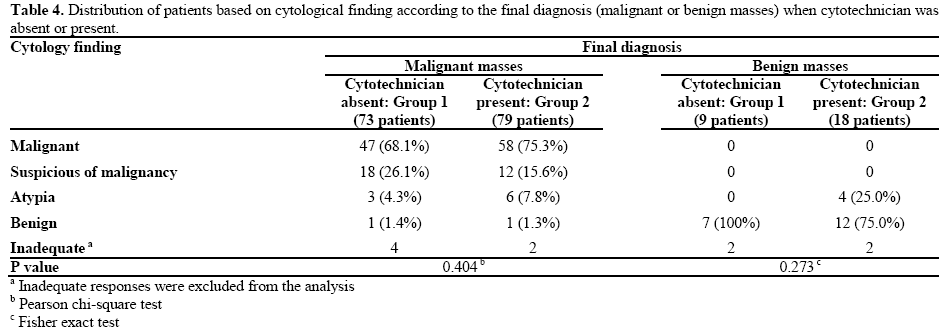
Table 4 shows the distribution of patients according to
cytology result. Malignant vs. benign lesions were not
influenced by the presence or absence of on-site
adequacy assessment (P=0.177); in fact, out of 75
adequate diagnoses of Group 1, 68 (90.7%) were
malignant and 7 (9.3%) were benign, while out of 93
adequate diagnoses of Group 2, 77 (82.8%) were
malignant and 16 (17.2%) were benign. Although 4 (25.0%) out of 16 benign masses were judged as
atypias in Group 2 vs. none in Group 1, the statistical
analysis did not show any significant difference
between the two groups both within malignant
(P=0.404) and benign lesions (P=0.273).
Finally, there were no complications in either group.
DISCUSSION
EUS provides excellent imaging of the pancreas and is
a sensitive staging test for pancreaticobiliary
malignancy [1, 2, 3, 4]. EUS-FNA has been shown to
be highly accurate in obtaining tissue with an average
sensitivity of 85% and accuracy of 88% in published
series [7]. However good test performance is not
invariable and poor performance has been reported
[16]. Factors that could influence the diagnostic
performance of EUS-FNA of the pancreas include the
experience of the endosonographer and reporting
cytopathologist, the number of passes, sample
preparation, the availability of onsite cytopathological
assessment and the prevalence of chronic pancreatitis
where tissue can be difficult to obtain making
cytopathological interpretation difficult [17, 18, 19, 20, 21, 22, 23, 24]. Optimising the performance of a
service requires careful attention to all of these
different variables. The perceived benefit of onsite
cytopathological evaluation is to reduce or eliminate
the unsatisfactory aspirate rate therefore ensuring that representative and potentially diagnostic material is
sent to the laboratory. FNA’s of the lesion are
performed until the cytotechnologist as in this study or
cytopathologist deems the material to be adequate.
There are robust data on the role of in room
cytopathologist improving the diagnostic accuracy of
lymph nodes, breast, thyroid and lung masses [11, 12, 13, 14].
The data on the role of pancreatic FNA is less clear cut,
with some studies utilising a cytopathologist [7, 25, 26]
others without any onsite adequacy assessment [27, 28, 29, 30] and some authors utilising an in room
cytotechnologist [31, 32, 33].
Klapman et al. [25] compared two sites with (centre 1)
and without (centre 2) an in room cytopathologist
present in all patients undergoing EUS-FNA for any
gastrointestinal and mediastinal lesions. One-hundred
and ten out 195 patients had EUS-FNA of the pancreas
(56.4%). The overall accuracy was 81% if both
positive and suspicious samples, i.e. grade 4 and 5
were included, and 78% if only grade 5 was included
as positive in centre 1 and 68% and 52%, respectively
for centre 2. The unsatisfactory aspirate rate was higher
in centre 2 as compared to centre 1 (20% vs. 9%). They
concluded that an in room cytopathologist is a vital
component of the EUS-FNA procedure and should be
taken into consideration when setting up the service.
However, the two groups were not similar in terms of
the number of pancreatic cases as they were more
common in the centre without onsite cytopathology.
Turner and colleagues [7] reported the results of a large
retrospective study of 442 patients undergoing EUSFNA
of pancreatic tumours. Using strict cytological
criteria, i.e. categorising samples graded as highly
suspicious as false negative, their accuracy was 80%
with a negative predictive value of 43%. If highly
suspicious cytology was classified as positive result,
accuracy was 87% andt he negative predictive value
was 53%. An in room cytopathologist was available for
adequacy assessment in only 43% of all cases.
Iglesias-Garcia et al. [26] recently reported their results
on the role of an in room cytopathologist in patients
with pancreatic lesions. They found that onsite
assessment by a cytopathologist significantly lowered the inadequate aspirate rate (1% vs. 12.6%) and the
number of passes (2.0±0.7 vs. 3.5±1.0) resulting in
significantly improved accuracy (96.8% vs. 86.2%) for
malignancy. However there was a significantly higher
number of benign cases in the group without the in
room cytopathologist (32 vs. 16).
Other studies have reported excellent diagnostic
performance without the availability of an onsite
cytopathologist. Hwang et al. [27] reported an overall
accuracy of 83% and a negative predictive value of
46% without the presence of a cytotechnician or
cytopathologist. These results are similar to those of
our study but it is not clear if the authors included
grade 4 as a true positive sample. Their inadequate
aspirate rate was 12%. Cherian et al. [28] reported an
overall accuracy and negative predictive value of 96%
and 85%, respectively in the absence of a
cytopathologist. Itoi et al. [29] reported similar data in
a large retrospective study in the absence of an onsite
assessment with an accuracy of 90.7% and negative
predictive value of 68.8%. Similarly Hikichi and
colleagues [30] reported on the role of onsite adequacy
assessment either by the endosonographer (Group 1) or
the cytopathologist (Group 2) in a low volume centre in
separate time periods. They reported no significant
difference in the accuracy or negative predictive value
between the two groups (94.7% and 83.3% vs. 94.3%
and 75%) but concluded that for accurate diagnosis,
rapid onsite evaluation (ROSE) should be performed
during EUS-FNA by the endosonographer if no
cytopathologist is available.
Therefore, the evidence is divided in literature as to
whether onsite cytopathologist is necessary for
improving the diagnostic accuracy of EUS-FNA of
pancreatic lesions. There is also evidence that suggests
onsite adequacy assessment by a non medical person,
i.e. cytotechnologist, could improve results.
Alsohaibani et al. [31] compared onsite assessment in
consecutive periods of time by a cytotechnologist and
nurse respectively and found diagnostic yield was
significantly improved by the presence of the
cytotechnician. In addition, Savoy et al. [32] conducted
a double blinded randomised trial to determine the
accuracy of onsite cytopathology interpretation of EUS-FNA of all solid lesion including pancreatic
lesions by comparing endosonographers with a
cytotechnologist. The authors concluded that
endosonographers were inferior to cytotechnologist in
improving the onsite adequacy assessments thus
highlighting the importance of cytotechnologists.
Initial EUS-FNA series reported inadequate aspirate
rates in the order of 16-20% [16] and reducing this by
the use of onsite cytopathology evaluation is the aim of
onsite adequacy assessment. In our unit onsite
assessment was introduced at a time the service had
already been running for over 6 years and the
endosonographers and cytopathologists had experience
of over 700 pancreatic FNAs. In addition liquid based
cytology was in use which has been shown to reduce
inadequate aspirates [34]. These two factors may
account for the low inadequate aspirate rate of 7.1% in
the absence of onsite assessment seen in our series and
contribute to the lack of benefit seen with the presence
of the cytotechnologist. Our cytotechnologists are
experienced in undertaking adequacy assessment in
other sites, e.g. lung FNA’s [35, 36, 37]. They were
trained and monitored in providing adequacy
assessment for the pancreatic FNA’s by the
cytopathologist leading the service (V.W.). Studies that
have made a direct comparison and shown a difference
have utilised a cytopathologist rather than
cytotechnologist and it may be that the greater
experience and knowledge of the cytopathologist is the
critical factor. However Petrone et al. [33] concluded
that an adequate training period with an expert
pathologist significantly improves the
cytotechnologist’s skill in terms of judging adequacy
and diagnostic accuracy. Therefore, it is possible to
achieve comparable results with rapid onsite evaluation
by a cytotechnician.
A possible shortcoming of our study is that it covered
the period of time of introduction of onsite assessment
and therefore includes the learning curve of the
cytotechnologists. However improving diagnostic
performance by improving the yield would be difficult
in view of the low inadequate aspirate rate in the
absence of the cytotechnologist. In addition this cannot
be considered a case control/cohort study.
Interventions in addition to in room cytotechnologist
that have been shown to increase diagnostic
performance include optimising the number of needle
passes (by improving yield) [24], varying the site of
puncture within the lesion [18] (improving yield),
dedicated supervised training of the endosonographer
(improving technique) [38], cytopathologist training
and mentoring [39], and increasing the number of
categorical diagnosis by reducing the number of
samples categorised as atypical or suspicious [40].
To conclude, our results suggest that the utility of
onsite adequacy assessment by a
cytotechnologist/biomedical scientist in an established
high volume pancreatic EUS-FNA service using liquid
based cytology with baseline good diagnostic
performance is unproven. This would support the idea of carefully analysing service performance including
documenting the inadequate aspiration rate before
selecting the appropriate intervention to improve
outcomes. However there might be a role for rapid
onsite evaluation when starting a new service which
will require a period of training and mentorship.
Conflict of interest
There are no competing interests
Funding
There was no funding available for this
project
References
- Varadarajulu S, Eloubeidi MA. The role of endoscopic
ultrasonography in the evaluation of pancreaticobiliary cancer. Surg
Clin North Am. 2010;90:251-63.
- Mansfield SD, Scott J, Oppong K, Richardson DL, Sen G, Jaques
BC et al. Comparison of multislice computed tomography and
endoscopic ultrasonography with operative and histological findings
in suspected pancreatic and periampullary malignancy. Br J Surg
2006.;95:1512-20.
- Kala Z, Válek V, Hlavsa J, Hana K, Hana K, Vánová A. The role
of CT and endoscopic ultrasound in pre-operative staging of
pancreatic cancer. Eur J Radiol. 2007;62:166-9.
- Dewitt J, Devereaux BM, Lehman GA, Sherman S, Imperiale TF.
Comparison of endoscopic ultrasound and computed tomography for
the preoperative evaluation of pancreatic cancer: a systematic review.
Clin Gastroenterol Hepatol. 2006;4:717-25
- Eloubeidi MA, Chen VK, Eltoum IA, Jhala D, Chhieng DC, Jhala
N et al. Endoscopic ultrasound-guided fine needle aspiration biopsy
of patients with suspected pancreatic cancer: diagnostic accuracy and
acute and 30-day complications. Am J Gastroenterol. 2003;98:2663-
2670.
- Harewood GC, Wiersema MJ. Endosonography-guided fine needle
aspiration biopsy in the evaluation of pancreatic masses. Am J
Gastroenterol 2002;97:1386-91.
- Turner BG, Cizginer S, Agarwal D, Yang J, Pitman MB, Brugge
WR Diagnosis of pancreatic neoplasia with EUS and FNA: a report
of accuracy. Gastrointest Endosc. 2010;71:91-8.
- Robins DB, Katz RL, Evans DB, Atkinson EN, Green L. Fine
needle aspiration of the pancreas. In quest of accuracy. Acta Cytol.
1995;39:1-10
- Erickson RA, Sayage-Rabie L, Beissner RS. Factors predicting the
number of EUS-guided fine-needle passes for diagnosis of pancreatic
malignancies. Gastrointest Endosc 2000;51:184-90.
- Layfield LJ, Bentz JS, Gopez EV. Immediate on-site
interpretation of fine-needle aspiration smears: a cost and
compensation analysis. Cancer 2001;93:319-22.
- Hall TL, Layfield LJ, Philippe A, Rosenthal DL. Sources of
diagnostic error in fine needle aspiration of the thyroid. Cancer.
1989;63:718-25.
- Austin JH, Cohen MB Value of having a cytopathologist present
during percutaneuous fine-needle aspiration biopsy of lung: report of
55 cancer patients and metaanalysis of the literature. AJR Am J
Roentgenol. 1993;160:175-7.
- Miller DA, Carrasco CH, Katz RL, Cramer FM, Wallace S,
Charnsangavej .Fine needle aspiration biopsy: the role of immediate
cytologic assessment. AJR Am J Roentgenol. 1986;147:155-8.
- Palombini L, Fulciniti F, Vetrani A, De Rosa G, Di Benedetto G,
Zeppa P et al. Fine-needle aspiration biopsies of breast masses. A
critical analysis of 1956 cases in 8 years (1976-1984). Cancer.
1988;61:2273-7.
- Exact confidence limits for p. Geigy Scientific Tables, 7th
Ed.Ciba-Geigy Ltd., Basle: Switzerland, p85-98.
- Volmar KE, Vollmer RT, Jowell PS, Nelson RC, Xie HB.
Pancreatic FNA in 1000 cases: a comparison of imaging modalities.
Gastrointest Endosc 2005;61:854-61.
- Puri R, Vilmann P, Saftoiu A, Skov BG, Linnemann D, Hassan H
et al. Randomized controlled trial of endoscopic ultrasound-guided
fine-needle sampling with or without suction for better cytological
diagnosis Scandinavian Journal of Gastroenterology 2009,;44: 499-
504:
- Krishna NB, Mehra M, Reddy AV, Agarwal B. EUS/EUS-FNA
for suspected pancreatic cancer: influence of chronic pancreatitis and
clinical presentation with or without obstructive jaundice on
performance characteristics. Gastrointest Endosc. 2009;70:70-9.
- Alsibai KD, Denis B, Bottlaender J, Kleinclaus I, Straub P, Fabre
M. Impact of cytopathologist expert on diagnosis and treatment of
pancreatic lesions in current clinical practice. A series of 106
endoscopic ultrasound-guided fine needle aspirations.
Cytopathology. 2006;17:18-26.
- Jhala NC, Jhala DN, Chhieng DC, Eloubeidi MA, Eltoum IA.
Endoscopic ultrasound-guided fine-needle aspiration. A
cytopathologist's perspective. Am J Clin Pathol. 2003;120:351-67.
- Williams DB, Sahai AV, Aabakken L, Penman ID, van Velse A,
Webb J et al. Endoscopic ultrasound guided fine needle aspiration
biopsy: a large single centre experience. Gut 1999;44:720-6.
- Wilson JL, Kalade A, Prasad S, Cade R, Thomson B, Banting S
et al. Diagnosis of solid pancreatic masses by endoscopic ultrasoundguided
fine-needle aspiration. Intern Med J 2009;39:32-7
- Erickson RA. EUS-guided FNA. Gastrointest Endosc
2004;60:267-79.
- LeBlanc JK, Ciaccia D, Al-Assi MT, McGrath K, Imperiale T,
Tao LC et al. Optimal number of EUS-guided fine needle passes
needed to obtain a correct diagnosis. Gastrointest Endosc
2004;59:475-81
- Klapman JB, Logrono R, Dye CE, Waxman I. Clinical impact of
on-site cytopathology interpretation on endoscopic ultrasound-guided
fine needle aspiration. Am J Gastroenterol. 2003;98:1289-94.
- Iglesias-Garcia J, Dominguez-Munoz JE, Abdulkader I, Larino-
Noia J, Eugenyeva E, Lozano-Leon A et al. Influence of On-Site
Cytopathology Evaluation on the Diagnostic Accuracy of
Endoscopic Ultrasound-Guided Fine Needle Aspiration (EUS-FNA)
of Solid Pancreatic Masses. Am J Gastroenterol. 11;106:401-6
- Hwang CY, Lee SS, Song TJ, Moon SH, Lee D, Park do H et al.
Endoscopic ultrasound guided fine needle aspiration biopsy in
diagnosis of pancreatic and peripancreatic lesions: a single center
experience in Korea. Gut Liver. 2009;3:116-21
- Cherian PT, Mohan P, Douiri A, Taniere P, Hejmadi RK, Mahon
BS.Role of endoscopic ultrasound-guided fine-needle aspiration in
the diagnosis of solid pancreatic and peripancreatic lesions: is onsite
cytopathology necessary? HPB (Oxford). 2010 Aug;12(6):389-95.
- Itoi T, Tsuchiya T, Itokawa F, Sofuni A, Kurihara T, Tsuji S et
al. Histological diagnosis by EUS-guided fine-needle aspiration biopsy in pancreatic solid masses without on-site cytopathologist: a
single-center experience. Dig Endosc. 2011;23:34-8.
- Hikichi T, Irisawa A, Bhutani MS, Takagi T, Shibukawa G,
Yamamoto G et al. Endoscopic ultrasound-guided fine-needle
aspiration of solid pancreatic masses with rapid on-site cytological
evaluation by endosonographers without attendance of
cytopathologists. J Gastroenterol. 2009;44:322-8.
- Alsohaibani F, Girgis S, Sandha GS. Does onsite cytotechnology
evaluation improve the accuracy of endoscopic ultrasound-guided
fine needle aspiration biopsy? Can J Gastroenterol 2009;23:26–30.
- Savoy AD, Raimondo M, Woodward TA, Noh K, Pungpapong S,
Jones AD et al. Can endosonographers evaluate on-site cytologic
adequacy? A comparison with cytotechnologists.. Gastrointest
Endosc. 2007 Jun;65(7):953-7.
- Lee JK, Choi ER, Jang TH, Chung YH, Jang KT, Park SM et al.
A prospective comparison of liquid-based cytology and traditional
smear cytology in pancreatic endoscopic ultrasound-guided fine
needle aspiration. Acta Cytol. 2011;55(5):401-7. Epub 2011 Oct 8.
- Nicholson S, Sainsbury JR, Wadehra V, Needham GK, Farndon
JR. Use of fine needle aspiration cytology with immediate reporting
in the diagnosis of breast disease.. Br J Surg. 1988 Sep;75(9):847-50.
- Veale D, Gilmartin JJ, Sumerling MD, Wadehra V, Gibson GJ.
Prospective evaluation of fine needle aspiration in the diagnosis of
lung cancer. Thorax. 1988 Jul;43(7):540-4.
- Swinburn CR, Veale D, Peel ET, Wadehra V, Elliott ST,
Sumerling MD et al. A prospective randomized comparison of fine
needle aspiration biopsy and fibreoptic bronchoscopy in the
investigation of peripheral pulmonary opacities.. Respir Med. 1989
Nov;83(6):493-5.
- Petrone MC, Arcidiacono PG, Carrara S, Mezzi G, Doglioni C,
Testoni PA. Does cytotechnician training influence the accuracy of
EUS-guided fine-needle aspiration of pancreatic masses? Dig Liver
Dis. 2012 Apr;44(4):311-4.
- Nayar M, Joy D, Wadehra V, Oppong KE. Effect of dedicated
and supervised training on achieving competence in EUS-FNA of
solid pancreatic lesions. Scand J Gastroenterol. 2011; 46:1-7.
- Weynand B, Borbath I, Galant C, Piessevaux H, Deprez PH.
Optimizing specimen collection and laboratory procedures reduces
the non-diagnostic rate for endoscopic ultrasound-guided fine-needle
aspiration of solid lesions of the pancreas.Cytopathology
2011;10:1365-2303
- Cleveland P, Gill KR, Coe SG, Woodward TA, Raimondo M,
Jamil L et al. An evaluation of risk factors for inadequate cytology in
EUS-guided FNA of pancreatic tumors and lymph nodes..
Gastrointest Endosc. 2010 Jun;71(7):1194-9

