Keywords
Mortality; surgery
Abbreviations
BMI body mass index; CI confidence interval; DGE delayed gastric emptying; POPF post-operative pancreatic fistula; PPH post-pancreatectomy haemorrhage; RR relative risk; VFA visceral fat area
INTRODUCTION
The incidence of obesity is increasing the world over [1]. Obesity is a well-known risk factor for cardiovascular disease, hypertension, diabetes and certain malignancies like colon, ovary, endometrium, prostrate and breast [2-6]. Recent evidence has not only suggested obesity to play a role in the development of pancreatic cancer [7-11], but also adversely affect outcomes in patients who undergo surgery for the cancer [12, 13].
Pancreatoduodenectomy (PD), performed for pancreatic head and neck cancers is a procedure fraught with the risk of morbidity [14] and mortality. Important factors related to the development of the complications include the texture of the gland (firm or soft) [15], size of the pancreatic duct [16], and surgeon-determined factors such as choice of suture-material [15] and methods of reconstruction [17], amongst others. While fatty infiltration of the pancreas has been suggested to be a determinant of perioperative pancreatic surgical outcomes [18], this is not uniformly reported [19-21].
Several studies have directly examined the impact of a high body mass index (BMI) on outcomes following pancreatic resection. However, their small sample sizes and inconsistent findings have limited the interpretation of their findings. Despite this, it is important for us to appreciate that over the next few years the number of PDs being performed on obese patients is likely to increase and hence we need to objectively determine if obesity influences morbidity following pancreatic surgery. Once such an association is developed, it may enable us to understand the factors leading to these altered outcomes and this could potentially help us to develop strategies aimed at minimising these risks.
This systematic review and meta-analysis examines the evidence in the literature with an aim to determining the impact of obesity on perioperative surgical outcomes in patients undergoing pancreatic surgery for malignant as well as benign conditions of the pancreas.
METHODS
A literature search was conducted using PubMed, Medline, Cochrane and Embase databases, using the search terms “pancreatic surgery”, “pancreatoduodenectomy”, “pancreaticoduodenectomy”, “obesity”, “BMI”, “body mass index”, “surgical outcome”, “postoperative complications”, “complications” from January 1990 to June 2013 without any restrictions. All publications from past 23 years were considered for review.
Inclusion Criteria
The criteria for including manuscripts in this review were as follows
(1) Participants – Human subjects undergoing pancreatic surgery,
(2) Intervention – Pancreatic surgery for benign as well as malignant diseases
(3) Comparative variables – Pre-operative BMI/Visceral fat (VF) / Visceral Fat Area (VFA) / Abdominal Wall Fat (AWF) / Total Fat Area (TFA) with peri-operative variables
(4) Outcomes data – A. Perioperative variables – Blood loss, operating time, lymph node number, tumor size. B. Postoperative variables – Overall postoperative complications and specific complications (as defined by the authors) such as, pancreatic fistula (POPF), Delayed gastric emptying (DGE), intra-abdominal abscess, wound infection, bleeding (PPH), re-laparotomy, in-hospital stay, non-operative complications
(5) Types of study – Prospective studies and retrospective studies. In addition, the bibliography of each manuscript was examined and cross-referenced for relevant publications.
Exclusion Criteria
Review articles, letters/comments and editorials were excluded.
Abstracts of citations identified from the literature search were assessed for eligibility for inclusion in this systematic review. The data was arranged in a prespecified spread sheet. Any disagreement was resolved by discussion between the authors.
Quality Analysis
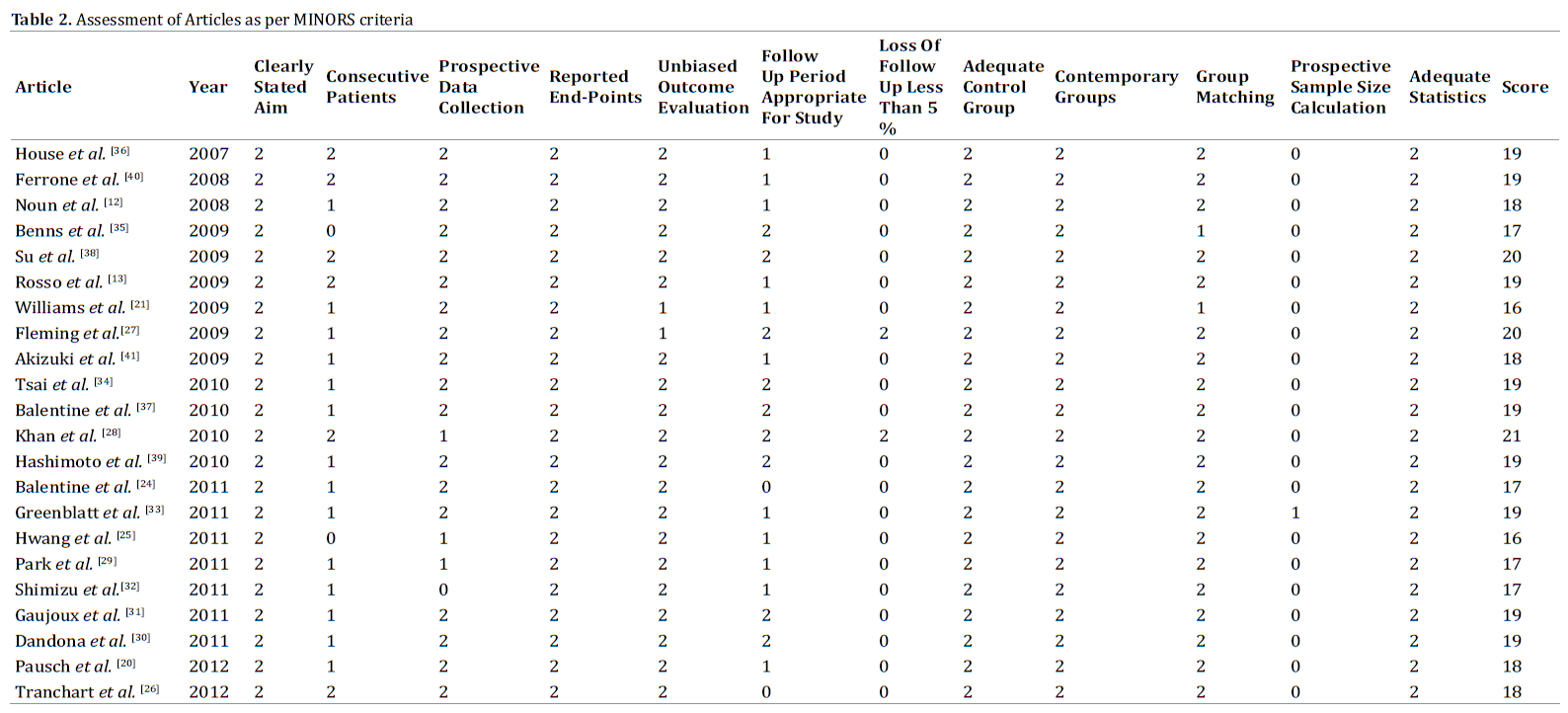
Since all the studies included in the analysis were nonrandomised studies, in order to objectively assess the quality of the studies included we used the Methodological Index for Nonrandomized Studies (MINORS) – a validated tool for the evaluation of non-randomised studies [22]. Studies with 12 or more points were considered as high quality and were included in the analysis.
Statistical Analysis
This study was performed in line with the recommendations of the Preferred Reporting Items for Systematic reviews and Meta-Analysis (PRISMA) Statement [23]. The study included 14 Non-randomised experimental studies reporting primary outcome and 8 studies reporting one or more of the secondary outcome measures. All the patients included in these studies were hospitalised patients. Initially, Funnel plots were created to confirm the heterogeneity of the eligible studies. After satisfying the heterogeneity, further analysis was attempted. The main outcome measure was identified as post-operative pancreatic fistula. The secondary outcome measures were restricted to overall complications and wound infection as other complications were inconsistently reported.
The meta-analysis followed the Binary Fixed-Effect - Mantel Haenszel model and was carried out with the OpenMeta [Analyst] software. Relative risk, confidence intervals, and tests of significance were derived from fixed effects model. The analysis was carried out separately considering BMI more than 30 and BMI more than 25 as obesity criteria and were compared to non-obese group (BMI<25). These study estimates were combined in order to obtain a single estimate for decision making. The estimated effect measure was Relative Risk. Betweenstudy heterogeneity assessed using Cochran Q statistic was significant. Subgroup analysis was carried out for primary outcome only. The Forest plots made indicates the Relative risk among obese individuals (BMI more than 30 and BMI more than 25). RR of 1 (one) indicate that the risk is equal in both the groups and >1 (more than one) indicate increased risk; less than 1 denotes decreased risk of complications.
RESULTS
Using the above search strategy, a total of 598 publications / articles were retrieved of which 22 studies (Figure 1 – Quorum Chart) were identified describing the impact of obesity on perioperative outcomes following PD [12, 13, 20, 21, 24-41]. Table 1 lists the various studies by their level of evidence.

Quality Assessment
Using the MINORS tool, all 22 studies had a score of more than 16 (Table 2) and were included in the analysis.
Patient and Surgical Demography
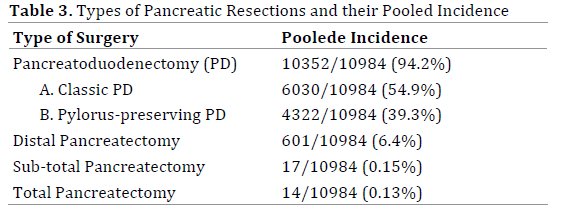
The analysis was based on a pooled sample size of 10,984 patients derived from retrospective analysis of prospectively maintained databases. Table 3 lists the various surgical procedures performed. The indications for the surgical procedures are provided in (Table 4).

Peri-Operative Outcomes
Operating Time: While 9 out of 22 studies reported no increase in operative time associated with increasing BMI/VFA [12, 20, 25, 27, 29, 31, 34-36] (Normal BMI group: 210–443 min vs. Obese group: 402–464 min; p-not significant}, 5 studies reported an increase in OT with increasing BMI [21, 24, 28, 32, 38] (Normal BMI group: 185-363 min vs. Obese group: 438-723 min; p<0.05). 8 other studies, however, lacked data on the association between obesity and operating time [13, 26, 30, 33, 37, 39-41].
Peri-Operative Blood Loss: 10 out of 22 studies reported a significant increase in blood loss with increasing BMI/ VFA [20, 21, 25, 27-29, 31, 32, 34, 35] (Normal BMI group: 300–1020 ml vs. Obese group: 650–1255 ml; p<0.05) while 10 studies lacked data about the association of perioperative blood loss and BMI[12, 13, 24, 26, 30, 33, 37, 39-41]. Su et al. [38] and House et al. [36] did not find an increase in blood loss with increasing BMI (Normal BMI group: 595–719 ml vs. Obese group: 686–881 ml; p-not significant).
Total Lymph Nodes Harvested: 5 of the 22 studies reported on the differences in total lymph nodes harvested between patients with a normal or low BMI and those with an elevated BMI above normal [27, 28, 31, 34, 35] (Normal BMI group: 9.5-19 vs. Obese group: 11-20; p-not significant). In all 5 studies, no significant differences in the total number of harvested lymph nodes were reported.
Nature of Pancreatic disease: Of the 22 studies, 80% of pancreatic resections were performed for malignancy (Table 4). 10 studies considered only malignant pancreatic disease [20, 26-28, 30, 31, 34-37], of which 9 studies included subjects exclusively with pancreatic ductal adenocarcinoma [20, 27, 28, 30, 31, 34-37]. 11 studies included patients with benign and malignant pancreatic disease [12, 13, 21, 25, 29, 32, 33, 38-41] while in a single study, the nature of disease was not specified [24].
Of these, 4 studies compared post-operative surgical outcome to the nature of the pancreatic disease [29, 33, 34, 39] of which 2 studies compared occurrence of POPF [29, 39]. Park et al. [29] concluded that POPF incidence was high in cancer of non-pancreatic origin, namely Ampulla, bile duct and duodenu)m (p=0.015). However, POPF occurrence was independent of the nature of primary pancreatic pathology. Hashimoto et al. [39], too, failed to note an increased incidence of POPF depending on the pathology (p=0.383).
Tsai et al. [34] found that obesity (BMI > 30kg/m2) was associated with better disease-specific survival rate (HR – 0.73, p < 0.01).
Stage of the Pancreatic Malignancy: Of the 22 studies included, 6 studies mentioned about the stage of the pancreatic malignancy [20, 27, 28, 31, 34, 37]. In all these studies, there was predominantly Stage II disease (75.8% - 97.3%). 3 studies [20, 28, 34] compared cancer stage amongst different BMI groups and found no significant difference.
There was no direct comparison of stage of pancreatic malignancy to peri-operative surgical outcomes in any of these studies.
Morbidity Rate: An overall morbidity rate of 5 - 67.6% was reported across studies.
Benns et al. [35] reported a significantly increased risk (p=0.01) and severity of post-operative morbidity in patients with a BMI of more than 30kg/m2 (Severity score - obese: 1.6, non-obese: 1.2, p=0.02). Pausch et al. [20], on the other hand, reported that pre-operative weight-loss (> 10% of body weight), rather than obesity, per se, was associated with an increased post-operative morbidity (p<0.03). 9 of the 22 studies reported no increase in postoperative morbidity associated with an increase in BMI [12, 20, 21, 24, 27, 28, 31, 34, 36] (Normal BMI group: 11-40.2% vs. Obese group: 5-67.6 %; p-not significant) while 11 out of 22 studies lacked data regarding the influence of BMI on post-operative morbidity [25, 26, 29, 30, 32, 36-38, 40, 41, 43]. Greenblatt et al. [33], too, reported that a BMI of >25kg/m2 was predictive of postoperative morbidity in patients undergoing PD (odds ratio (OR)-1.27 90%CI).
The overall post-operative complication rate among obese and non-obese individuals is shown in Figure 2. The overall complication rate among obese individuals is 1.194 times more than that of non-obese individuals. However, the risk was not found to be statistically significant (RR=1.194; CI=1.069-1.334, p=0.647).
Figure 2. Forest Plot of Relative Risk for Overall Complications among Obese Individuals.
Post-operative Pancreatic Fistula: An overall POPF incidence rate of 2 - 54.3% was reported across studies. In 7 studies [12, 25, 26, 29, 34, 39, 40], a significant association was noted between a raised BMI and the occurrence of POPF(Normal BMI group: 2.9-33.6% vs. Obese group: 9.4-54.3%; p<0.05) while in three studies [26, 29, 32] an increasing VFA was found to correlate with the occurrence of clinically significant POPF. A BMI >25 was determined to be an independent risk factor for POPF occurrence [13, 25, 26, 29, 32]. Rosso et al. [13] actually found that a BMI >25 was linked to risk of clinically significant POPF.
VF thickness, rather than BMI (>30kg/m2), was found to be associated with the development of POPF [36].
Conversely, 4 other studies, found no correlation between the development of POPF and either abdominal fat / VF (17% vs. 11%, p-not significant) [24] or elevated BMI [21, 38, 41] (Normal BMI group: 4-18.8% vs. Obese group: 2-13%; p-not significant).
In 8 studies, no data on the association of obesity and POPF occurrence could be determined [20, 27, 28, 30, 31, 33, 35, 37].
Relative risk of developing POPF among obese and nonobese individuals is shown in Figures 3-5. Few authors considered BMI > 30 as obese while others considered BMI>25 as obesity criteria. Hence the data was regrouped and the studies defining obesity as BMI >30 analysed separately from those defining obesity as BMI > 25. The plot in Figure 3 indicates the relative risk of POPF among obese (BMI ≥30) and non-obese individuals (BMI < 25). The overall relative risk rate was 1.61 (CI=1.259-2.062) indicating that obese individuals are 1.6 times more at risk of developing POPF compared to non-obese individuals. The forest plot in Figure 4 indicates the relative risk of post-operative pancreatic fistula among obese (BMI ≥ 25) and non-obese (BMI<25) individuals. Obese individuals (with BMI ≥ 25) are at a 2.2 times (relative risk=2.169; CI=1.572-2.994) more risk for developing POPF compared to non-obese individuals. It also emphasizes that the postoperative risk of POPF becomes more prominent when the cut-off BMI value is considered to be ≥ 25. Hence, a combined plot was prepared to find out the change in the risk ratio of POPF among obese and non-obese individuals (Figure 5). The overall risk ratio shows 1.808 (CI=1.487-2.198).
Figure 3. Forest Plot of Relative Risk for Developing Pancreatic Fistula in Studies Defining Obesity as BMI>30.
Figure 4. Forest Plot of Relative Risk for Developing POPF in Studies Defining Obesity as BMI>25.
Figure 5. Forest Plot of Relative Risk for Pancreatic Fistula Combining All Studies.
Delayed Gastric Emptying: An overall DGE incidence rate of 4- 53% was reported across studies.
Only one study noted a significant association between increasing VFA and DGE [29] (p=0.014). In 8 other studies, no correlation was noted between the development of DGE and either increasing BMI [12, 25, 34, 36, 39, 41] (Normal BMI group: 4 – 42% vs. Obese group: 10.5–53%; p-not significant), increasing VFA [24] or increasing VF/ intra-abdominal fat [32].
13 studies lacked data about association between DGE occurrence and increasing BMI [13, 20, 21, 26-28, 30, 31, 33, 35, 37, 38, 40].
Post-Pancreatectomy Haemorrhage: An overall PPH incidence rate of 0 – 10.5% was reported across studies.
Data on the relation between PPH and obesity was available in only four of the 22 studies. No increased risk of PPH was noted to correlate with increasing BMI, intraabdominal fat / VF or VFA in all the four studies [12, 24, 29, 32] (Normal BMI group: 0-6.8% vs. Obese group: 1.2–10.5%; p-not significant).
Post-Operative Intra-Abdominal Abscess: An overall post-operative intra-abdominal abscess incidence rate of 1.7 – 40% was reported across studies.
Williams et al. [21] reported a significantly higher incidence of post-operative intra-abdominal abscess in the obese group (14% vs. 7%; p=0.05) as compared to patients with a normal BMI. Similarly, Su et al. [38], too, found that a BMI >25 was an independent risk factor for developing post-operative infectious complications (7.9% vs. 3.9%, OR=6.5, p=0.005). Four other studies, however, reported no association between occurrence of post-operative intra-abdominal abscess and increasing BMI, VFA or VF [12, 24, 32, 41] (Normal BMI group: 1.7–30% vs. Obese group:2–40%; p-not significant).
Pausch et al. [20], instead reported that patients with larger AWF had fewer post-operative intra-abdominal abscess compared to those with smaller AWF (7.1% vs. 1.7%; p=0.047).
In 15 studies no data comparing the association between post-operative intra-abdominal abscess and increasing BMI could be determined [13, 25-31, 33-37, 39, 40].
Post-Operative Wound Infection: An overall postoperative wound infection incidence rate of 3.9 - 15.8 % was reported across studies.
While nine studies reported no increased incidence of post-operative wound infection with an increasing BMI/ VFA [12, 21, 24, 25, 29, 32, 34, 35, 41] (Normal BMI group: 3.9-11% vs. Obese group: 5–15.8%; p-not significant), House et al. [36] reported that BMI>30 was an independent predictor of post-operative wound infection (hazards ratio: 1.1; p=0.03) with a significant correlation between VF thickness and post-operative wound infection.
A higher incidence of wound infections was noted in obese individuals as compared to those who are non-obese (Figure 6; relative risk=1.69 (CI=1.225-2.274)).
Figure 6. Forest Plot Showing Relative Risk of Wound Infection among Obese and Non-Obese Group.
Non-Operative Complications: Shimizu et al. [32] reported a significant increase in post-operative pulmonary complications in patients with a high VFA on multivariate analysis (p=0.04, OR-4.246).
In-Hospital Stay: While Park et al. [29] reported no increased length of stay amongst patients with a high VFA (28.2 vs. 26 days; p-NS), two out of 22 studies reported a significantly increased hospital stay in obese patients [12, 21](Normal BMI group: 8-17 days vs. Obese group: 9.5– 23.1 days; p<0.05). In 6 of the 22 studies, it was noted that there existed no significant difference in length of hospital stay among different BMI groups [20, 25, 27, 28, 34, 35, 38](Normal BMI group: 9–23 days vs. Obese group: 10–25 days; p-not significant).
Centre Surgical Volume: 21 of the 22 articles were based on single institution data [12, 13, 20, 21, 24-32, 34-41] except for the publication by Greenblat et al. [33] which used data from the American College of Surgeons National Surgical Quality Improvement Program (ACS NSQIP) database. In the 21 studies, the number of resections per year varied from 7 to 80.
DISCUSSION
Obesity is on the rise the world over and has assumed epidemic proportions [44]. Moreover, a pooled analysis of 7 prospective cohort studies indicated that a high BMI was an independent risk factor for pancreatic cancer [45]. A previous meta-analysis on the impact of BMI on outcomes of pancreatic surgery indicated that obesity increased the complexity of surgery and the development of POPF but did not significantly influence other parameters [46]. This meta-analysis solely looked at BMI and its influence on perioperative outcomes. However, studies have shown [29, 32] that it is the visceral fat area, more than the BMI, which can potentially influence outcomes. More importantly, there may not be a direct correlation between BMI and visceral fat [29, 32]. Thus, till clearer evidence emerges on which constitutes a better parameter for assessing the impact of obesity on surgical variables, it would be prudent to at least assess both BMI and VF/VFA.
Given an appreciation of the scenario that we will be seeing an increase in the number of obese patients undergoing surgery for pancreatic tumours, it is essential to determine if, and how, obesity would influence perioperative outcomes. This information can aid the development of strategies to minimize any such negative influences of obesity on pancreatic surgical outcomes.
Fatty infiltration of the pancreas as a risk factor for poor outcomes following pancreaticoenteric anastomosis has been well appreciated [18]. This review confirms that while obesity does not significantly increase the risk for overall complications following pancreatic surgery, there is certainly an increased risk of POPF in obese patients or patients with an elevated VFA [12, 25, 26, 29, 34, 39, 40]. In fact, a BMI ≥ 25 was determined to be an independent risk factor for POPF occurrence [13, 25, 26, 29, 32]. Future randomised studies are needed to determine the best method for reconstructing the pancreaticoenteric anastomosis in PD depending on the texture of the pancreatic gland [17]. Obesity also results in an increased risk of wound infections following pancreatic surgery.
Obesity is not associated with a prolonged duration of surgery but may contribute to increased intra-operative blood loss and hence the need for blood transfusions [20, 21, 25, 27-29, 31, 32, 34, 35]. On closer analysis, VFA rather than merely an elevated BMI, influences the technical difficulty of the procedure and the increased blood loss [29, 32] following pancreatic surgery. Thus, meticulous technique may help reduce the blood loss in obese patients possibly at the expense of an increased operative time.
Obesity certainly does not appear to interfere with the extent of dissection in patients undergoing pancreatic surgery as per the lack of significant difference between the lymph nodes harvested in these patients (9.5-19 vs. 11- 20; p–not significant) [27, 28, 31, 34, 35].
An important finding in this review is the potential for obese patients to develop pulmonary complications [32]. These findings stress the importance of development of clinical pathways prior to-, as well as, following pancreatic surgery focusing on the incorporation of chest physiotherapy to help reduce the development of such problems which may arise due to poor breathing efforts associated with obesity and also post-operative pain.
Obesity or increased visceral fat was not found to influence the development of other complications following pancreatic surgery. Considering that the data included in the review has emerged from high-volume pancreatic centres, it can be well appreciated that the lack of effect of obesity on the vast majority of perioperative variables may be a reflection of standardization in surgical technique [47] pre-existent in these centres – a valuable lesson for new, as well as, low-volume centres who perform pancreatic resectional surgery. The effect of obesity on enhanced recovery protocols following PD is just beginning to be understood with a recent study suggesting the need to tailor the existing enhanced recovery protocols following PD to patients with raised BMI and respiratory co-morbidities [48].
One of the short-comings of the analysis is the inherent heterogeneity in the studies available. Studies included different types of pancreatic resections (PD, distal pancreatectomy, total and subtotal pancreatectomy), varied indications (malignant and benign disease) and different parameters for assessing the impact of body fat content (BMI, VF, VFA). This, however, reflects the nonselective reporting of data in literature. Any attempt to subdivide these into outcomes for each surgery, indication or parameter assessed would not have been possible.
The strength of this study rests in an exhaustive literature review to identify manuscripts that compared outcomes following pancreatic surgery between patients with a normal BMI and those with an elevated BMI. Due attention to the heterogeneity of data was taken into consideration when performing the meta-analysis. Moreover, manuscripts included were subjected to an objective (MINORS) assessment tool to determine the quality of the manuscripts. The data included is from studies that can be defined as “high-volume” centres having recorded more than 5 pancreatic resections per year [49] (7-80 resections per year).
CONCLUSIONS
This study summarizes the highest quality of evidence currently available comparing perioperative outcomes following pancreatic surgery between individuals with low to normal BMI and those with an elevated BMI. The evidence suggests that obesity increases the risk of POPF and wound infections but does not increase operating time or influence the development of DGE, PPH and intraabdominal collections. Obesity contributes to an increase in intra-operative blood loss but does not impair the performance of a standard lymphadenectomy.
Conflict of interest
All the authors have no conflicts of interest
References
- Swinburn B, Sacks G, Hall K, McPherson K, Finegood D, Moodie M, Gortmaker S. The global obesity pandemic: Shaped by global drivers and local environments. Lancet 2011; 378:804-814. [PMID: 21872749]
- Carmichael AR. Obesity and prognosis of breast cancer. Obes Rev 2006; 7:333-340. [PMID: 17038127]
- Dignam JJ, Polite BN, Yothers G, Raich P, Colangelo L, O'Connell MJ, Wolmark N. Body mass index and outcomes in patients who receive adjuvant chemotherapy for colon cancer. J Natl Cancer Inst 2006; 98:1647-1654. [PMID: 17105987]
- Gong Z, Agalliu I, Lin DW, Stanford JL, Kristal AR. Obesity is associated with increased risks of prostate cancer metastasis and death after initial cancer diagnosis in middle-aged men. Cancer 2007; 109:1192-1202. [PMID: 17311344]
- Kjaerbye-Thygesen A, Frederiksen K, Hogdall EV, Glud E, Christensen L, Hogdall CK, Blaakaer J, Kjaer SK. Smoking and overweight: Negative prognostic factors in stage iii epithelial ovarian cancer. Cancer Epidemiol Biomarkers Prev 2006; 15:798-803. [PMID: 16614126]
- von Gruenigen VE, Tian C, Frasure H, Waggoner S, Keys H, Barakat RR. Treatment effects, disease recurrence, and survival in obese women with early endometrial carcinoma : A gynecologic oncology group study. Cancer 2006; 107:2786-2791. [PMID: 17096437]
- Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of u.S. Adults. N Engl J Med 2003; 348:1625-1638. [PMID: 12711737]
- Hanley AJ, Johnson KC, Villeneuve PJ, Mao Y. Physical activity, anthropometric factors and risk of pancreatic cancer: Results from the canadian enhanced cancer surveillance system. Int J Cancer 2001; 94:140-147. [PMID: 11668489]
- Larsson SC, Permert J, Hakansson N, Naslund I, Bergkvist L, Wolk A. Overall obesity, abdominal adiposity, diabetes and cigarette smoking in relation to the risk of pancreatic cancer in two swedish population-based cohorts. Br J Cancer 2005; 93:1310-1315. [PMID: 16288300]
- Li D. Diabetes and pancreatic cancer. Mol Carcinog 2012; 51:64-74. [PMID: 22162232]
- Michaud DS, Giovannucci E, Willett WC, Colditz GA, Stampfer MJ, Fuchs CS. Physical activity, obesity, height, and the risk of pancreatic cancer. JAMA 2001; 286:921-929. [PMID: 11509056]
- Noun R, Riachy E, Ghorra C, Yazbeck T, Tohme C, Abboud B, Naderi S, et al. The impact of obesity on surgical outcome after pancreaticoduodenectomy. JOP 2008; 9:468-476. [PMID: 18648138]
- Rosso E, Casnedi S, Pessaux P, Oussoultzoglou E, Panaro F, Mahfud M, Jaeck D, et al. The role of "fatty pancreas" and of bmi in the occurrence of pancreatic fistula after pancreaticoduodenectomy. J Gastrointest Surg 2009; 13:1845-1851. [PMID: 19639369]
- Shukla P, Barreto S, Shrikhande S. The evolution of pancreatoduodenectomy. Hepatogastroenterology 2011; 58:1409-1412. [PMID: 21937418]
- Shrikhande SV, Qureshi SS, Rajneesh N, Shukla PJ. Pancreatic anastomoses after pancreaticoduodenectomy: Do we need further studies? World J Surg 2005; 29:1642-1649. [PMID: 16311866]
- Shukla PJ, Barreto SG, Fingerhut A. Do transanastomotic pancreatic ductal stents after pancreatic resections improve outcomes? Pancreas 2010; 39:561-566. [PMID: 20562577]
- Shukla PJ, Barreto SG, Fingerhut A, Bassi C, Buchler MW, Dervenis C, Gouma D, Izbicki JR, Neoptolemos J, Padbury R, Sarr MG, Traverso W, Yeo CJ, Wente MN. Toward improving uniformity and standardization in the reporting of pancreatic anastomoses: A new classification system by the international study group of pancreatic surgery (isgps). Surgery 2010; 147:144-153. [PMID: 19879614]
- Mathur A, Pitt HA, Marine M, Saxena R, Schmidt CM, Howard TJ, Nakeeb A, et al. Fatty pancreas: A factor in postoperative pancreatic fistula. Ann Surg 2007; 246:1058-1064. [PMID: 18043111]
- Lermite E, Pessaux P, Brehant O, Teyssedou C, Pelletier I, Etienne S, Arnaud JP. Risk factors of pancreatic fistula and delayed gastric emptying after pancreaticoduodenectomy with pancreaticogastrostomy. J Am Coll Surg 2007; 204:588-596. [PMID: 17382217]
- Pausch T, Hartwig W, Hinz U, Swolana T, Bundy B, Hackert T, Grenacher L, et al. Cachexia but not obesity worsens the postoperative outcome after pancreatoduodenectomy in pancreatic cancer. Surgery 2012; 152: 81-88. [PMID: 22770957]
- Williams TK, Rosato EL, Kennedy EP, Chojnacki KA, Andrel J, Hyslop T, Doria C, et al. Impact of obesity on perioperative morbidity and mortality after pancreaticoduodenectomy. J Am Coll Surg 2009; 208:210-217. [PMID: 19228532]
- Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index for non-randomized studies (minors): Development and validation of a new instrument. ANZ J Surg 2003; 73:712-716. [PMID: 12956787]
- Liberati A, Altman D, Tetzlaff J, Mulrow C, Gøtzsche PC, Ioannidis JP, Clarke M, et al. The prisma statement for reporting systematic reviews and meta-analyses of studies that evaluate health care interventions: Explanation and elaboration. Ann Intern Med 2009; 151: 65-94. [PMID:19622512]
- Balentine CJ, Enriquez J, Cruz G, Hodges S, Bansal V, Jo E, et al. Obesity does not increase complications following pancreatic surgery. J Surg Res 2011; 170:220-225. [PMID: 21514600]
- Hwang HK, Park JS, Park CI, Kim JK, Yoon DS. The impact of body mass index on pancreatic fistula after pancreaticoduodenectomy in asian patients on the basis of asia-pacific perspective of body mass index. JOP 2011; 12:586-592. [PMID: 22072248]
- Tranchart H, Gaujoux S, Rebours V, Vullierme MP, Dokmak S, Levy P, et al. Preoperative ct scan helps to predict the occurrence of severe pancreatic fistula after pancreaticoduodenectomy. Ann Surg 2012; 256:139-145. [PMID: 22609844]
- Fleming JB, Gonzalez RJ, Petzel MQ, Lin E, Morris JS, Gomez H, Lee JE, et al. Influence of obesity on cancer-related outcomes after pancreatectomy to treat pancreatic adenocarcinoma. Arch Surg 2009; 144:216-221. [PMID: 19289659]
- Khan S, Sclabas G, Reid-Lombardo K, Sarr MG, Nagorney D, Kendrick ML, Que FG, et al. Does body mass index/morbid obesity influence outcome in patients who undergo pancreatoduodenectomy for pancreatic adenocarcinoma? J Gastrointest Surg 2010; 14:1820-1825. [PMID: 20676790]
- Park CM, Park JS, Cho ES, Kim JK, Yu JS, Yoon DS. The effect of visceral fat mass on pancreatic fistula after pancreaticoduodenectomy. J Invest Surg 2012; 25:169-173. [PMID: 22583013]
- Dandona M, Linehan D, Hawkins W, Strasberg S, Gao F, Wang-Gillam A. Influence of obesity and other risk factors on survival outcomes in patients undergoing pancreaticoduodenectomy for pancreatic cancer. Pancreas 2011; 40:931-937. [PMID: 21747317]
- Gaujoux S, Torres J, Olson S, Winston C, Gonen M, Brennan MF, Klimstra DS, et al. Impact of obesity and body fat distribution on survival after pancreaticoduodenectomy for pancreatic adenocarcinoma. Ann Surg Oncol 2012; 19:2908-2916. [PMID: 22411205]
- Shimizu A, Tani M, Kawai M, Hirono S, Miyazawa M, Uchiyama K, Yamaue H. Influence of visceral obesity for postoperative pulmonary complications after pancreaticoduodenectomy. J Gastrointest Surg 2011; 15:1401-1410. [PMID: 21567293]
- Greenblatt DY, Kelly KJ, Rajamanickam V, Wan Y, Hanson T, Rettammel R, Winslow ER, Cho CS, et al. Preoperative factors predict perioperative morbidity and mortality after pancreaticoduodenectomy. Ann Surg Oncol 2011; 18:2126-2135. [PMID: 21336514]
- Tsai S, Choti MA, Assumpcao L, Cameron JL, Gleisner AL, Herman JM, Eckhauser F, et al. Impact of obesity on perioperative outcomes and survival following pancreaticoduodenectomy for pancreatic cancer: A large single-institution study. J Gastrointest Surg 2010; 14:1143-1150. [PMID: 20431978]
- Benns M, Woodall C, Scoggins C, McMasters K, Martin R. The impact of obesity on outcomes following pancreatectomy for malignancy. Ann Surg Oncol 2009; 16:2565-2569. [PMID: 19557479]
- House MG, Fong Y, Arnaoutakis DJ, Sharma R, Winston CB, Protic M, Gonen M, et al. Preoperative predictors for complications after pancreaticoduodenectomy: Impact of bmi and body fat distribution. J Gastrointest Surg 2008; 12:270-278. [PMID: 18060467]
- Balentine C, Enriquez J, Fisher W, Hodges S, Bansal V, Sansgiry S, Petersen N, Berger D. Intra-abdominal fat predicts survival in pancreatic cancer. J Gastrointest Surg 2010; 14:1832-1837. [PMID: 20725799]
- Su Z, Koga R, Saiura A, Natori T, Yamaguchi T, Yamamoto J. Factors influencing infectious complications after pancreatoduodenectomy. J Hepatobiliary Pancreat Sci 2010; 17:174-179. [PMID: 19517055]
- Hashimoto Y, Traverso LW. Incidence of pancreatic anastomotic failure and delayed gastric emptying after pancreatoduodenectomy in 507 consecutive patients: Use of a web-based calculator to improve homogeneity of definition. Surgery 2010; 147:503-515. [PMID: 20018335]
- Ferrone CR, Warshaw AL, Rattner DW, Berger D, Zheng H, Rawal B, Rodriguez R, et al. Pancreatic fistula rates after 462 distal pancreatectomies: Staplers do not decrease fistula rates. J Gastrointest Surg 2008; 12:1691-1697. [PMID: 18704597]
- Akizuki E, Kimura Y, Nobuoka T, Imamura M, Nagayama M, Sonoda T, Hirata K Reconsideration of postoperative oral intake tolerance after pancreaticoduodenectomy: Prospective consecutive analysis of delayed gastric emptying according to the isgps definition and the amount of dietary intake. Ann Surg 2009; 249:986-994. [PMID: 19474680]
- Wright JG, Swiontkowski MF, Heckman JD. Introducing levels of evidence to the journal. J Bone Joint Surg Am 2003; 85:1-3. [PMID: 12533564]
- Sakuramoto S, Sasako M, Yamaguchi T, Kinoshita T, Fujii M, Nashimoto A, Furukawa H, et al. Adjuvant chemotherapy for gastric cancer with s-1, an oral fluoropyrimidine. N Engl J Med 2007; 357:1810-1820. [PMID: 17978289]
- James WP. The epidemiology of obesity: The size of the problem. J Intern Med 2008; 263:336-352. [PMID: 18312311]
- Jiao L, Berrington de Gonzalez A, Hartge P, Pfeiffer RM, Park Y, Freedman DM, Gail MH, et al. Body mass index, effect modifiers, and risk of pancreatic cancer: A pooled study of seven prospective cohorts. Cancer Causes Control 2010; 21:1305-1314. [PMID: 20383573]
- Ramsey AM, Martin RC. Body mass index and outcomes from pancreatic resection: A review and meta-analysis. J Gastrointest Surg 2011; 15:1633-1642. [PMID: 21484490]
- Shrikhande SV, Barreto SG, Somashekar BA, Suradkar K, Shetty GS, Talole S, Sirohi B, et al. Evolution of pancreatoduodenectomy in a tertiary cancer center in india: Improved results from service reconfiguration. Pancreatology 2013; 13:63-71. [PMID: 23395572]
- Chaudhary A, Barreto S, Talole S, Singh A, Perwaiz A, Singh T. Early discharge after pancreatoduodenectomy - what helps and what prevents? Pancreas 2015; 44:273-278. [PMID: 25479587]
- Birkmeyer JD, Warshaw AL, Finlayson SR, Grove MR, Tosteson AN. Relationship between hospital volume and late survival after pancreaticoduodenectomy. Surgery 1999; 126:178-183. [PMID: 10455881]







