Keywords
Fibrin Tissue Adhesive; Pancreatoduodenectomy
Abbreviation
FRS fistulae risk score; LOS length of stay; PD pancreatoduodenectomy; POPF post-operative pancreatic fistulae; NG no glue
INTRODUCTION
Pancreaticoduodenectomy (PD) is a commonly performed surgical procedure for various malignant and benign diseases of the pancreas and periampullary region [1]. The reported major postoperative complication rate after PD is 40% to 50% [2-5]. Poor pre-operative cardiac reserve is a predictor of those patients most susceptible to developing complication post PD [6]. A pancreatic anastomotic leak with post-operative pancreatic fistula (POPF) is the most common complication after PD [1, 7, 8] with a reported incidence of 2% to 28% [2, 9-13]. Leaks can lead to delayed gastric emptying, wound infection, pancreatitis, bleeding, peritonitis and/or sepsis [1, 7] and death. Over the past decade, peri-operative mortality in large specialised centres performing PD has improved to 0-3% [14, 15]. A review of over 500 patients undergoing PD for malignant disease at our centre found that pancreatic leaks contributed to peri-operative mortality of 2%, but did not influence long term survival [16]. However, despite improving mortality, with such high reported perioperative morbidity 30%- 50% [2, 9, 10], reducing pancreatic leak and fistula should be an important objective of every pancreatic surgeon when performing PD.
Management of the pancreatic stump after PD remains controversial [8]. Improved diagnostic aides and radiological intervention techniques have led to an increasing trend towards conservative management of POPF [7] but not without risk as conservative management of fistula has been shown to be associated with high mortality in some studies [2, 13, 15, 18]. When uncontrolled POPF occurs, completion pancreatectomy (CP) remains the gold standard for stopping these pancreatic leaks [19] but leaves patients without endogenous Insulin and Glucagon hormone production resulting in difficult to control diabetes. We recently reported that prophylactic Octreotide given post PD does not reduce the incidence of POPF [20]. Various techniques of stump management have been described with variable results [18-28]. These include drainage techniques such as placement of a stent in the pancreatic duct to support the healing anastomosis [18], placement of an external drain in the pancreaticobiliary jejunal limb [25], use of T tube [26], insertion of a transhepatic catheter [27], pancreatic drainage to the stomach [28] and separate Roux-en-Y drainage [27, 29] of the pancreas. Variations in the anastomotic techniques have been employed to mitigate POPF including, a singlelayer end-to-end intussuscepting anastomosis [30], single layer end to side anastomosis [1], multilayer anastomosis with small bowel patch [31] duct-to-mucosa technique [4, 29, 32] and invagination technique [1].
EVICEL® (Johnson and Johnson Medical Pty Ltd., Pinewood Campus, Nine Mile Ride, Wokingham, Berkshire, United Kingdom, RG40 3EW) is an adhesive fibrin glue sealant that consists mainly of human fibrinogen and thrombin, was granted marketing authorization valid throughout the EU on 6 October 2008 for use in both haemostasis and tissue sealing. Previous non-randomised and retrospective studies involving pancreatic resection with pancreatico-enteric anastomoses have suggested that the incidence of a fistula decreases after a pancreatic resection with the application of fibrin glue and collagen patch [33, 34]. A randomised study published in 2011 involving 128 consecutive patients who underwent PD and who had pancreatico-jejunostomy reinforced with or without polyglycolic acid mesh and fibrin glue sealant found no differences in the fistulae rate between the groups [35]. A prospective randomised study that applied fibrin glue to patients after a PD or a distal pancreatectomy for a wide range of pancreatic disease including inflammatory pancreatitis showed no difference in the rates or severity of pancreatic fistulae or intra-abdominal complications [36]. Recently a small study involving 57 patients where 32 patients had fibrin glue applied outside the seromuscular - pancreatic parenchymal anastomosis showed no significant differences in the rates of pancreatic fistulae, general complications or raised lipase levels among patients undergoing PD. The author attributed the presence of soft pancreas with associated pancreatic fistula and complications [10]. Similar results have been reported in another trial performed in a high volume centre with similar post-operative complications and leaks rates among 125 patients undergoing PD. [37].
The use of EVICEL® to reduce the incidence of a gastrointestinal anastomotic leak in major visceral surgery has been trialled in non-randomised trials, some with positive results [38].
However, there are no randomised trials using EVICEL® or other fibrin glue products as a film between a two layer pancreatico-jejunostomy anastomosis following PD. We therefore evaluated the effect of topical fibrin glue applied in this manner after pancreaticoduodenectomy on postoperative pancreatic fistula, overall complication rates and hospital length of stay (LOS).
METHODS
Surgical Technique and Post-Operative Management
This was a single centre audit of 100 consecutive and contemporaneous Whipple’s procedures performed by a single consultant surgeon (B Jaques) where the only variable was a thin layer of fibrin glue sealant in alternate patients from 1 to 100 placed between a 2 layer pancreatico-jejunostomy as seen in Figure 1. A standardised pancreaticoduodenectomy was performed in 98 patients who had a pylorus preserving procedure and in one glue, and one non-glue patient who had a classical Whipple’s performed. There were 5 patients who required a portal venous resection, one glue patient and 4 non-glue patients and only one of the 100 patients had down staging neo-adjuvant chemo-radiotherapy; none of these patients had a complication or pancreatic fistulae. All pancreatico-jejunostomy anastomoses were fashioned end to side in two layers. The inner layer was formed using interrupted 4.0 PDS duct-to-mucosa sutures. Then, with or without a fibrin glue sealant middle layer, the outer layer was fashioned with a running 4.0 PDS seromuscular jejunum to pancreatic parenchyma suture. Three surgical drains were placed in exactly the same manner in all patients and drain fluid from each collected daily from day 3 to day 8 when drains were routinely removed in the absence of pancreatic fistula. Pancreatic fistula was detected by analysing drain fluid effluent for amylase and defined as positive when levels were greater than 3 times normal serum level (>300U/L). All patients had a nasogastric drainage tube as well as a naso-jejunal (NJ) fine bore feeding tube paced at surgery. The tip of each NJ feeding tube was manually manipulated distal to the gastro-enterostomy and PEPTAMEN® feed (Nestlé Health Science, Suite 1.11, South Harrington Building, 182 Sefton Street, Brunswick Business Park, Liverpool, L3 4BQ) was commenced initially at 10 mLs/hour, and then gradually increased to 50 mLs/hour. Feed was started on the night of surgery and continued until oral diet was tolerated usually on the third or fourth post-operative day. In addition, all patients had peri-operative intravenous (i.v.) Pantoprazole 40 mg daily until commencing an oral diet.
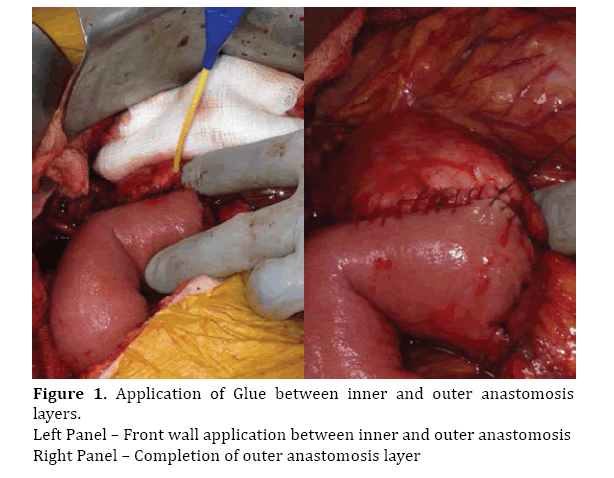
Figure 1. Application of Glue between inner and outer anastomosis layers.
Left Panel – Front wall application between inner and outer anastomosis
Right Panel – Completion of outer anastomosis layer
All patients were consented as outpatients prior to their operation. At the time of each PD, alternate patients received fibrin glue sealant (EVICEL®) with their anastomosis. Patients receiving fibrin glue sealant, had EVICEL® applied topically through a double-barrel syringe connected to a Y-shaped catheter applied circumferentially between the mucosal and sero-muscular layer in a thin layer (4-10 mL in total required). EVICEL® was not applied into the pancreatic duct.
Three large bore 19-Fr Blake surgical drains were placed in exactly the same manner in each patient. Two were positioned to sit posterior to the pancreatico-jejunal anastomosis and one placed anterior to it. Effluent from each drain was analysed biochemically for fluid amylase until removal.
Nasogastric and NJ tubes were removed once patients tolerated oral diet.
Data Collection and Outcome Measures
All data were collected prospectively. Primary endpoints were post-operative pancreatic fistulae (POPF), any complication and hospital length of stay. Post-operative complications were recorded as per the modified Clavien- Dindo classification adapted for pancreaticoduodenectomy [23]. Pancreatic fistulas were defined according to the International Study Group on Pancreatic Fistula recommendations (ISGPF) [21] as any measurable volume of fluid output from any drain on or after postoperative day 3 that had an amylase level three times greater than the serum level (>300 U/L). The presence of a peri-pancreatic fluid collection on axial imaging with clinical suspicion of a fistula was included in the analysis in patients in whom drains had been removed. Drains with fluid effluent of any volume with high amylase recordings remained in-situ until the recorded volume was zero for two consecutive days, this on one occasion required patient discharge with outpatient management of drains by a district community nurse.
Fistula Risk Score
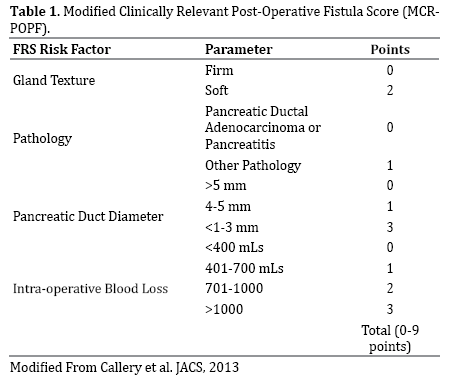
The FRS as defined by Callery et al. [24], was modified slightly for this study. The scoring for pancreas gland texture, pathology, and intraoperative blood loss was not modified, however the pancreatic duct diameter as measured at operation was measured into 3 and not 5 categories. It was felt that it was too subjective to differentiate the smaller diameter ducts which could easily dilate with passage of a measuring micrometre. Ducts were measured using a single standard 4mm cannula as a gauge and were grouped when it didn’t fit as <4 mm (3 points), it fit snuggly as 4-5mm (1 point), there was excess room once placed >5 mm (0 points). This modified FRS is defined in Table 1.
Follow-up
After initial follow-up between 4 to 6 weeks, all patients were regularly reviewed appropriately depending on their underlying pathological condition. No patients were lost to follow-up.
Statistical Analysis
All results are expressed as median and range values. Continuous variables were analysed using Mann-Whitney U test whereas categorical variables were analysed using the chi-squared and/or Fisher’s exact test. All statistical analyses were performed using SPSS software for Windows (version 21; SPSS, Inc, Chicago, IL).
RESULTS
Patients Characteristics
Patient demographics are summarised in Table 2. Results from 100 consecutive patients undergoing Whipple’s PD for malignant and benign pancreatic lesions from November 2008 to 2014 were audited. Fifty patients had EVICEL® Glue ((G) group) applied between a two layer pancreatico-jejunostomy anastomosis and 50 had standard anastomosis without a glue layer, No Glue ((NG) group). The two groups were matched with regards to age [G median = 68 years (range 44-84 years) vs. NG mediaN= 66, (range 38-82 years), P=0.19] and sex [G Male: Female 25:25 vs. NG Male: Female 26:24, P=0.84].

Post- Operative Complications
There was no mortality in either group. Post-operative complications rates are shown in Tables 3, 4. The overall complications were N=12(24%) in each group (P=0.22). Significant complication rate (Clavien Grade 3 and above) [G N=4(8%) vs. NG N=2(4%), P=0.40] was also similar between the two groups. The most common post-operative complication was post-operative pancreatic fistula [G N=7(14%) vs. NG N=11(22%), P=0.42], the majority of which in each group were biochemical pancreatic leaks which were insignificant and required no intervention (see below). Post-operative length of stay (LOS) was also similar [G median 13 days, (range 11-21 days) vs. NG median 14 days, (range 9-22 days), P=0.90].


Importantly, the peri-operative findings of soft pancreas in N=32(32%) of patients (P=0.17) or small diameter of the pancreatic duct in N=57(57%) of patients (P=0.92) and/ or preoperative biliary stent placement in N=72(72%) of patients (P=0.15) were not different between the groups and were not predictive of increase post-operative leak or complication rates on their own.
Post- Operative Pancreatic Fistula
When POPF occurred in this series, they were segregated into two broad categories, clinically significant or strictly biochemical fistulae and graded A, B or C as defined by ISPGF [21]. Clinically significant fistulae were defined as leaks whereby the volume of fistula effluent was greater than 50 mLs/24 hours and/or the patient displayed any of the following signs or symptoms of systemic upset such as pyrexia, elevated white cell count, high volume nasogastric effluent, or abdominal pain. Biochemical fistulae (Grade A) were transient and asymptomatic, characterised only by elevated drain amylase levels and had no significant clinical sequelae [21, 22]. In contrast, clinically significant POPF (Grades B and C) were more morbid and required any deviation from normal clinical management. Grade B fistulae include therapeutic medical management with antibiotics or Octreotide infusion with Total Parenteral Nutrition (TPN). Grade C fistulae are defined as requiring more invasive intervention in the form of an operative intervention under general anaesthesia, percutaneous radiological insertion of drain with return to ICU for intense management. These particularly severe fistulae can also in some cases lead to sepsis, organ failure or death [21].
In this study, the overall combined incidence of pancreatic fistula in both groups (Glue and no Glue) together was N=18(18%), of which 61% (N=11 of 18) were ISPGF Grade A biochemical leaks which required no medical or surgical treatment. Table 5 summaries all the pancreatic fistulae. Although there was a trend for less pancreatic fistulae in the patients who received EVICEL® Glue, the post-operative pancreatic fistula rate was not significantly different between the groups [G N=7(14%) vs. NG N=11(22%), P=0.42]. Using the ISPGF Grading of pancreatic fistula severity, 5 patients in the G group had Grade A fistula compared to 6 patients in the NG group, [G N=5(10%) vs. NG N=6(12%), P=0.50]. Two patients in the G group and 4 patients in the NG group required Octreotide as a continuous IV infusion at a dose of 200μg/ hour and TPN instituted to control ISPGF Grade B high volume pancreatic fistulae [G N=2(4%) vs. NG N=4(8%), P=NS]. One patient in the NG group required radiological insertion of a drain with return to ICU for an intraabdominal collection related to pancreatic fistula ISPGF Grade C [G N=0(0%) (N=0) vs. NG N=1(2%), P=NS].

When POPF was examined in the context of modified Fistula Risk Score (FRS) Table 1, [24] we found that that patients with high FRS who had glue treatment applied, experienced significantly less POPF than patients in the No-Glue group [CRF-POPF 7 points: POPF G N=4 of 13 (31%) vs. POPF NG N=9 of 18 (50%), P=0.03] (Figure 2).
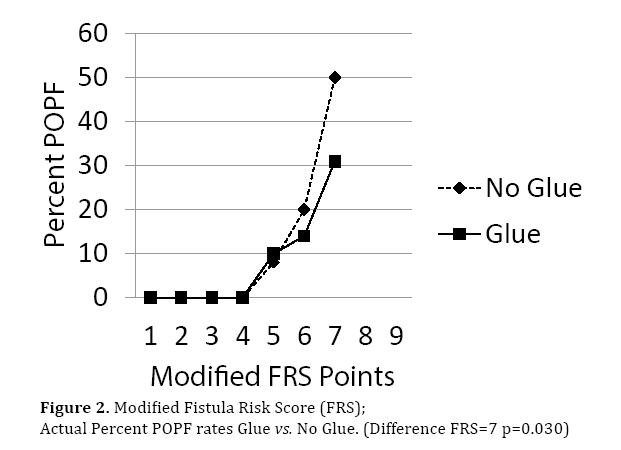
Figure 2. Modified Fistula Risk Score (FRS); Actual Percent POPF rates Glue vs. No Glue. (Difference FRS=7 p=0.030)
DISCUSSION
This single-centre audit was performed to evaluate the role of EVICEL® Glue in preventing post-operative complications after pancreaticoduodenectomy (PD). 100 consecutive patients undergoing Whipple’s procedure for malignant and benign pancreatic lesions were included. Fifty alternating patients received fibrin glue applied between anastomotic layers as a thin film during pancreaticoduodenectomy and were compared to 50 contemporaneous patients who did not have glue application. The results of this study are stronger than previous similar publications in that all the procedures were performed in a high volume centre by a single surgeon using the same technique for anastomosis, drain placement and fistula detection. The two groups were matched with regards to age, sex and pancreatic consistency, and the only difference between the groups was a layer of fibrin glue between the anastomotic layers in half of the patients. No significant difference was found between the two groups in terms of overall post-operative pancreatic leak rates [G N=7(14%) vs. NG N=11(22%), P=0.42] or significant complications rates [G N=2(4%) vs. NG N=4(8%), P=0.40].
Many studies attribute post-operative pancreatic fistula (POPF) following PD with soft texture of the pancreas [10]. However, in our series the soft consistency of pancreas was present in 15%-17% of the patients and on single variate analysis was not associated with increased POPF. There was a trend for less overall POPF when EVICEL® glue was applied. When the risk of fistula was defined by FRS, in patients most at risk of developing fistula with the highest FRS, there were significantly more POPF in the noglue cohort. We adapted the FRS slightly using a simple, reliable and accurate method of measuring pancreatic duct diameter. Although this modification has not been validated in large studies, we feel that grouping the small diameter duct values into a single value is more accurate and less subjective then differentiating between 1, 2 and 3 mm duct diameters. The score of 3 for >1-3mm ducts was derived from the sum and average of the combined points as defined by Callery et.al. [24]. We found that patients with low modified FRS did not experience POPF, however as expected, with higher point scoring POPF increased. The highest MCR-POPF score in this study was 7 points which had similar number of patients in each group. The fistula rate however was 19% higher in the NG cohort indicating that there is a role for application of a fibrin glue layer in patients undergoing PD with a likely diagnosis that does not include pancreatic ductal adenocarcinoma or pancreatitis, coupled with a soft pancreas, small diameter duct and/or high intra-operative blood loss.
The weakness of this study was the method of randomisation and small sample size. As the two groups were well matched with regards to the patient age, sex, consistency of pancreas texture, presence of biliary stent at operation, and small pancreatic duct size the audit has found remarkably similar cohorts for comparison. This study does appear underpowered for showing statistical differences between the groups in the overall complication and pancreatic fistula rate which we feel is attributable to the low significant complication and serious pancreatic fistulae rates in both cohorts. To reach statistical significance for overall POPF and complication rates, future studies would need to draw data from several individuals in a large unit or span several centres and would need to be tightly controlled for standardisation of operation, drain placement and detection of fistula in the post-operative period as was controlled in this study. When the risk of POPF was stratified using a FRS, the study was sufficiently powered showing advantage with glue in those with high FRS.
The technique of fibrin glue application between the layers of PD anastomoses was unique to this study and performed to augment the seal of the outer anastomoses by forming a strong fibrin bond between the pancreas and jejunum. Fibrin glue was not associated with any adverse events in the 50 patients who had it applied.
As most patients had uneventful operations and those that had POPF mostly had clinically insignificant leaks, it is not surprising that the hospital length of stay was almost identical in both groups and it is unlikely that a larger study size would find differences in that outcome in a single centre trial.
CONCLUSION
The application of glue sealant was safe with no adverse effects. We recommend that fibrin glue should be considered in those where a high FRS is predicted as glue significantly reduced the POPF rate in patients most at risk for developing CR-POPF.
Conflict of Interest
Authors declare no conflict of interests for this article.
References
- Yeo CJ, Cameron JL, Lillemoe KD, Sauter PK, Coleman J, Sohn TA, Campbell KA, Choti MA. Does prophylactic Octreotide decrease the rates of pancreatic fistula and other complications after pancreaticoduodenectomy? Results of a prospective randomized placebo-controlled trial. Ann Surg 2000; 232:419-429. [PMID: 10973392]
- Yeo CJ, Cameron JL, Sohn TA, Lillemoe KD, Pitt HA, Talamini MA, Hruban RH, Ord SE, et al. Six hundred fifty consecutive Pancreaticoduodenectomies in the 1990s: pathology, complications, outcomes. Ann Surg 1997; 226:248-260. [PMID: 9339931]
- Strasberg SM, Drebin JA, Soper NJ. Evolution and current status of the Whipple procedure: an update for gastroenterologists. Gastroenterology 1997; 113:983-994. [PMID: 9287993]
- Fernandez-del Castillo C, Rattner DW, Warshaw AL. Standards for pancreatic resection in the 1990s. Arch Surg 1995; 130:295-300. [PMID: 7887797]
- Yeo CJ. Management of complications following pancreaticoduodenectomy. SurgClin North Am 1995; 75:913-924. [PMID: 7660254]
- Ausania F, Snowden CP, Prentis JM, Holmes LR, Jaques BC, White SA, French JJ, Manas DM. Effects of low cardiopulmonary reserve on pancreatic leak following pancreaticoduodenectomy. British Journal of Surgery 2012; 99:1290-4. [PMID: 22828960]
- Haddad LBP, Scatton O, Randone B, Andraus W, Massault PP, Dousset B, Soubrane O. Pancreatic fistula after pancreaticoduodenectomy: the conservative treatment of choice. HPB 2009; 11:203-209. [PMID: 19590648]
- Balcom JH IV, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg 2001; 136:391-398. [PMID: 11296108]
- Schmidt CM, Powell ES, Yiannoutsos CT, Howard TJ, Wiebke EA, Wiesenauer CA, Baumgardner JA, Cummings OW. Pancreaticoduodenectomy: a 20-year experience in 516 patients. Arch Surg 2004; 139:718-727. [PMID: 15249403]
- Martin I, Au K. Does fibrin glue sealant decrease the rate of anastomotic leak after a pancreaticoduodenectomy? Results of a prospectiverandomized trial. HPB 2013; 15:561-166. [PMID: 23458447]
- Lin JW, Cameron JL, Yeo CJ, Riall TS, Lillemoe KD. Risk factors and outcomes in postpancreaticoduodenectomy pancreaticocutaneous fistula. J Gastrointest Surg 2004; 8:951-959. [PMID: 15585382]
- Sarr MG; Pancreatic Surgery Group. The potent somatostatin analogue vapreotide does not decrease pancreas-specific complications after elective pancreatectomy: a prospective, multicenter, double-blinded, randomized, placebo controlled trial. J Am Coll Surg 2003; 196:556-565. [PMID: 12691930]
- Buchler MW, Friess H, Wagner M, Kulli C, Wagener V, Z'Graggen K. Pancreatic fistula after pancreatic head resection. Br J Surg 2000; 87:883-889. [PMID: 10931023]
- Allema JH, Reinders ME, van Gulik TM, Koelemay MJ, Van Leeuwen DJ, de Wilt LT, Gouma DJ, Obertop H. Prognostic factors for survival after Pancreaticoduodenectomy for patients with carcinoma of the pancreatic head region. Cancer 1995; 75:2069-2076. [PMID: 7697596]
- Miedema BW, Sarr MG, van Heerden JA, Nagorney DM, McIlrath DC, Ilstrup D. Complications following pancreaticoduodenectomy: current management. Arch Surg 1992; 127:945-949. [PMID: 1353671]
- Sewpaul A, Farooque Y, Robinson S, Sen G, French JJ, White S, Manas D, Charnley R, Jaques B. The Effect of a Pancreatic Anastomotic Leak on Survival Following Pancreatectoduodenectomy for Ampullary, Distal Cholangiocarcinoma and Pancreatic Ductal Adenocarcinoma. JOP 2015; 16:235-44.
- Bottger TC, Junginger T. Factors influencing morbidity and mortality after pancreaticoduodenectomy: critical analysis of 221 resections. World J Surg 1999; 23:164-171. [PMID: 9880426]
- Hamanaka Y, Suzuki T. Total pancreatic duct drainage for leakproofpancreaticojejunostomy. Surgery 1994; 115:22-26. [PMID: 8284756]
- Gueroult S, Parc Y, Duran F, Paye F, Parc R. Completion pancreatectomy for postoperative peritonitis after pancreaticoduodenectomy: early and late outcome. Arch Surg 2004; 139:16-19. [PMID: 14718268]
- Rohatgi S, Rehman S, French J, Manas D, Sen G, White S, Jaques B. Role of prophylactic octreotide in pancreaticoduodenectomy patients: single centre comparative study in 456 whipple’s patients. (Accepted for Publication) JOP; 2016; 17: 1.
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, Neoptolemos J, Sarr M, Traverso W, Buchler M. Postoperative pancreatic fistula: An international study group (ISGPF) definition. Surgery 2005; 138 (1): 8-13. [PMID: 16003309]
- Pratt WB, Maithel SK, Vanounou T, Huang ZS, Callery MP, Vollmer CM, Jr. Clinical and economic validation of the International Study Group of Pancreatic Fistula (ISGPF) classification scheme. Ann Surg 2007; 245:443-451. [PMID: 17435552]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205-13. [PMID: 15273542]
- Callery MP, Pratt WB, Kent TS, Chaikof EL, Vollmer CM, Jr. A prospectively validated clinical risk score accurately predicts pancreatic fistula after pancreatectomy. 2013; J Am Coll Surg 216:1-14. [PMID: 23122535]
- Keck H, Steffen R, Neuhaus P. Protection of pancreatic and biliary anastomosis after partial duodenopancreatectomy by external drainage. Surg Gynecol Obstet 1992; 174:329-331. [PMID: 1348151]
- Marcus ST, Cohen H, Ranson JHC. Optimal management of the pancreatic remnant after pancreaticoduodenectomy. Ann Surg 1995; 221:635-638. [PMID: 7794068]
- Cameron JL. Atlas of Surgery, Vol 1. Philadelphia: Decker/Mosby- Year Book 1990; 402-403.
- Mason GR, Freeark RJ. Current experience with pancreatogastrostomy. Am J Surg 1995; 169:217- 219. [PMID: 7840383]
- Kingsnorth AN. Duct to mucosa isolated Roux loop pancreaticojejunostomy as an improved anastomosis after resection of the pancreas. Surg Gynecol Obstet 1989; 169:451- 453. [PMID: 2814757]
- Sing RF, Reilly PM, Schwab CW. The single-layered, parachuted intussuscepted pancreaticojejunostomy. Am Surg 1995; 61: 322-323. [PMID: 7893096]
- Hiraoka T, Kanemitsu K, Tsuji T, Saitoh N, Takamori H, Akamine T, Miyauchi Y. A method for safe pancreaticojejunostomy. Am J Surg 1993; 165: 270-272. [PMID: 8427410]
- Matsumoto Y, Fujii H, Miura K, Inoue S, Sekikawa T, Aoyama H, Ohnishi N, Sakai K, et al. Successful pancreaticojejunal anastomosis for pancreaticoduodenectomy. Surg Gynecol Obstet 1992; 175:555-562. [PMID: 1360173]
- Chirletti P, Caronna R, Fanello G, Schiratti M, Stagnitti F, Peparini N, Benedetti M, Martino G. Pancreaticojejunostomy with application of fibrinogen/thrombincoated collagen patch (TachoSil) in Roux-en-Y reconstruction after pancreaticoduodenectomy. J Gastrointest Surg 2009; 13:1396-1398. [PMID: 19381733]
- Mita K, Ito H, Fukumoto M, Murabayashi R, Koizumi K, Hayashi T, Kikuchi H Pancreaticojejunostomy using a fibrin adhesive sealant (Tacho Comb (registered trademark)) for the prevention of pancreatic fistula after pancreaticoduodenectomy. Hepatogastroenterology 2011; 58:187-191.
- Satoi S, Toyokawa H, Yanagimoto H, Yamamoto T, Hirooka S, Yui R, Yamaki S, Matsui Y, et al. Reinforcement of pancreticojejunostomy using polyglycolic acid mesh and fibrin glue sealant. Pancreas 2011; 40:16-20. [PMID: 20966808]
- D’Andrea AA, Costantino V, Sperti C, Pedrazzoli S. Human fibrin sealant in pancreatic surgery: it is useful in preventing fistulas? A prospective randomized study. Ital J Gastroenterol 1994; 26:283-6. [PMID: 7949264]
- Lillemoe KD, Cameron JL, Kim MP, Campbell KA, Sauter PK, Coleman JA, Yeo MD. Does fibrin glue sealant decrease the rate of pancreatic fistula after pancreaticoduodenectomy? Results of a prospective randomized trial. J Gastrointest Surg 2004; 8:766-72; discussion 772-4. [PMID: 15531229]
- OrciLA,Oldani G, Berney T, Andres A, Mentha G, Morel P, Toso C. Systematic review and meta-analysis of fibrin sealants for patients undergoing pancreatic resections. HPB (Oxford) 2014; 16:3-11. [PMID: 23461684]

