Keywords
Choledocholithiasis; Cholelithiasis; Common Bile Duct; Gallbladder; Gallstones
INTRODUCTION
Historically, no cause was identified in 10-30% [1, 2] of cases of acute pancreatitis and these patients were often labelled as suffering from idiopathic acute pancreatitis. The advent of endoscopic retrograde cholangiopancreatography (ERCP) led to a cause being identified in 30-60% of such cases, with pathologies including biliary calculi, chronic pancreatitis, pancreatic tumours and sphincter of Oddi dysfunction [3]. More recently, the development of endoscopic ultrasound (EUS) has provided a new means of examining the bile duct. The role of EUS in searching for common duct stones was first reported by Edmundowicz et al. in 1992 [4]. A review by Rösch et al. estimated the prevalence of stones in an analysis of 15 series to be 39.9%, with an overall sensitivity of 93.1% and a specificity of 89.0% [5].
However, there are a number of difficulties in comparing series due to widely differing: criteria for patient selection, investigation algorithms, and examination techniques. There is also the constantly evolving EUS imaging technology. In addition, EUS cannot be widely accepted as a primary investigation method, at least at present, due to its limited availability outside of the teaching hospital setting as it requires a skilled endoscopist and there is a steep learning curve to evaluating the images obtained.
The aim of this study was to investigate the role of EUS where other investigative techniques including: trans-abdominal ultrasound scan (US); computed tomography (CT); ERCP; and magnetic resonance cholangiopancreatography (MRCP), had failed to identify the cause of biochemically proven acute pancreatitis.
PATIENTS AND METHODS
The computerised radiology database at University Hospital Wales was utilised to identify all patients undergoing EUS during the period January 2000 to December 2004. Patients had the procedure performed and reported by a single radiologist. Only those undergoing EUS in the setting of acute pancreatitis were included. The diagnosis of acute pancreatitis was based on the clinical history and clinical examination and confirmed by the detection of a serum amylase of greater than 400 IU/L [6]. Patient notes were retrieved from the medical records department and data collected included the demographic data and the reports of pre-EUS imaging. The reports from the EUS examination were then compared to the other modalities. In cases in which surgery was subsequently performed, the EUS findings were compared to the operative findings. Clinical follow-up was until December 2007.
Following conscious sedation, an Olympus radial echoendoscope (UM-20 or UM-2000, KeyMed, Southend-on-Sea, Essex, United Kingdom) was passed to the second part of the duodenum. At the level of the papilla, in the long position, gentle withdrawal of the endoscope was commenced. Inflation of a water filled balloon around the ultrasound transducer, and aspiration of luminal gas enabled ultrasound imaging of the gallbladder, biliary tract, and pancreatic head.
STATISTICS
Descriptive statistics only were computed: mean, median, standard deviation, range, and frequencies.
ETHICS
Approval was obtained from the Research and Development Department of the Hospital prior to commencing the work. Informed consent was obtained from all patients prior to performance of endoscopic ultrasound and all aspects of the study were conducted in accordance with the Declaration of Helsinki.
RESULTS
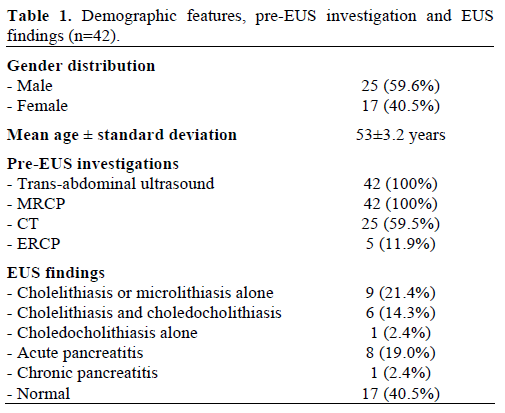
During the 5-year period covered by the study, forty two patients (25 male and 17 female; mean age 53±3.2 years) with negative prior imaging underwent EUS to determine the aetiology in cases of idiopathic acute pancreatitis (Table 1). The study cohort requiring an EUS represented 6.7% of the 630 patients experiencing 672 episodes of acute pancreatitis during the interval covered by the study. Pre-EUS imaging included US and MRCP which had been performed in every case, with in addition CT (n=25; 59.5%) or ERCP (n=5; 11.9%). All patients undergoing EUS examination had suffered an episode of mild pancreatitis and none were persistently jaundiced at the time of EUS. EUS was normal in 17 patients (40.5%) and in none of these patients has cholelithiasis/choledocholithiasis since been confirmed by any diagnostic means.
Pancreaticobiliary abnormalities were identified in 25 of 42 patients (59.5%). Cholelithiasis or microlithiasis was the commonest finding being identified in 15 patients (35.7%) (Figure 1). Choledocholithiasis was noted in 7 patients (16.7%): 6 of which also had gallstones, while one patient had calculi identified within the common bile duct but not the gallbladder (Figure 2). Therefore overall, 16 patients (38.1%) had EUS evidence of stone disease.
Figure 1. EUS confirming the presence of microlithiasis (arrowed)
within the gallbladder.
Figure 2. EUS demonstrating a small stone (arrowed) within the
common bile duct that was not observed on MRCP.
Signs of recent acute pancreatitis without an underlying cause were observed in 8 patients (19.0%). These consisted of pancreatic parenchymal oedema and small peri-pancreatic fluid collections and were identified in patients who had undergone US and MRCP and not CT. These observations did not contribute to identifying an aetiology for the pancreatitis but did confirm the insult had occurred.
The final patient, who suffered from recurrent attacks of acute pancreatitis, had changes compatible with chronic pancreatitis diagnosed on EUS.
All patients with common bile duct stones underwent ERCP and sphincterotomy, and stones were universally confirmed. The patient with gallbladder calculi alone was listed for cholecystectomy but developed jaundice whilst awaiting cholecystectomy. The individual underwent ERCP which demonstrated microlithiasis within the common bile duct.
No patients with a normal EUS have subsequently been re-investigated and diagnosed with cholelithiasis during the follow-up period which was a median of 73.7 months (range: 58.8-99.1 months).
DISCUSSSION
The primary finding of the study was the identification of stone pathology in 16 of 42 (38.1%) patients in whom other imaging modalities had failed to identify lithiasis. The finding of early chronic pancreatitis in a further patient where this had not been seen on CT or cholangiography meant that EUS identified a cause of pancreatitis in 17 of 42 (40.5%) of cases. Therefore, with the combination of investigations used, the idiopathic pancreatitis rate in the entire series of 630 patients experiencing acute pancreatitis during the interval covered by the study was 4.0% (25 patients). As the minimum duration of follow-up was nearly 5 years and no further episodes of pancreatitis were recorded, it is likely that EUS was accurate in identifying all of those with pancreatobiliary pathology as aetiology for their pancreatitis.
The identification of cholelithiasis/choledocholithiasis in patients with acute pancreatitis is of vital importance given the persisting high mortality rates of 19-25% seen in patients developing severe acute pancreatitis with necrosis as a result of gallstone disease [7, 8]. For most patients with gallstone pancreatitis, a transabdominal ultrasound will identify cholelithiasis and may demonstrate a dilated biliary tree. Furthermore, in half of the cases with choledocholithiasis a stone may be identified using ultrasound. If stones are not seen in either the gallbladder or bile duct using ultrasound then CT cholangiography, MRCP or ERCP may be utilised with varying degrees of success. Another option is to consider EUS. This may be used routinely or selectively when other non-invasive modalities have failed to identify an aetiology for the acute pancreatitis. There is currently good evidence to suggest that EUS is superior to CT [9, 10, 11], MRCP [11, 12, 13], and ERCP [14, 15] in detecting gallstone disease in the setting of obstructive jaundice. EUS has a reported sensitivity of up to 100%, specificity as high as 95.4% and accuracy of 96.9% together with a negative predictive value as high as 100% for the detection of common duct stones which are the cause of acute biliary pancreatitis. EUS appears to be particular benefit over other methods in relation to the detection of stones smaller than 5 mm in diameter, those that typically cause acute pancreatitis.
There are fewer studies that have specifically looked at the role of EUS in establishing the cause of acute pancreatitis either in the acute or post-acute phase [16, 17, 18, 19, 20]. The sensitivity in these studies has been reported at 91-100%; with a specificity of 100% and an accuracy of 97-100%. It is difficult to be certain of the sensitivity/specificity in this series, as many of the patients undergoing EUS had already had a negative ERCP, the investigation usually regarded as a “gold standard”.
Given the superiority of EUS over other imaging modalities, it may be argued that EUS be used in the investigation of all cases of acute pancreatitis in which no calculi are observed in either the gallbladder or common bile duct on trans-abdominal US. However, given the limited availability of EUS and pressures on skilled operators to perform non-biliary investigations, we would suggest that all patients with acute pancreatitis undergo a trans-abdominal US and also have routine biochemical investigations to look for hypercalcaemia and hyperlipidaemia. A careful drug history is important in particular in relation to “statins” as these drugs are now widely prescribed as lipid lowering agents, and are associated with acute pancreatitis [21]. We then perform an MRCP as our next investigation of choice, with EUS limited to those in which no cause for acute pancreatitis has been identified. In the future, as EUS proliferates, it may then become the investigation of choice.
One figure that does vary between series is prevalence of calculi detected by EUS performed for evaluation of presumed common bile duct calculi. In our series, calculi not identified by other modalities were detected in 38% of cases, which is comparable to the overall figure for presence of stones of 30.9% reported in the Rösch et al. review [5]. However, in this review figures varied from 19% to 68% which probably reflects changes in imaging technologies in the 8-year period covered by the studies described in the review but may also be related to operator experience or a genuine variation in prevalence in lithiasis/microlithiasis in the populations studied; these questions not being addressed in the studies.
One limitation of studies assessing imaging modalities is the constant evolution in the quality of the images obtained. Since the end of the recruitment period there have been several significant developments in endoscope technology and thus the specificity and sensitivity of the investigation is likely to have improved. If a primary EUS service was being assessed this would be a very significant issue; however, in a situation in which EUS is a second line investigation, it must be recalled that MRI has also improved in this time interval thus emphasising the importance of regular auditing of imaging modalities to ensure the best possible service is being provided.
CONCLUSIONS
EUS provided additional diagnostic information in 17 of the 42 (40.5%) patients. Moreover, exclusion of gallstones/microlithiasis is also important as it facilitates a search for other causes of pancreatitis. In conclusion, most cases of cholelithiasis can be diagnosed with standard imaging modalities but when these fail to identify a cause, EUS has an important role to play.
Conflict of interest
The authors have no potential conflicts of interest
References
- Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med 1994; 330:1198-210. [PMID 7811319]
- Ballinger AB, Barnes E, Alstead EM, Fairclough PD. Is intervention necessary after a first episode of acute idiopathic pancreatitis? Gut 1996; 38:293-5. [PMID 8801214]
- Katon RM, Bilbao MK, Eidemiller LR, Benson JA Jr. Endoscopic retrograde cholangiopancreatography in the diagnosis of non-alcoholic pancreatitis. Surg Gynecol Obstet 1978 147: 333-338. [PMID 684583]
- Edmundowicz SA, Aliperti G, Middleton WD. Preliminary experience using endoscopic ultrasonography in the diagnosis of choledocholithiasis. Endoscopy 1992; 24:774-8. [PMID 1468395]
- Rösch T, Mayr P, Kassem MA. Endoscopic ultrasonography in acute biliary pancreatitis. J Gastrointest Surg 2001; 5:223-8. [PMID 11419445]
- UK Working Party on Acute Pancreatitis UK guidelines for the management of acute pancreatitis. Gut 2005; 54 (Suppl 3):1-9. [PMID 15831893]
- Dervenis C, Johnson CD, Bassi C, Bradley E, Imrie CW, McMahon MJ, Modlin I. Diagnosis, objective assessment of severity, and management of acute pancreatitis. Santorini consensus conference. Int J Pancreatol 1999; 25:195-210. [PMID 10453421]
- Gullo L, Migliori M, Oláh A, Farkas G, Levy P, Arvanitakis C, et al. Acute pancreatitis in five European countries: etiology and mortality. Pancreas 2002; 24:223-7. [PMID 11893928]
- Amouyal P, Amouyal G, Lévy P, Tuzet S, Palazzo L, Vilgrain V, et al. Diagnosis of choledocholithiasis by endoscopic ultrasonography. Gastroenterology 1994; 106:1062-7. [PMID 8143973]
- Polkowski M, Palucki J, Regula J, Tilszer A, Butruk E. Helical computed tomographic cholangiography versus endosonography for suspected bile duct stones: a prospective blinded study in nonjaundiced patients. Gut 1999; 45:744-9. [PMID 10517914]
- Kondo S, Isayama H, Akahane M, Toda N, Sasahira N, Nakai Y, et al. Detection of common bile duct stones: comparison between endoscopic ultrasonography, magnetic resonance cholangiography, and helical-computed-tomographic cholangiography. Eur J Radiol 2005; 54:271-5. [PMID 15837409]
- de Lédinghen V, Lecesne R, Raymond JM, Gense V, Amouretti M, Drouillard J, et al. Diagnosis of choledocholithiasis: EUS or magnetic resonance cholangiography? A prospective controlled study. Gastrointest Endosc 1999; 49:26-31. [PMID 9869719]
- Zidi SH, Prat F, Le Guen O, Rondeau Y, Rocher L, Fritsch J, et al. Use of magnetic resonance cholangiography in the diagnosis of choledocholithiasis: prospective comparison with a reference imaging method. Gut 1999; 44:118-22. [PMID 9862837]
- Prat F, Amouyal G, Amouyal P, Pelletier G, Fritsch J, Choury AD, et al. Prospective controlled study of endoscopic ultrasonography and endoscopic retrograde cholangiography in patients with suspected common-bileduct lithiasis. Lancet 1996; 347:75-9. [PMID 8538344]
- Palazzo L, Girollet PP, Salmeron M, Silvain C, Roseau G, Canard JM, et al. Value of endoscopic ultrasonography in the diagnosis of common bile duct stones: comparison with surgical exploration and ERCP. Gastrointest Endosc 1995; 42:225-31. [PMID 7498687]
- Sugiyama M, Atomi Y. Acute biliary pancreatitis: the roles of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography. Surgery 1998; 124: 14-21. [PMID 9663246]
- Chak A, Hawes RH, Cooper GS, Hoffman B, Catalano MF, Wong RC, et al. Prospective assessment of the utility of EUS in the evaluation of gallstone pancreatitis. Gastrointest Endosc 1999; 49: 599-604. [PMID 10228258]
- Frossard JL, Sosa-Valencia L, Amouyal G, Marty O, Hadengue A, Amouyal P. Usefulness of endoscopic ultrasonography in patients with "idiopathic" acute pancreatitis. Am J Med 2000; 109:196-200. [PMID 10974181]
- Tandon M, Topazian M. Endoscopic ultrasound in idiopathic acute pancreatitis. Am J Gastroenterol 2001; 96:705-9. [PMID 11280538]
- Liu CL, Lo CM, Chan JK, Poon RT, Lam CM, Fan ST, Wong J. Detection of choledocholithiasis by EUS in acute pancreatitis: a prospective evaluation in 100 consecutive patients. Gastrointest Endosc 2001; 54:325-30. [PMID 11522972]
- Johnson JL, Loomis IB. A case of simvastatin-associated pancreatitis and review of statin-associated pancreatitis. Pharmacotherapy 2006; 26:414-22. [PMID 16503723]



