Keywords
Cholangiopancreatography, Magnetic Resonance; Common bile duct; Gallstones; Jaundice; Pancreatitis
Abbreviations
CBD common bile duct; CT computed tomography; MRI magnetic resonance imaging; US ultrasound
INTRODUCTION
Acute pancreatitis is an increasingly common and expensive problem. Over $2.2 billion per year is spent due to all causes of acute pancreatitis with inpatient admissions exceeding 300,000 and about 20,000 deaths yearly [1-4]. Although there are a great many uncommon and rare causes of pancreatitis [4-6], gallstones are the most common cause [4, 7], accounting for 30-50% cases worldwide.
Gallstone pancreatitis occurs as a result of stones in the common bile duct (CBD). Such stones may result in obstruction of the common channel within or just proximal to the papilla, resulting in outflow obstruction of pancreatic secretions. Although this can occur in the absence of infection, a colonized pancreaticobiliary tree that becomes obstructed by these stones may also produce a cholangitis involving the pancreas and leading to second mechanism of gallstone pancreatitis [8, 9]. In either case, the CBD is typically dilated.
Indeed, dilatation of the CBD is one of the most powerful independent predictors of choledocholithiasis [10, 11]. Because of the importance of ductal dilatation in the diagnosis of choledocholithiasis, and our anecdotal observation that imaging modalities are not always concordant for CBD dilatation, and the observed trends in the use of abdominal imaging, in particular increasing reliance on computed tomography (CT) [12, 13], we sought to compare the three most common extracorporeal imaging modalities regarding their measurement of the diameter of CBD, taking advantage of a very large singleinstitution database.
METHODS
Study Population and Data Collection
Approval from the Institutional Review Board of Saint Agnes Hospital was obtained and a cohort of patients diagnosed with gallstone pancreatitis was identified by retrospective review of a database of patients who underwent cholecystectomy from 2000 to 2013. Patients with inadequate data for analysis were excluded from the study. Patients were assigned to groups depending on whether they underwent ultrasound (US) alone, CT alone, magnetic resonance imaging (MRI) alone, both US and CT, both US and MRI, or both MRI and CT.
The diagnosis of gallstone pancreatitis was determined from the patient charts using history, physical examination findings, laboratory studies, and imaging reports, including abdominal US, CT, and MRI. CBD diameter was measured per protocol at the point of maximum diameter. Preoperative imaging studies were included if performed prior to cholecystectomy within 30 days, but typically within a few hours of each other in the emergency department.
Statistical Analysis
Statistical analyses were performed with SPSS (IBM Corp, Chicago). A paired-samples T-test was used to compare measurements of CBD diameter by US, CT, and MRI. A P-value <0.05 was regarded as significant.
RESULTS
Among 6876 patients undergoing cholecystectomy between 2000 and 2013 (Figure 1), a total of 738 (11%) patients were diagnosed with acute gallstone pancreatitis. The median age of this cohort was 59 years (range 12-99) with a majority being female (n=456, 62%) and Caucasian (n=442, 60%). Comorbidities were common among the study cohort, with 104 (53%) patients having an ASA class 3 or 4 (Table 1).

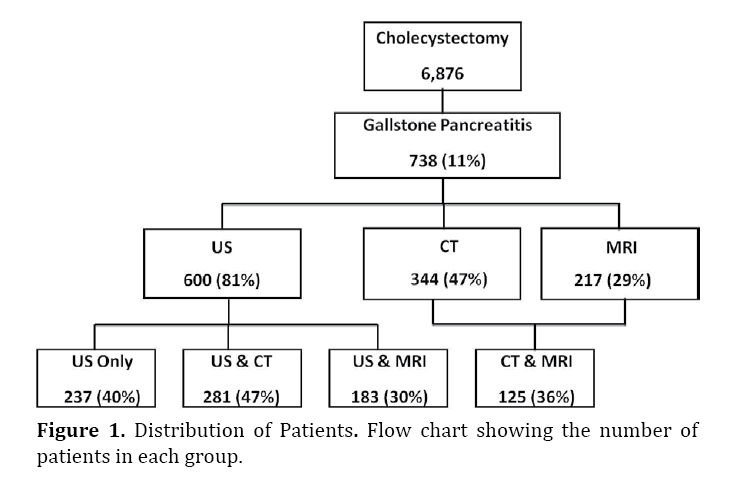
Figure 1. Distribution of Patients. Flow chart showing the number of patients in each group.
A total of 600 (81%) patients had a preoperative US documented in the medical record. The diagnosis of choledocholithiasis correlated as expected with a larger CBD diameter. Nearly half of patients, 344 (47%), underwent a CT scan, and a third (217; 30%) underwent an MRI. Of the 600 who underwent an US, 237 (40%) had a US only, 281 (47%) also underwent CT and 183 (30%) also underwent MRI (Figure 1). Only 26 of the 281 (9%) of those having CT and US had CBD measurements from both modalities; for the US vs. MRI group, 66 of 183 (36%) of reports provided the CBD diameter; and for the group CT vs. MRI, 18 of 125 (14%) had available CBD measurements (Table 2). Over the 14-year study period, the percent of patients undergoing imaging per year tended to decrease for US, but to increase for CT and MRI (Figure 2).

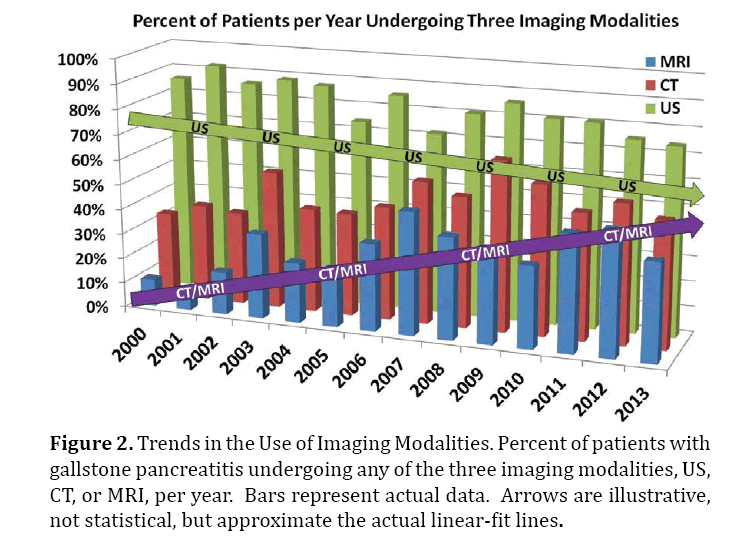
Figure 2. Trends in the Use of Imaging Modalities. Percent of patients with gallstone pancreatitis undergoing any of the three imaging modalities, US, CT, or MRI, per year. Bars represent actual data. Arrows are illustrative, not statistical, but approximate the actual linear-fit lines.
As tabulated in Table 2, the diameter of the CBD was significantly greater by CT compared to US, in patients imaged with both modalities: 11.2 mm on CT versus 8.7 mm on US (P=0.022); Figure 3 provides an illustration of this phenomenon in two cases. To exclude the possibility of a passed stone artificially causing these findings in cases where the CT was done first, we isolated only those cases in which the US was done first, followed by the CT (70% of cases). In this subgroup, the diameter of the CBD was still greater by CT compared to US, in patients imaged with both modalities: 11.9 mm on CT versus 9.7 mm on US, but did not reach the 0.05 cutoff for significance due to smaller numbers (P=0.093). The CT-measured CBD diameter was again greater than the MRI-measured diameter (13.9 vs. 10.5, respectively) although this difference was just marginally significant (P=0.059). The CBD diameter was found to be very similar when measured by MRI and US, with a mean of 7.0 mm and 7.1 mm, respectively (P=0.859).
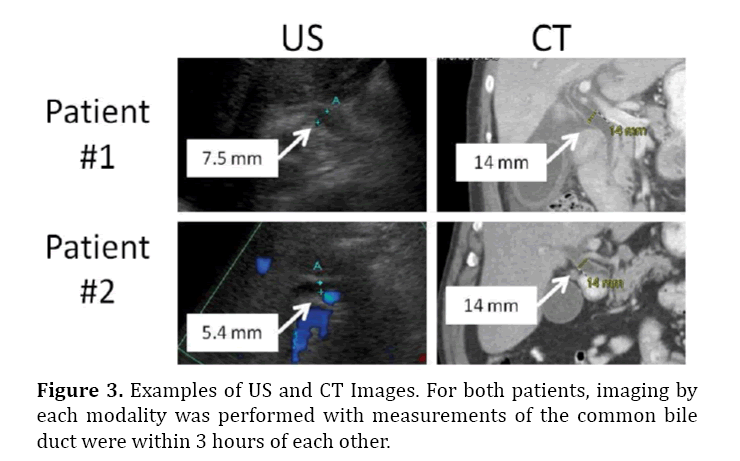
Figure 3. Examples of US and CT Images. For both patients, imaging by each modality was performed with measurements of the common bile duct were within 3 hours of each other.
The standard laboratory values alkaline phosphatase and bilirubin for patients undergoing CT (157 U/L and 1.5 mg/dL, respectively), and for those undergoing US (152 U/L and 1.3 mg/dL, respectively), were clinically similar, as expected, given the overlap in these populations.
There were insufficient data available from imaging reports to examine other relevant differences, such as gallstones, gallbladder wall thickening, and pericholecystitic fluid. For instance, of 44 patients with pericholecystic fluid on US, only 10 (23%) also had documented pericholecystic fluid reported on CT.
Likewise, 28% of patients had pericholecystic fluid on US and on MRI. Of the 32 patients who had a preoperative CT and MRI, 9 (2.1%) had pericholecystic fluid on both imaging modalities.
DISCUSSION
Although the most common clinical manifestation of gallstones is biliary colic and acute cholecystitis, as many as 8% of patients with gallstones develop gallstone pancreatitis [9, 14-16]. While gallstone pancreatitis can be mild and self-limited, up to 20% of patients develop severe acute pancreatitis with high, double-digit mortality rates [17, 18]. The definitive treatment is cholecystectomy, which in mild cases is done during the same admission to prevent future recurrence [9, 19, 20], generally after endoscopic stone extraction.
One of the cornerstones of initial management, however, is diagnosing and removing the inciting factor: the choledocholithiasis, which is generally detected using a combination of elevated lipase, alkaline phosphatase, and bilirubin, and imaging findings of a dilated bile duct containing stones. Dilatation of the CBD is one of the most reliable signs of choledocholithiasis [10, 11].
CBD dilatation has traditionally been measured using US. However, the use of CT for abdominal imaging is increasing several fold over recent years, while that of US is stable or, in some groups, decreasing [12, 13]. Using the National Hospital Ambulatory Medical Care Survey from 1996 to 2007, Kocher et al. [13] found a 330% increase in the use of CT. The fact that our upward trend (Figure 2) is less steep is likely due to an expected plateauing of the trend in more recent years than those reported by Kocher et al. The increase use of CT, which in many centers is augmenting if not supplanting US, highlights the importance of our findings.
The upper limit of normal for the diameter of the CBD is controversial [21]. A common guideline for adult patients is one millimeter per decade of life, although some recent studies have shown that the commonly observed age-related normal increase in CBD diameter is smaller: approximately 0.2 mm per decade of life [22, 23]. Following cholecystectomy, however, CBD diameter may be 10 mm without obstruction. Regardless of the normal cutoff, the same patient repeatedly imaged within a few hours (such as those patients shown in Figure 2), would be expected to have consistent findings. Yet, we have anecdotally observed that this was sometimes not the case. Therefore we designed this simple study to compare the three most common imaging modalities, US, CT, and MRI, as they were interpreted in practice, within each patient experience.
Interestingly, our suspicion was justified in that CT measurements of the CBD were significantly greater than those obtained by US (Table 2), and were also greater, though only marginally significant, than MRI measurements, whereas MRI and US measurements were very similar. To be sure that we were not simply witnessing an artificial effect whereby patients get the increasingly common CT, then pass a stone, and then get an US, we isolated cases where the US was done first, followed by the CT, and still the CT-measured diameter was larger within individual patients. This suggests that the passage of stones does not explain our findings.
This discrepancy in diameter of CBD may be due to various factors. First, it could be due to measuring the CBD in different locations along the duct, depending on the imaging modality. In general, the practice in our institution is to measure the CBD at the point of maximal diameter for all three modalities. A second possibility is that contrast agents used at the time if CT have a choleretic effect that temporarily increases bile secretion. This effect certainly used to be significant, and increases of up to 4 mm have been observed after the administration of hepatotropic contrast agents [24]. However, this is unlikely relevant in our series, since the most common contrast agents during the study period (iohexol [Omnipaque™], iodixanol [Visipaque™], iopamidol [Isovue®], and Iopromide [Ultravist®]) are not strongly hepatotropic. A third possibility is that US artifacts such as reverberation can cause ducts to appear smaller than they actually are [24]. A fourth explanation is that the true duct size did actually change between studies, such that both US and CT were accurate and precise reflections of CBD diameter. Indeed, case reports have documented fluctuations of up to 13 mm, for example in a patient who passed a stone while in the emergency room [25]. However, as discussed above, this explanation is unlikely in our study, since in the vast majority of patients (70%), US was obtained prior to CT, such that if a passed stone explained the difference then the second study, the CT, should show a smaller CBD than the US, not vice versa.
Although there are many studies comparing various imaging modalities in their ability to detect choledocholithiasis [23, 26-29], we believe that this is the first study to focus on the comparison of bile-duct diameter per se in patients with gallstone pancreatitis. In a study focusing on elderly patients with acute cholecystitis, McGillicuddy, et al. [30] did compare CT and US findings and, in concordance with our study, found in the subgroup of patients undergoing both CT and US, the diameter of the CBD measured by CT was significantly larger than that measured by US (11.2 mm versus 8.7 mm, respectively). Similarly, Prpic et al. studying CBD diameter in healthy individuals, agreed with our finding that the diameter of bile ducts as measured by MRI highly correlated with US measurements [23].
Limitations of the study include its retrospective design. Data acquisition in such studies is imperfect. In addition, all the images were not reviewed and reported by the same radiologists. Although at first glance this appears to be a limitation, since the same highly experienced radiologists doing all the measurements would probably afford greater degree of standardization, nevertheless we wanted to capture the "real-world" phenomena, and therefore intentionally used exclusively the radiology reports as obtained at the time of patient presentation. We also recognize the paucity of paired CBD measurements available for analysis (Table 2 vs. Figure 1), but again, this is the nature of a retrospective chart review.
CONCLUSION
Although the diameter of CBD measured by US in the setting of acute gallstone pancreatitis was similar to the size measured by MRI, CBD diameter measured by CT was significantly greater than those measured by MRI and US, and should therefore be interpreted with caution.
Conflict of Interest
The authors declare that they have no conflict of interest.
References
- Cappell MS. Acute pancreatitis: etiology, clinical presentation, diagnosis, and therapy. Med Clin North Am 2008; 92:889-923. [PMID: 18570947]
- Fagenholz PJ, Fernandez-del Castillo C, Harris NS, Pelletier AJ, Camargo CA, Jr. Direct medical costs of acute pancreatitis hospitalizations in the United States. Pancreas 2007; 35:302-307. [PMID: 18090234]
- Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med 1994; 330:1198-1210. [PMID: 7811319]
- Frossard JL, Steer ML, Pastor CM. Acute pancreatitis. Lancet 2008; 371:143-152. [PMID: 18191686]
- Shmelev A, Sachdev S, Shah U, Abdo A, Kowdley GC, Cunningham SC. Energetic Etiologies of Acute Pancreatitis? An Observation., Pancreas Club, 49th Annual Meeting. Washington, DC: Pancreas Club, 2015.
- Shmelev A, Sachdev S, Shah U, Abdo A, Kowdley GC, Cunningham SC. Energetic etiologies of acute pancreatitis: A report of five cases. World J Gastrointest Pathophysiol 2015;4:243-8.
- Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med 2006; 354:2142-2150. [PMID: 16707751]
- Kimura Y, Arata S, Takada T, Hirata K, Yoshida M, Mayumi T, et al. Gallstone-induced acute pancreatitis. J Hepatobiliary Pancreat Sci 2010:17:60-69. [PMID: 20012326]
- Cucher D, Kulvatunyou N, Green DJ, Jie T, Ong ES. Gallstone pancreatitis: a review. Surg Clin North Am 2014:94:257-280. [PMID: 24679420]
- Shiozawa S, Tsuchiya A, Kim DH, Usui T, Masuda T, Kubota K, et al. Useful predictive factors of common bile duct stones prior to laparoscopic cholecystectomy for gallstones. Hepatogastroenterology 2005; 52:1662-1665. [PMID: 16334752]
- Hunt DR, Reiter L, Scott AJ. Pre-operative ultrasound measurement of bile duct diameter: basis for selective cholangiography. Aust N Z J Surg 1990; 60:189-192. [PMID: 2183754]
- Levin DC, Rao VM, Parker L, Frangos AJ, Sunshine JH. Recent trends in utilization rates of abdominal imaging: the relative roles of radiologists and nonradiologist physicians. J Am Coll Radiol 2008:5:744-747. [PMID: 18514954]
- Kocher KE, Meurer WJ, Fazel R, Scott PA, Krumholz HM, Nallamothu BK. National trends in use of computed tomography in the emergency department. Ann Emerg Med 2011; 58:452-462 e453. [PMID: 21835499]
- Moreau JA, Zinsmeister AR, Melton LJ, 3rd, DiMagno EP. Gallstone pancreatitis and the effect of cholecystectomy: a population-based cohort study. Mayo Clin Proc 1988; 63:466-473. [PMID: 3361956]
- Friedman GD. Natural history of asymptomatic and symptomatic gallstones. Am J Surg 1993:165:399-404. [PMID: ]
- Friedman GD, Raviola CA, Fireman B. Prognosis of gallstones with mild or no symptoms: 25 years of follow-up in a health maintenance organization. Journal of clinical epidemiology 1989; 42:127-136. [PMID: 2918322]
- Banks PA, Freeman ML, Practice Parameters Committee of the American College of G. Practice guidelines in acute pancreatitis. Am J Gastroenterol 2006; 101:2379-2400. [PMID: 17032204]
- Sabo A, Goussous N, Sardana N, Patel S, Cunningham SC. Necrotizing pancreatitis: A review of multidisciplinary management. JOP. J Pancreas 2015; 16:1. [PMID: 25791545]
- Ranson JH. The timing of biliary surgery in acute pancreatitis. Ann Surg 1979; 189:654-663. [PMID: 443917].
- Uhl W, Muller CA, Krahenbuhl L, Schmid SW, Scholzel S, Buchler MW. Acute gallstone pancreatitis: timing of laparoscopic cholecystectomy in mild and severe disease. Surg Endosc 1999; 13:1070-1076. [PMID: 10556440]
- Bowie JD. What is the upper limit of normal for the common bile duct on ultrasound: how much do you want it to be? Am J Gastroenterol 2000; 95:897-900. [PMID: 10763933]
- Lal N, Mehra S, Lal V. Ultrasonographic measurement of normal common bile duct diameter and its correlation with age, sex and anthropometry. Journal of clinical and diagnostic research : JCDR 2014; 8:AC01-04. [PMID: 25653927].
- Prpic GL, Babic N, Marjan D, Pecina M, Marotti M. MR assessment of bile duct size in healthy individuals: comparison with US measurements. Collegium antropologicum 2007; 31:567-571. [PMID: 17847941]
- Sauerbrei EE, Cooperberg PL, Gordon P, Li D, Cohen MM, Burhenne HJ. The discrepancy between radiographic and sonographic bile-duct measurements. Radiology 1980; 137:751-755. [PMID: 7444058]
- Jafari D, Cheng AB, Dean AJ. Dynamic changes of common bile duct diameter during an episode of biliary colic, documented by ultrasonography. Ann Emerg Med 2013; 62:176-179. [PMID: 23489651]
- Kondo S, Isayama H, Akahane M, Toda N, Sasahira N, Nakai Y, et al. Detection of common bile duct stones: comparison between endoscopic ultrasonography, magnetic resonance cholangiography, and helical-computed-tomographic cholangiography. Eur J Radiol 2005:54:271-275. [PMID: 15837409]
- Sugiyama M, Atomi Y. Endosc opic ultrasonography for diagnosing choledocholithiasis: a prospective comparative study with ultrasonography and computed tomography. Gastrointest Endosc 1997:45:143-146. [PMID: 9040999]
- Sgouros SN, Bergele C. Endosc opic ultrasonography versus other diagnostic modalities in the diagnosis of choledocholithiasis. Dig Dis Sci 2006:51:2280-2286. [PMID: 17080253]
- Mitchell SE, Clark RA. A comparison of computed tomography and sonography in choledocholithiasis. AJR Am J Roentgenol 1984:142:729-733. [PMID: 6608232]
- McGillicuddy EA, Schuster KM, Brown E, Maxfield MW, Davis KA, Longo WE. Acute cholecystitis in the elderly: use of computed tomography and correlation with ultrasonography. Am J Surg 2011:202:524-527. [PMID: 21906722]

