Keywords
Demography; Mortality; Pancreatitis
INTRODUCTION
Acute pancreatitis is a relatively common clinical condition hallmarked by unregulated trypsin activity within the pancreatic acinar cell, leading to pancreatic autodigestion and parenchymal inflammation [1]. The most common risk factors for acute pancreatitis in adults are gallstone disease and excess alcohol ingestion [2, 3]. Chronic pancreatitis, on the other hand, is a progressive fibro-inflammatory disease characterized by irreversible loss of the pancreatic parenchyma and subsequent functional insufficiency [4]. Excess alcohol is the most common risk factor for chronic pancreatitis in adults. Although the pathogenesis differs for acute and chronic pancreatitis, patients with chronic disease frequently present with clinical episodes of acute pancreatitis [4, 5]. Both are associated with significant morbidity and substantial use of healthcare resources [6].
Each year in the United States more than 220,000 people are admitted to the hospital with pancreatitis, and the number of admissions is steadily increasing [6, 7]. From 1988 to 2002, hospital admissions due to acute pancreatitis rose from 101,000 to 210,000 annually, and the corresponding admission rate from 0.4 to 0.7 hospitalizations per 1,000 U.S. population [8]. Approximately 20% of these patients have a severe clinical course, and the overall mortality rate is between 2% and 6% [1, 8]. Despite major advances in intensive care units and other forms of supportive treatment, mortality rates from pancreatitis have not significantly declined [9].
The factors involved in inpatient mortality from pancreatitis have not been previously assessed on a large-scale basis. The aim of our study was to identify those factors strongly associated with pancreatitisrelated death in a large sample of hospitalized patients.
METHODS
Study Design and Population
We performed a retrospective analysis of the 2004 Healthcare Cost and Utilization Project (HCUP) database using its Nationwide Inpatient Sample (HCUP-NIS) to facilitate our search (https://www.ahrq.gov/data/hcup/). HCUP-NIS is the largest inpatient care database in the United States. It contains data from nearly 8 million hospital stays each year, and maintains discharge diagnoses and information from over 1,000 hospitals nationwide in 37 states. It is the only national hospital database containing charge information on all patients, regardless of payer; this includes patients covered by Medicare and Medicaid (U.S. Department of Health and Human Services; https://www.cms.hhs.gov/), private insurance, and the uninsured. It encompasses both urban and rural hospitals, as well as teaching and non-teaching institutions. Data elements available within the HCUP-NIS database include primary and secondary diagnoses, primary and secondary procedures, admission and discharge status, patient demographics, expected payment source, total charges, length of stay, and hospital characteristics.
In our study, the total burden of disease was captured using the admission diagnosis search criterion of “pancreatitis”. Mortality was ascertained by those patients who registered inpatient hospital death during 2004.
Potential Predictors of Mortality
Patient-related and hospital course-related characteristics were evaluated as potential predictors of mortality. Patient-related factors included age, race, gender, socioeconomic status, and the number of additional comorbid conditions or diagnoses. Age was categorized by using 65 years as cut-off value. Race was divided into six groups: Caucasian, African American, Hispanic, Asian or Pacific Islander, Native American, and others. Socioeconomic status was measured according to household income quartiles, and the number of additional diagnoses was categorized as less than, or equal to, 3 and more than 3 comorbid conditions.
Hospital course-related factors included length of stay and the number of inpatient hospital procedures. Length of stay was divided into four groups: less than 3 days, 3-7 days, 8-14 days, and more than 14 days. The number of inpatient procedures was categorized as one procedure or 2 or more procedures.
STATISTICS
Data are reported as mean±SD and frequencies. Statistical analyses were performed using Stata 9.0 (Stata Corp, College Station, TX, USA). The hierarchical log-linear models were used to test the distribution of race and hospital size. Univariate logistic regression analysis was performed keeping inpatient mortality as the main study outcome; odds ratios (ORs) and 95% confidence intervals (95% CIs) were computed. The simple contrast was applied to non-dichotomic factors. In addition, we used multiple logistic regression analysis in order to identify factors that were independently associated with mortality. Variables for the final logistic regression model were selected by using a stepwise procedure, and the most parsimonious predictive model was chosen using the Akaike Information Criterion (AIC).
A receiver-operator-characteristic (ROC) curve was assembled and the area under the curve (AUC) was analyzed to evaluate thresholds for patients with and without inpatient mortality to distinguish positives from negatives. For each decision threshold, the test sensitivity was derived from patients who had deceased, and the test specificity from patients who had not. Sensitivities and specificities were plotted as functions of each other, with the upper left-hand corner representing perfect discrimination.
RESULTS
In the year 2004, there were 78,864 patients admitted to U.S. hospitals with a primary diagnosis of pancreatitis and captured by the HCUP-NIS database. Varying degrees of data were available in each of the categories analyzed. Total of 57,068 patients had complete data available. Information from at least 57,068 patients was used during data analysis for each variable.
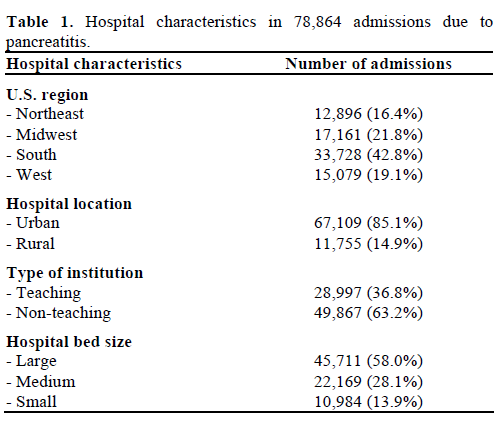
Table 1 highlights the characteristics of the hospitals that were used in our analysis. Four separate regions from within the United States were represented. The South region of the country registered the highest number of hospital admissions due to pancreatitis (33,728; 42.8%). Most patients were admitted to hospitals located in urban settings (67,109; 85.1%), and the majority were non-teaching institutions (49,867; 63.2%). Nearly 60% of patients received their care at a large-sized hospital (45,711; 58.0%); keeping in mind that hospital bed size was dependent upon hospital location according to the HCUP-NIS database (the cutoff for a “large” hospital in a Western rural community was 45 beds, as opposed to 425 beds for a Northeastern urban institution).
According to bed size, there were 13.9% admissions in small volume hospitals overall associated with a 2.3% mortality rate for pancreatitis (n=255). There were 28.1% admissions in medium-sized hospitals associated with a 2.4% mortality rate (n=536; OR=1.04, 95% CI: 0.90-1.21), and 58.0% admissions in large volume hospitals associated with a 2.9% mortality rate (n=1,310; OR=1.24; 95% CI: 1.08-1.42). Caucasian and Hispanic patients were more prevalent in small hospitals (P<0.001), while most African American patients were likely to present to large volume hospitals (P<0.001). Therefore, a significant higher frequencies of Asian or Pacific Islanders (P=0.015), Native Americans (P<0.001) and other races (P<0.001) were admitted in medium sized hospitals than in small or high sized ones (Table 2).

Table 3 demonstrates the inpatient demographics for all available data within the HCUP-NIS database. In 78,864 patients hospitalized with pancreatitis, 2,129 (2.7%) died prior to discharge. Mean age at the time of admission was 53.2±19.0 years, half were female (39,765 out of 78,662; 50.6%), and the majority of patients were Caucasian (36,728 out of 58,455; 62.8%). Mean number of comorbid conditions or additional diagnoses was 7.1±3.6.
In terms of hospital course, mean length of stay was 6.7±8.9 days. Average number of inpatient procedures was 1.5±2.1, and total hospital charges were $30,777±55,402. Ninety-two percent of hospital admissions (71,908 out of 78,542) were considered non-elective, or arrival through the emergency room (Table 3).
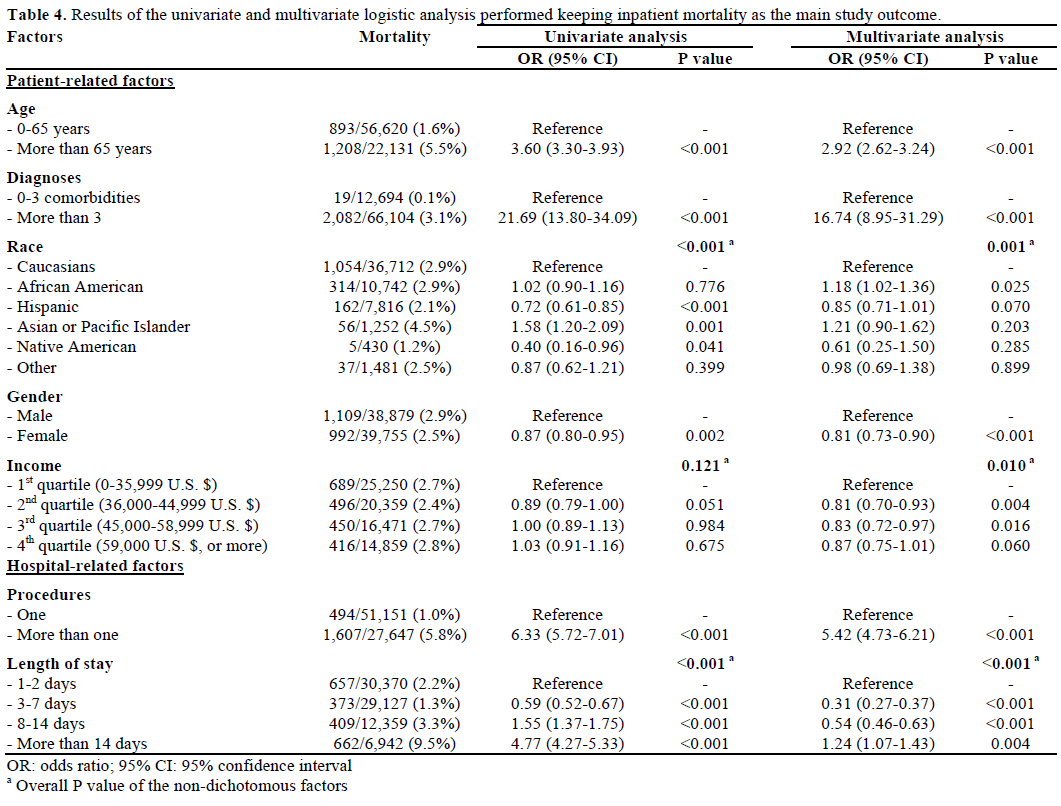
Results of the univariate logistic regression analysis are shown in Table 4, summarizing the odds ratios (ORs) with respective P-values for the seven separate groups of covariate factors most strongly associated with pancreatitis-related mortality. Among the patientrelated factors, age greater than 65 years old (OR=3.60, 95% CI: 3.30-3.93; P<0.001) and more than 3 comorbid conditions (OR=21.69, 95% CI: 13.80-34.09; P<0.001) were strongly associated with inpatient mortality. Compared to Caucasians, African American patients (OR=1.02, 95% CI: 0.90-1.16) and Asian patients (OR=1.58, 95% CI: 1.20-2.09) were more likely to die, but this was only statistically significant for Asian patients (P=0.001). Female gender was less associated with mortality (OR=0.87, 95% CI: 0.80- 0.95; P=0.002), and compared to patients in the lowest income quartile, those in the 2nd quartile were less likely to die (OR=0.89, 95% CI: 0.79-1.00; P=0.051).
Among the hospital course-related factors, univariate analysis showed a significant association with inpatient mortality in patients with more than one procedure (OR=6.33; 95% CI: 5.72-7.01; P<0.001; Table 4). Furthermore, increasing length of stay was strongly associated with increasing mortality (length of stay 8- 14 days, OR=1.55, 95% CI: 1.37-1.75, P<0.001; length of stay more than 14 days, OR=4.77, 95% CI: 4.27- 5.33, P<0.001) while the lowest mortality was found in patients with 3-7 days of length of stay (OR=0.59; 95% CI: 0.52-0.67).
The two rightmost columns of Table 4 highlight the results of the multivariate logistic regression analysis for the same seven groups of covariate factors. Again, there were significant correlations with pancreatitisrelated mortality in all seven categories. Age greater than 65 years old (OR=2.92, 95% CI: 2.62-3.24; P<0.001) and more than 3 comorbid conditions (OR=16.74, 95% CI: 8.95-31.29; P<0.001) were strong patient-related covariates. In terms of race, only African American race was significantly associated with mortality (OR=1.18, 95% CI: 1.02-1.36; P=0.025). Furthermore, females had a likely lower mortality than males (OR=0.81, 95% CI: 0.73-0.90; P<0.001); and compared to patients in the lowest income quartile, those in the 2nd and 3rd quartiles had also a likely lower probability to die (OR=0.81, 95% CI: 0.70-0.93; P=0.004 and OR=0.83, 95% CI: 0.72- 0.97; P=0.016, respectively). Those in the 4th quartile of income were 13% less likely to die, but this did not reach statistical significance (OR=0.87, 95% CI: 0.75- 1.01; P=0.060).
For the hospital course-related factors, multivariate analysis showed a significant association with inpatient mortality in patients with more than one procedure; OR=5.42, 95% CI: 4.73-6.21, P<0.001 (Table 4). Again, increasing length of stay was strongly associated with increasing pancreatitis-related mortality (length of stay greater than 14 days vs. 1-2 days: OR=1.24, 95% CI: 1.07-1.43, P=0.004) while patients with length of stay 3-7 days (OR=0.31, 95% CI: 0.27-0.37; P<0.001) and those with length of stay 8-14 days (OR=0.54, 95% CI: 0.46-0.63, P<0.001;) had significantly lower mortality than patients with 1-2 days of stay.
Finally, all seven covariate factors were used to generate the final multivariate logistic regression model and a score of the probability to death was computed for each patient by assigning 0 for factors in the reference category or the linear combination of the anti-log values of the ORs for factors different from the reference category. The ROC curve assembled by using this score yielded an AUC equal to 0.828 (95% CI: 0.820-0.837), suggesting high predictive value when estimating the likelihood of inpatient mortality (Figure 1).
Figure 1. ROC curve for the final predictive model.
DISCUSSION
Acute pancreatitis is a common disease that is primarily characterized by unregulated trypsin activity and pancreatic autodigestion with parenchymal inflammation [1]. It is associated with significant morbidity, and it may easily progress to a systemic inflammatory response syndrome with or without multi-organ dysfunction [10, 11, 12, 13, 14]. The most common risk factors for acute pancreatitis in adults are gallstone disease and excess alcohol ingestion [2, 3]. Other causes include medications, trauma, obstruction of the pancreatic duct (e.g., tumor), and certain metabolic derangements such as hypertriglyceridemia [1].
Chronic pancreatitis is a progressive fibro-inflammatory disease characterized by irreversible loss of the pancreatic parenchyma with subsequent functional insufficiency [4]. Excess alcohol is the most significant risk factor in adult patients, while genetic and anatomical defects predominate in children [5]. Morbidity associated with chronic pancreatitis includes chronic pain, intestinal malabsorption, pancreatic pseudocysts, peri-pancreatic ascites and fistulae, and duodenal and biliary obstruction [15]. Patients with chronic pancreatitis frequently present with clinical episodes of acute pancreatitis [4].
Over the past two decades, hospital admissions due to both acute and chronic pancreatitis have been steadily increasing [6, 8]. Despite major advances in intensive care units and other supportive treatments, the overall mortality rate from pancreatitis continues to be approximately 2-6% with each admission [1, 8]. The factors associated with this high rate of mortality have not been previously assessed on a large-scale basis. The aim of our study was to identify both patientrelated and hospital course-related factors that are strongly associated with death due to pancreatitis in hospitalized patients.
In our study, both univariate and multivariate logistic regression analysis confirmed several positive correlations between specific patient-related factors and inpatient mortality due to pancreatitis. Age greater than 65 years (OR=2.92, P<0.001) and the presence of more than 3 comorbid conditions (OR=16.74, P<0.001) were both strong and independent clinical predictors of mortality. Furthermore, female gender was associated with a decreased rate of mortality (OR=0.81, P<0.001), as were patients of higher economic status in the 2nd and 3rd quartiles of household income (OR=0.81, P=0.004, and OR=0.83, P=0.016 respectively). Lastly, of the various races analyzed, only African American race showed significant correlation with pancreatitis- 200
P=0.025). It should be noted that higher income and African American race (significantly lower mortality and higher mortality by multivariate analysis, respectively) were not statistically significant factors by univariate analysis. This may be due to their possible interplay with one another, creating somewhat of a “protective effect” from a positive association with mortality when each factor is not independently assessed.
In addition to patient-related factors, we analyzed hospital course-related characteristics that were potentially associated with mortality. In both univariate and multivariate analysis, increasing length of stay was associated with increasing rates of hospital mortality. Patients admitted for longer than 14 days were most likely to die (OR=1.24, P=0.004). Moreover, those patients that underwent more than one procedure during their hospitalization were also at greater risk for inpatient death (OR=5.42, P<0.001).
Other studies have examined the trends in hospital admissions and mortality due to acute and chronic pancreatitis [8, 16, 17, 18, 19]. Fagenholz et al. showed that hospital admissions for acute pancreatitis in the United States were higher among African Americans than Whites between the years 1988 and 2003 [8]. The overall mortality rate was 2%, with increasing age and male gender comprising two independent risk factors for hospital death. Our study confirms these findings, but further highlights the racial disparities among African Americans and Caucasians with respect to pancreatitis-related mortality. To our knowledge, Fagenholz et al. is the only other group that has previously identified these differences on such a largescale, nationwide inpatient study [8]. Furthermore, our study supports the relatively high overall mortality rate from pancreatitis (2.7%), and confirms the association between increasing age and inpatient death.
Why do these differences exist among patients hospitalized with pancreatitis? One theory is that patients of minority race and lower socioeconomic status have poorer access to healthcare and healthcare coverage [20, 21]. As a result, disease entities such as pancreatitis frequently present in later stages when the clinical course is severe, or the associated complications have already ensued. Later presentation or transfer from another hospital may translate into a more complicated hospital course in some settings [22], with an increased number of hospital procedures, length of stay, and overall mortality.
This concept of racial or economic disparities in hospitalized patients, however, is not unique when it comes to gastrointestinal-related diseases. Nguyen et al. reported colectomy rates to be significantly lower in African-American patients hospitalized with ulcerative colitis compared to Caucasians [23]. This same group reported lower rates of bowel resection in minority patients hospitalized with Crohn’s disease, and lower in-hospital mortality for wealthier individuals that resided in neighborhoods with a median household income above the national average [24]. Carbonell et al. analyzed over 93,000 cholecystectomy patients and demonstrated increasing length of stay in patients with lower household incomes [25]. Furthermore, Medicare and Medicaid insured patients had a higher length of stay, greater total charges, and higher rates of morbidity and mortality compared to privately-insured patients that were undergoing bariatric surgical procedures [26]. Despite these additional reports, racial and economic disparities in hospital mortality from pancreatitis have not been previously demonstrated. Our study shows significant differences in outcomes for minority and low-income patients, and it highlights a potential inequality of care in these subsets presenting with pancreatitis.
In terms of hospital-course characteristics associated with pancreatitis-related death, our study showed that greater length of stay and higher numbers of inpatient procedures were independent predictors of mortality. Length of stay in acute pancreatitis has been examined in the past, yet done so in the context of clinical factors that predict length of stay longer than seven days [27]. Length of stay and inpatient mortality, however, has not been previously studied, and our results suggest a higher risk of death with hospital stays greater than two weeks. Patients that fall into this category are likely those with severe acute pancreatitis and single-organ failure, or chronic pancreatitis with an associated complication. Patients with early severe acute pancreatitis and multi-organ failure often die within the first week of hospitalization [28, 29], and therefore likely comprise only a small minority of patients in our study that were alive longer than 14 days. In addition, inpatient procedures such as central line insertion, endoscopic retrograde cholangiopancreatography (ERCP), or catheter placement are often performed in patients with more severe disease, thus translating into a more complicated hospital course with a higher likelihood of mortality.
Our final predictive model incorporated the seven factors by multivariate analysis that proved to be the statistically significant risk factors for pancreatitisrelated death (age greater than 65 years, male gender, African American race, more than 3 additional diagnoses, low income, more than one hospital procedure, and length of stay greater than 14 days). Applying these risk factors, the model itself proved to be robust, with a good accuracy (AUC value of 0.828). This suggests good predictive value for estimating inpatient mortality in this subset of hospitalized patients admitted with pancreatitis.
The main limitation of our study stems from its retrospective design. It was not a prospective clinical trial with randomization and longitudinal follow-up. Instead we analyzed a single database with information accumulated from hundreds of hospitals around the country, grouping patients under the umbrella diagnosis of pancreatitis. As such, we are limited in both the extent and type of information available for each patient’s hospitalization. For example, specific information regarding the type of pancreatitis (i.e., acute vs. acute on chronic), patient body mass index (BMI), the presence of pancreatic necrosis, and/or the different types of inpatient procedures performed would be more helpful in our analysis, thus providing useful clinical correlates to specific factors involved in limiting overall and procedure-related mortality. Despite these clear limitations, the study encompasses a large population of patients with pancreatitis, and uncovers important patient-related and hospital-related characteristics that may contribute to inpatient mortality.
Overall, the results of our analysis suggest that several factors are associated with pancreatitis-related death in hospitalized patients. No single characteristic can reliably or accurately predict mortality, but rather a combination of factors (both patient-related and hospital course-related) should be used to predict inpatient death. In summary, our findings suggest that older age (more than 65-year-old), male gender, African American race, low household income, and a high number of coexisting medial conditions are the most important patient-related factors in predicting death from pancreatitis. At the same time, hospital course-related factors such as a prolonged stay (more than 14 days) and inpatient procedures (more than one procedure) are also strongly associated with mortality and should be used in combination with patient-related factors to predict pancreatitis-related death in hospitalized patients.
Awards/recognition
The abstract from this manuscript was presented as an “AGA Poster of Distinction” at Digestive Disease Week (DDW) 2008 in San Diego, CA, USA
Grant support None
Study sponsor None
Financial disclosures None of the authors of this manuscript have any relevant financial disclosures or conflicts of interest to state
References
- Whitcomb DC. Clinical practice. Acute pancreatitis. N Engl J Med 2006; 354:2142-50. [PMID 16707751]
- Venneman NG, Buskens E, Besselink MG, Stads S, Go PM, Bosscha K, et al. Small gallstones are associated with increased risk of acute pancreatitis: potential benefits of prophylactic cholecystectomy? Am J Gastroenterol 2005; 100:2540-50. [PMID 16279912]
- Lankisch PG, Lowenfels AB, Maisonneuve P. What is the risk of alcoholic pancreatitis in heavy drinkers? Pancreas 2002; 25:411-2. [PMID 12409838]
- Chari ST. Chronic pancreatitis: classification, relationship to acute pancreatitis, and early diagnosis. J Gastroenterol 2007; 42:58- 9. [PMID 17238029]
- Nair RJ, Lawler L, Miller MR. Chronic pancreatitis. Am Fam Physician 2007; 76:1679-88. [PMID 18092710]
- Spanier BW, Dijkgraaf MG, Bruno MJ. Epidemiology, aetiology and outcome of acute and chronic pancreatitis: An update. Best Pract Res Clin Gastroenterol 2008; 22:45-63. [PMID 18206812]
- DeFrances CJ, Hall MJ, Podgornik MN. 2003 National Hospital Discharge Survey. Advance data from vital and health statistics. No. 359. Hyattsville, MD: National Center for Health Statistics, 2005.
- Fagenholz PJ, Castillo CF, Harris NS, Pelletier AJ, Camargo CA Jr. Increasing United States hospital admissions for acute pancreatitis, 1988-2003. Ann Epidemiol 2007; 17:491-7. [PMID 17448682]
- McKay CJ, Imrie CW. The continuing challenge of early mortality in acute pancreatitis. Br J Surg 2004; 91:1243-4. [PMID 15382103]
- Forsmark CE, Toskes PP. Acute pancreatitis. Medical management. Crit Care Clin 1995; 11:295-309. [PMID 7788533]
- Winslet M, Hall C, London NJ, Neoptolemos JP. Relation of diagnostic serum amylase levels to aetiology and severity of acute pancreatitis. Gut 1992; 33:982-6. [PMID 1379569]
- Corfield AP, Cooper MJ, Williamson RC. Acute pancreatitis: a lethal disease of increasing incidence. Gut 1985; 26:724-9. [PMID 4018637]
- de Beaux AC, Palmer KR, Carter DC. Factors influencing morbidity and mortality in acute pancreatitis; an analysis of 279 cases. Gut 1995; 37:121-6. [PMID 7672660]
- Neoptolemos JP, Raraty M, Finch M, Sutton R. Acute pancreatitis: the substantial human and financial costs. Gut 1998; 42:886-91. [PMID 9691932]
- Steer ML, Waxman I, Freedman S. Chronic pancreatitis. N Engl J Med 1995; 332:1482-90. [PMID 7739686]
- Frey CF, Zhou H, Harvey DJ, White RH. The incidence and case-fatality rates of acute biliary, alcoholic, and idiopathic pancreatitis in California, 1994-2001. Pancreas 2006; 33:336-44. [PMID 17079936]
- Lindkvist B, Appelros S, Manjer J, Borgström A. Trends in incidence of acute pancreatitis in a Swedish population: is there really an increase? Clin Gastroenterol Hepatol 2004; 2:831-7. [PMID 15354285]
- Eland IA, Sturkenboom MJ, Wilson JH, Stricker BH. Incidence and mortality of acute pancreatitis between 1985 and 1995. Scand J Gastroenterol 2000; 35:1110-6. [PMID 11099067]
- Floyd A, Pedersen L, Nielsen GL, Thorladcius-Ussing O, Sorensen HT. Secular trends in incidence and 30-day case fatality of acute pancreatitis in North Jutland County, Denmark: a registerbased study from 1981-2000. Scand J Gastroenterol 2002; 37:1461-5. [PMID 12523598]
- Dark CK, Ezenkwele UA. Access to care as a predictor of patients' knowledge of cardiovascular diseases. J Natl Med Assoc 2007; 99:1338-46. [PMID 18229770]
- Arthur M, Hedges JR, Newgard CD, Diggs BS, Mullins RJ. Racial disparities in mortality among adults hospitalized after injury. Med Care 2008; 46:192-9. [PMID 18219248]
- Hill AD, Vingilis E, Martin CM, Hartford K, Speechley KN. Interhospital transfer of critically ill patients: demographic and outcomes comparison with nontransferred intensive care unit patients. J Crit Care 2007; 22:290-5. [PMID 18086399]
- Nguyen GC, Laveist TA, Gearhart S, Bayless TM, Brant SR. Racial and geographic variations in colectomy rates among hospitalized ulcerative colitis patients. Clin Gastroenterol Hepatol 2006; 4:1507-13. [PMID 17162242]
- Nguyen GC, Bayless TM, Powe NR, Laveist TA, Brant SR. Race and health insurance are predictors of hospitalized Crohn's disease patients undergoing bowel resection. Inflamm Bowel Dis 2007; 13:1408-16. [PMID 17567876]
- Carbonell AM, Lincourt AE, Kercher KW, Matthews BD, Cobb WS, Sing RF, Heniford BT. Do patient or hospital demographics predict cholecystectomy outcomes? A nationwide study of 93,578 patients. Surg Endosc 2005; 19:767-73. [PMID 15868259]
- Carbonell AM, Lincourt AE, Matthews BD, Kercher KW, Sing RF, Heniford BT. National study of the effect of patient and hospital characteristics on bariatric surgery outcomes. Am Surg 2005; 71:308-14. [PMID 15943404]
- Pofahl WE, Walczak SM, Rhone E, Izenberg SD. Use of an artificial neural network to predict length of stay in acute pancreatitis. Am Surg 1998; 64:868-72. [PMID 9731816]
- Isenmann R, Rau B, Beger HG. Early severe acute pancreatitis: characteristics of a new subgroup. Pancreas 2001; 22:274-8. [PMID 11291929]
- Beger HG, Rau BM. Severe acute pancreatitis: Clinical course and management. World J Gastroenterol 2007; 13:5043-51. [PMID 17876868]


