Keywords
Carcinoembryonic Antigen; Pancreas
Abbreviations
BD branch duct; ENPD endoscopic naso-pancreatic
drainage; IPMN intraductal papillary mucinous neoplasm; MD main
duct; MPD main pancreatic duct; RPJC repeated pancreatic juice
cytology
INTRODUCTION
IPMN of the pancreas is characterized by papillary
proliferation of columnar mucin-producing epithelial
cells [1]. IPMNs show a wide histological spectrum and
are suspected of progressing to invasive carcinomas in
the adenoma–carcinoma sequence [2]. Surgical resection
provides the best chance for cure in patients with
malignant IPMN. According to the 2012 revised consensus
guidelines (Fukuoka guidelines) [3], patients with Main
duct (MD)-IPMN and Branch duct (BD)-IPMN with “highrisk stigmata,” including obstructive jaundice, enhanced
solid components, or dilation of the main pancreatic duct
(MPD) to a diameter >10 mm, are strongly recommended
for surgical resection. On the other hand, the surgical
indication for patients with “worrisome features” is still
unclear.
If image modalities, including computed tomography
(CT), magnetic resonance cholangiopancreatography
(MRCP), and endoscopic ultrasonography (EUS), do not
provide sufficient information to decide the surgical
indication, further approaches, such as EUS-fineneedle
aspiration (EUS-FNA) or endoscopic retrograde
pancreatography (ERP) may be considered. Although
routine EUS-FNA or ERP for the evaluation of malignant
IPMN is not recommended in the international
consensus guideline, cytological results with fluid
collection or pancreatic juice sometimes are critical
for the management of IPMN, and molecular analysis,
including the use of tumor markers, with these samples
has been reported to be useful for evaluating malignant
IPMN [4, 5, 6].
Cytological examination of pancreatic juice obtained
during endoscopic retrograde cholangiopancreatography
(ERCP) is well established. In the last decade, EUS-FNAbased
cytology has been increasingly used worldwide;
however, the cytological diagnostic ability has not been
satisfactory because of its low sensitivity [7, 8, 9, 10, 11]. A recent meta-analysis of EUS-FNA-based cytology
revealed that it had good specificity but poor sensitivity
in differentiating malignant from benign IPMN [12]. In
addition, EUS-FNA-based cytology for mucinous cystic
lesions is not generally performed in Japan because of the
potential for seeding of tumor cells after EUS-FNA [13].
Recently, the usefulness of the repeated pancreatic juice
cytology (RPJC) method via endoscopic naso-pancreatic
drainage (ENPD) tube has been reported for diagnosis of
pancreatic neoplasm, especially of early pancreatic cancer
[14, 15, 16]; however, it is unclear whether this method is
useful and feasible for diagnosis of IPMN [17].
Cyst fluid CEA level has been reported to be a useful
marker for differentiation of mucinous from non-mucinous
cysts [7, 18], but it is of limited value for differentiation of
benign from malignant pancreatic cystic lesions [19]. When
only patients with IPMN were analyzed, the diagnostic
ability of cyst fluid CEA level to distinguish malignant from
benign IPMN has given inconsistent results [4, 20, 21, 22].
A more recent report indicated that CEA level in pancreatic
juice was a useful predictor of malignant IPMN [23, 24]. So,
far, studies analyzing CEA level of pancreatic juice have not
been reported from other institutions.
CEA immunohistochemical expression has been
reported to correlate with histological grade of IPMN
in resected tissues [25]. There has been only one study
examining the relationship between cyst fluid CEA levels
and degree of dysplasia. This study reported that CEA
levels increased as the histologic grade of dysplasia
progressed from low to high; however, CEA levels declined
once invasive cancer developed [22]. To the best of our
knowledge, there has been no report on the relationship
of CEA level of cyst fluid or pancreatic juice and CEA
expression in resected tissues of IPMN.
In this study, we compared the usefulness and feasibility
of the RPJC method with those of the conventional method
in patients with IPMN. We also evaluated use of the CEA
level of pancreatic juice combined with the RPJC method
for differentiation of malignant IPMN. In addition, we
accessed the relationship between CEA level of pancreatic
juice and immunohistochemical CEA expression in
resected species of IPMN.
Methods
Patients
The subjects were 75 consecutive patients (56
men and 19 women; mean age, 68.3 years) with IPMN
who underwent ERCP and aspiration cytology of pure
pancreatic juice between March 2004 and February
2015. The patient characteristics diagnosed by EUS, CT, or MRCP were consistent with the 2006 criteria, which
included branch type of IPMN with cyst size >30 mm and
presence of nodules or MPD dilatation or the main duct
type of IPMN. The histology of IPMN was based on analysis
obtained during surgery (n=72). All resected specimens
were examined pathologically and classified into four
groups: IPMN with low-grade dysplasia (LGD), IPMN with
intermediate-grade dysplasia (IGD), IPMN with high-grade
dysplasia (HGD), and IPMN with an associated invasive
carcinoma, according to the World Health Organization
classification [1]. Malignant IPMN was defined as HGD
and invasive carcinoma. In the absence of surgery,
the reference standard for the diagnosis of IPMC was
based on cytopathological detection of cancer cells from
pancreatic juice or liver tissues obtained by biopsy from
liver metastasis coupled with clinical and/or radiological
evidence of progressive disease (n=3). This study protocol
was approved by the ethics committee of our institution.
Cytological Examination
ERCP was performed by using a duodenoscope (JF
240 and JF 260V; Olympus Optical Co. Ltd., Tokyo, Japan).
Between March 2004 and January 2008, conventional
sampling of pure pancreatic juice for cytology and CEA
examination was performed during ERCP in 25 patients
with IPMN. These patients were examined by the
conventional method and classified as the “conventional
group.” Between January 2008 and January 2015, we
attempted to collect cytological samples of pancreatic juice
repeatedly by using an ENPD tube in 50 patients with IPMN
and could place the tube in 45 patients. These patients
were classified as the “RPJC group”. In this period, we
failed to place the ENPD tube in the MPD in five patients in
whom pancreatic juice could be obtained. These patients
were included as the “conventional cytology group”. The
RPJC method was performed as previously reported [15].
If possible, the tip of the tube was placed close to the cyst
or nodule in the MPD.
Pancreatic juice samples were centrifuged, and then
smears of cell pellets were made on slide glasses, fixed in
95% ethyl alcohol, and stained by using the Papanicolaou
technique. The cytological diagnoses were categorized into
the following five groups: benign/reactive process (class
1, 2), atypical cells (class 3), severe atypical cells (class
3b), malignancy strongly suspected (class 4), and cytology
conclusive for malignancy (class 5). Cytological results in
which malignancy was suspected (classes 3b and 4) or
conclusive (class 5) were regarded as cancer-positive, and
atypical results were regarded as cancer-negative.
The sensitivities, specificities, positive predictive
values, negative predictive values, and overall accuracies
of the RPJC and conventional method for malignant IPMN
were compared by χ2 test. In addition, the sensitivities
of RPJC for malignant IPMN were examined according to
clinical features, including type of IPMN, MPD diameter,
size of mural nodule, numbers of cytological samplings,
tumor location, and existence of invasion. A p value < 0.05
was considered to indicate statistical significance.
CEA Levels in Pancreatic Juice and CEA Immunohistochemistry
The CEA levels in the supernatant were measured
by means of a CEA immunometric chemiluminescent
assay kit (Fujirebio, Tokyo, Japan). The cutoff levels for
pancreatic juice CEA level were determined to maximize
the difference between benign and malignant IPMNs by
receiver operating characteristic (ROC) curve analysis.
Sections of formalin-fixed paraffin-embedded tissue
were subjected to immunohistochemistry using the avidin–
biotin complex method to characterize the tumor cells. We
used antibodies against carcinoembryonic antigen (NCLCEA-
2; Novocastra, Laboratories, UK; 1:100 dilution).
The extent of immunohistochemical staining was graded
by using a three-tiered scale. Positivity with apical or
cytoplasmic staining in <10% of the tumor cells was defined
as low, cases with 10–50% were defined as intermediate,
and cases with >50% were defined as high expression. The
relationship between CEA level of Pancreatic juice and CEA
immunohistochemical expression was evaluated by using
Spearman correlation coefficients.
Complications
After the procedure, the patients were carefully
observed for any complications. Procedure-induced
pancreatitis was defined as persistent abdominal pain
continuing for ≥24 hours in association with the serum
concentration of pancreatic enzyme (amylase) ≥3× the
upper limit of normal. Pancreatitis was graded according
to a modification of the 1991 consensus guidelines: mild,
requiring fasting and treatment for ≤3 days; moderate,
requiring fasting and treatment for 4–10 days; and severe,
requiring fasting and treatment for >10 days, intensive
care, or surgical intervention.
Frequencies of pancreatitis in the conventional and
RPJC groups were compared by using Fisher’s exact test.
A p value <0.05 was considered to indicate statistical
significance. IBM SPSS Statistics software version 20.0
(IBM Corporation, Chicago, IL) was used to perform all
statistical analyses.
Ehics
In this retrospective study, written informed consent
was not provided by the participants, but the documents
that explain how the data included in this study would
be used were displayed on bulletin board in Chiba
university hospital. The study protocol conforms to the
ethical guidelines of the “World Medical Association
Declaration of Helsinki - Ethical Principles for Medical
Research Involving Human Subjects” adopted by the 18th
WMA General Assembly, Helsinki, Finland, June 1964 and
amended by the 59th WMA General Assembly, Seoul, South
Korea, October 2008, as reflected in a priori approval by
our institutional review committee.
RESULTS
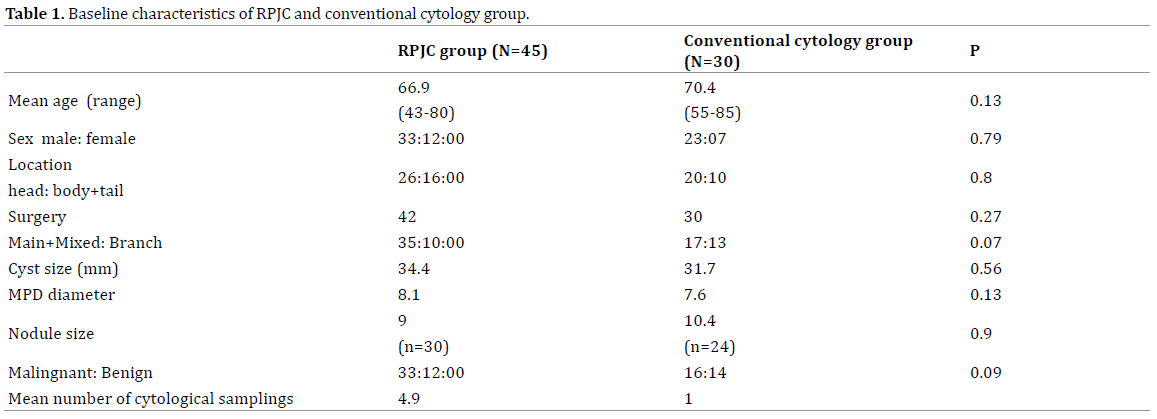
In the baseline characteristics, the conventional cytology
group tended to include more patients with the branch duct type of IPMN; therefore, the group tended to have more
patients with benign IPMN than did the RPJC group (Table
1). All 30 patients in the conventional cytology group and
42 patients (93%) in the RPJC group underwent surgery.
Surgery could not be performed on three patients because
two had metastatic cancer and one rejected surgery
because of old age. In the RPJC group, the mean number of
samples of collected pancreatic juice was 4.9. The overall
sensitivity, specificity, positive predictive value, negative
predictive value, and accuracy of the conventional method
for malignant IPMN were 12.5%, 100%, 100%, 52%, and
54%, respectively, and those of the RPJC method were 52%,
83%, 88%, 43%, and 60%, respectively, which showed
significantly higher sensitivity for the RPJC method than for
the conventional method (Table 2). In the RPJC group, there
were two false-positive cases: class 5 was detected in one
patient with branch duct type, and class 4 was detected in
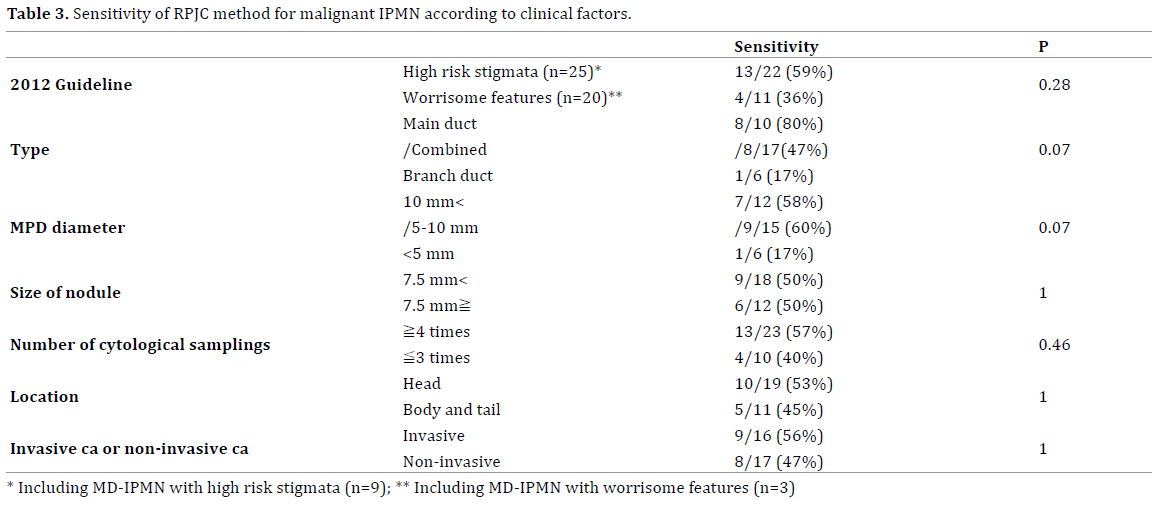
one patient with the other main duct type. The sensitivities of
the RPJC method according to clinical features, including the
type of IPMN, MPD diameter, size of mural nodule, numbers
of cytological samplings, tumor location, and existence of
invasion, are shown in Table 3. In these groups, 22 (88%) of
25 patients who had high-risk stigmata, including the main
duct type, and 11 (55%) of 20 patients who had worrisome
features were malignant. The sensitivities of the RPJC method
were 59% in the patients with high-risk stigmata and 39%
in the patients with worrisome features. The sensitivities of
the RPJC method tended to be higher in the main duct and
combined type of IPMN than in the branch duct type (59%
vs. 17%, p=0.07) and were not significantly different with
respect to the size of mural nodules, numbers of cytological
samplings, tumor location, and invasive or non-invasive
IPMC.

CEA Levels in Pancreatic Juice and CEA Immunohistochemistry
We examined CEA levels in the pancreatic juice of 47
IPMN patients (15 patients from the conventional cytology
group and 32 patients from the repeated cytology group)
obtained during ERP. The mean CEA level of pancreatic
juice was 1336 ng/mL in malignant IPMN and was 35.5 ng/
mL in benign IPMN, (p=0.02). According to the ROC curves
for CEA levels of pure pancreatic juice, the diagnostic cutoff
levels for differentiation from malignant IPMN was 72 ng/
mL and the area under the curve was 0.74 (Figure 1). The
sensitivity, specificity, and accuracy of the CEA cutoff level
were 48%, 85%, and 61%, respectively. If either the CEA
level in pancreatic juice was >72 ng/mL or cytological
malignancy was interpreted as positive, the sensitivity,
specificity, and accuracy were 67%, 88%, 72% in 32 IPMN
patients, were 67%, 83%, and 73% in the patients with
worrisome features (n=15), and were 83%, 75%, and 80%
in the patients with worrisome features and MPD ≥5 mm
(n=10) (Table 4).
Figure 1. According to the ROC curves for CEA levels of pure pancreatic
juice, the diagnostic cutoff levels for differentiation from malignant IPMN
was 72 ng/mL and the area under the curve was 0.74.

CEA immunohistochemistry was evaluated in 32 IPMN
patients, including 22 with malignant and 10 with benign
IPMN whose CEA levels of pancreatic juice were examined.
The relationship between CEA level of pancreatic juice and CEA immunoreactivity of the tissue sample is shown
in Figure 2. Malignancy was detected in 6 of 13 patients
with low or intermediate expression and in 16 of 19 with
high expression of CEA immunoreactivity. Malignancy
was significantly more often detected in patients with
high expression than in those with low and intermediate
expression (p=0.049). The mean CEA levels of the low,
intermediate, and high expression categories of CEA
immunoreactivity were 2.8 ng/mL, 32.9 ng/mL, and
1616.7 ng/mL, respectively. The CEA levels of pancreatic
juice were significantly different between the patients with
low and intermediate expression (p=0.04) and between
those with intermediate and high expression of CEA
immunoreactivity (p=0.01). The CEA level of pancreatic
juice positively correlated with CEA immunohistochemical
expression (r=0.67, p<0.01).
Figure 2. The relationship between CEA level of pancreatic juice and CEA immunoreactivity of tissue samples is shown. High CEA expression was detected
in 16 of 22 patients with malignant IPMN and in 3 of 10 patients with benign IPMN. High CEA expression was significantly more often detected in malignant
IPMN than in benign (p = 0.049). The mean CEA levels of low, intermediate, and high expression of CEA immunoreactivity are 2.8 ng/mL, 32.9 ng/mL, and
1616.7 ng/mL, respectively. The CEA levels of pancreatic juice are significantly different between the patients with low and intermediate expressions (p =
0.04) and between those with intermediate and high expressions of CEA immunoreactivity (p = 0.01). The CEA level of pancreatic juice positively correlates
with CEA immunohistochemical expression (r = 0.67, p < 0.01).
☐ indicates benign IPMN, and ◆ indicates malignant IPMN.
Complications
Post-ERCP pancreatitis was identified in 4 patients
(8.9%) in the RPJC group and in two patients (7.1%) in
the conventional cytology group, but the difference was
not significant. In the RPJC group, two patients (5.7%)
developed mild pancreatitis in the main duct and combined
type of IPMN; on the other hand, in the branch duct type
of IPMN, two patients (20%) developed pancreatitis,
including one with mild and one with moderate severity.
All of them were cured by conservative treatment.
DISCUSSION
In this study, we first separately examined the diagnostic
abilities of the RPJC method and CEA level of pancreatic
juice and found that their sensitivities were insufficient for differentiation of malignant IPMN. However, if the
RPJC method results were combined with a CEA level in
pancreatic juice >72 ng/mL, the sensitivity and accuracy
improved to >80%, especially in patients with “worrisome
features” whose MPD size was 5–9 mm.
Cytological examination of pancreatic juice obtained
during ERCP has been performed since ERCP was first
introduced, and its sensitivity for malignant IPMN has
been reported to range from 30–40% [10, 11]. Recently,
excellent results of PJC using balloon catheter or lavage
cytology with cell block have been reported [26, 27].
Regarding cytological interpretation, severe atypical cells
(class 3b) were interpreted as cancer-positive in our study
because high-grade epithelial atypia has been reported
as being a more sensitive predictor of malignancy than
positive cytology [28, 29]. However, the 12.5% sensitivity
for the conventional method was relatively lower than the
levels reported in other studies. This result may be because
of the unavailability of secretin, which was discontinued
in Japan in 2004. The sensitivity of the repeated cytology
method was 57%, which was significantly higher than that
of the conventional method (p=0.01). The sensitivities
of the repeated cytology method tended to be higher for
the main duct and combined types of IPMN than for the
branch duct type (59% vs. 17%, p=0.07). Positive results
of pancreatic juice cytology were more likely to be easily
obtained when malignant IPMN was present in the MPD.
However, the sensitivity of this method was insufficient for
differentiation of malignant from benign IPMN, especially in
the 39% of patients with “worrisome features” (Figure 3).
Figure 3. (a). In a 58-year-old woman, multidetector-row CT showed main pancreatic duct dilatation with a diameter of 8 mm without an apparent nodule
that is categorized as MD-IPMN with “worrisome features.” (b). ERP was performed, the ENPD tube was left in place for 3 days, and cytological samples
were collected six times; the samples are class 3, 3, 3, 5, 3, and 4, respectively. (c). Cytological diagnosis is positive at the fourth and sixth samplings. (d). After examination by pancreatoscopy, a total pancreatectomy was performed. Pathological examination of the resected specimen showing micro invasive
IPMC. (e). The CEA levels of pancreatic juice are 1580 ng/mL, and CEA immunohistochemical analysis indicates high expression.
According to the 2012 revised consensus guidelines,
patients with MD-IPMN and BD-IPMN with “high-risk
stigmata” are recommended for surgical resection. In
contrast, patients with BD-IPMN with “worrisome features”
are recommended for evaluation without immediate
resection. In fact, our data showed that 22 (88%) of 25
patients who had high-risk stigmata, including MD-IPMN,
and 11 (55%) of 20 patients who had worrisome features,
including MD-IPMN with MPD<10 mm, had malignancies.
With regard to MD-IPMN, 8 (89%) of 9 patients with highrisk
stigmata and 2 (67%) of 3 with worrisome features
had malignancies. Therefore, further improvements are
required to differentiate benign from malignant IPMN,
especially in patients with worrisome features, including
MD-IPMN with MPD<10 mm.
Marie F et al. reported that a cyst fluid CEA
concentration >200 ng/mL had sensitivity and specificity
of 90% and 71%, respectively, for diagnosis of malignant
IPMN [4]; however, these data have not been reproduced in subsequent studies, so its ability to distinguish
malignant IPMN is controversial. Recent meta-analysis
showed that CEA cutoff levels for determining a malignant
cyst have ranged from 109.9–6000 ng/mL, and pooled
estimates of CEA in malignant cysts have led to poor
prediction. On the other hand, Hirono S et al. reported
that a CEA concentration >110 ng/mL in pancreatic juice
was the only independent predictive factor for malignant
IPMN [23]. More recently, they also reported that a CEA
concentration >30 ng/mL had sensitivity, specificity, and
accuracy of 94%, 85%, and 80%, respectively, for diagnosis
of malignant BD-IPMN [24]. These results were difficult to
compare because the specimens (cyst fluid or pancreatic
juice), sampling method (EUS-FNA or ERCP), and variety
of pancreatic cyst were different. We speculated that CEA
levels of pancreatic juice may reflect secretion of CEA from
tumor cells of the MPD as well as the branch duct. In this
study, the CEA cutoff concentration was 72 ng/mL for
differentiation of malignant from benign IPMN, and a CEA
concentration >72 ng/mL had sensitivity and specificity of
48% and 85%, respectively. From our results, it appeared
that the CEA level of pancreatic juice was of limited value
in differentiating malignant from benign IPMN. However,
if the RPJC method results and a CEA level >72 ng/mL
in pancreatic juice were combined, the sensitivity and
accuracy improved.
CEA immunohistochemical analysis revealed that high
CEA expression was significantly more often detected in
malignant IPMN than in benign IPMN and that the CEA level of pancreatic juice correlated with CEA expression.
However, 4 of 17 malignant patients with IPMN and
high CEA expression had low CEA concentrations of
pancreatic juice, which caused the sensitivity of CEA level
of pancreatic juice for differentiation of malignant IPMN to
be low. Interestingly, these four patients all had invasive
IPMC. Kucera S et al. reported that cyst fluid CEA level
increased with increasing histological grade but declined
with development of invasive cancer. They speculated that
fewer cells with tight junctions were present and therefore,
there was less CEA at the luminal surface available for
release into the cystic fluid.
The major complication associated with ERCP is post-
ERCP pancreatitis, the incidence of which varies widely
from 1–8%. In the present study, post-ERCP pancreatitis
occurred in two patients (6.7%) in the conventional group
and in four patients (8.9%) of the repeated cytology
group, all of which resolved with conservative treatment.
The incidence of pancreatitis was slightly higher in the
conventional group than in the repeated cytology group,
possibly because the viscosity of the pancreatic juice may
have slowed flow through the ENPD tube. In addition,
pancreatitis tended to occur more in BD-IPMN patients
(20%) than in MD and combined IPMN patients (5.7%).
This finding might have been related to the presence of
chronic obstructive pancreatitis by mucin, which could have
developed in more cases of MD and combined IPMN than
in cases of BD-IPMN and resulted in a lower incidence of
post-ERCP pancreatitis. These findings were similar to those
reported previously in which pancreatic stent placement
increased the post-ERCP pancreatitis in male patients with
IPMN, possibly because of obstruction by mucin, but no
patients with a dilatation of the MPD >6 mm had post-ERCP
pancreatitis [30]. Considering this frequency of pancreatitis
and its low sensitivity, the RPJC method does not appear to be
suitable for patients with BD-IPMN.
There were some limitations in this study. This was
a retrospective study with a small number of patients
conducted at a single tertiary center. In addition, there may
have been a selection bias because we could not perform
ERCP with pancreatic juice cytology and CEA analysis of
pancreatic juice consequently.
CONCLUSION
In conclusion, the repeated cytological method
was found to be feasible for IPMN patients with MPD
diameters ≥5 mm. This method combined with a CEA
level of pancreatic juice may be useful for patients with
“worrisome features” and MPD diameters from 5–9 mm.
Further studies with larger numbers of patients will be
needed to confirm the reliability of this method.
ACKNOWLEDGMENTS
The authors would like to thank Enago (www.enago.jp)
for the English language review.
Supported by the KAKENHI grants 24501337
Conflict of Interest
The authors have no conflicts to disclose. All authors
disclosed no financial relationships relevant to this
publication.
References
- Bosman FT, Carneiro F, Hruban RH, Theise N. WHO classification of
tumours of the digestive system. 4th ed Geneva: WHO 2010
- Kloppel G, Solcia E, Longnecker DS, Capella C, Sobin LH. Histological
typing of tumours of the exocrine pancreas. World Health Organization
International histological classification of tumours 2nd Ed Berlin:
Springer-Verlag 1996.
- Tanaka M, Fernandez-del Castillo C, Adsay V, Chari S, Falconi M,
Jang JY, et al. International Association of P. International consensus
guidelines 2012 for the management of IPMN and MCN of the pancreas.
Pancreatology 2012; 12:183-197. [PMID: 22687371]
- Maire F, Voitot H, Aubert A, Palazzo L, O'Toole D, Couvelard A,
et al. Intraductal papillary mucinous neoplasms of the pancreas:
performance of pancreatic fluid analysis for positive diagnosis and
the prediction of malignancy. Am J Gastroenterol 2008; 103:2871-7.
[PMID: 18775021]
- Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N, Ahmad N,
et al. Pancreatic cyst fluid DNA analysis in evaluating pancreatic cysts:
a report of the PANDA study. Gastrointest Endosc 2009; 69:1095-102.
[PMID: 19152896]
- Singhi AD, Nikiforova MN, Fasanella KE, McGrath KM, Pai RK, Ohori NP,
et al. Preoperative GNAS and KRAS testing in the diagnosis of pancreatic
mucinous cysts. Clin Cancer Res 2014; 20:4381-9. [PMID: 24938521]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E. Diagnosis of
pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst
study. Gastroenterology 2004; 126:1330-6. [PMID: 15131794]
- Frossard JL, Amouyal P, Amouyal G. Performance of endosonographyguided
fine needle aspiration and biopsy in the diagnosis of pancreatic
cystic lesions. Am J Gastroenterol 2003; 98:1516-24. [PMID: 12873573]
- Sedlack R, Affi A, Vazquez-Sequeiros E. Utility of EUS in the evaluation
of cystic pancreatic lesions. Gastrointest Endosc 2002; 56:543-7. [PMID:
12297771]
- Yamaguchi K, Nakamura M, Shirahane K, Kawamoto M, Konomi
H, Ohta M, et al. Pancreatic juice cytology in IPMN of the pancreas.
Pancreatology 2005; 5:416-21; discussion 421. [PMID: 15985766]
- Yamaguchi T, Shirai Y, Ishihara T, Sudo K, Nakagawa A, Ito H, et
al. Pancreatic juice cytology in the diagnosis of intraductal papillary
mucinous neoplasm of the pancreas: significance of sampling by peroral
pancreatoscopy. Cancer 2005; 104:2830-6. [PMID: 16287152]
- Suzuki R, Thosani N, Annangi S, Guha S, Bhutani MS. Diagnostic yield
of EUS-FNA-based cytology distinguishing malignant and benign IPMNs:
a systematic review and meta-analysis. Pancreatology 2014; 14:380-4.
[PMID: 25278308]
- Hirooka Y, Goto H, Itoh A, Hashimoto S, Niwa K, Ishikawa H, et al. Case
of intraductal papillary mucinous tumor in which endosonography-guided
fine-needle aspiration biopsy caused dissemination. J Gastroenterol
Hepatol 2003; 18:1323-4. [PMID: 14535994]
- Iiboshi T, Hanada K, Fukuda T, Yonehara S, Sasaki T, Chayama K.
Value of cytodiagnosis using endoscopic nasopancreatic drainage for
early diagnosis of pancreatic cancer: establishing a new method for the
early detection of pancreatic carcinoma in situ. Pancreas 2012; 41:523-9.
[PMID: 22504379]
- Mikata R, Ishihara T, Tada M, Tawada K, Saito M, Kurosawa J, et al.
Clinical usefulness of repeated pancreatic juice cytology via endoscopic
naso-pancreatic drainage tube in patients with pancreatic cancer. J
Gastroenterol 2013; 48:866-73. [PMID: 23053424]
- Hanada K, Okazaki A, Hirano N, Izumi Y, Minami T, Ikemoto J,
et al. Diagnostic strategies for early pancreatic cancer. Journal of
gastroenterology 2015; 147-54. [PMID: 26651254]
- Iwata T, Kitamura K, Yamamiya A, Ishii Y, Sato Y, Nomoto T, et al.
Evaluation of diagnostic cytology via endoscopic naso-pancreatic
drainage for pancreatic tumor. World J Gastrointest Endosc 2014; 6: 366-
72. [PMID: 25132920]
- Park WG, Mascarenhas R, Palaez-Luna M, Smyrk TC, O'Kane D, Clain
JE, et al. Diagnostic performance of cyst fluid carcinoembryonic antigen
and amylase in histologically confirmed pancreatic cysts. Pancreas 2011;
40:42-5. [PMID: 20966811]
- Ngamruengphong S, Michael J. Bartel, Massimo Raimondo. Cyst
carcinoembryonic antigen in differentiating pancreatic cysts: A metaanalysis.
Dig Liver Dis 2013; 45: 920-6. [PMID: 23790480]
- Pitman MB, Michaels PJ, Deshpande V, Brugge WR, Bounds BC.
Cytological and cyst fluid analysis of small (< or =3 cm) branch duct
intraductal papillary mucinous neoplasms adds value to patient
management decisions. Pancreatology 2008; 8:277-84. [PMID: 18497541]
- Pais SA, Attasaranya S, Leblanc JK, Sherman S, Schmidt CM, DeWitt
J. Role of endoscopic ultrasound in the diagnosis of intraductal papillary
mucinous neoplasms: correlation with surgical histopathology. Clin
Gastroenterol Hepatol 2007; 5:489-95. [PMID: 17350894]
- Kucera S, Centeno BS, Springett G, Malafa MP, Chen YA, Weber J, et
al. Cyst fluid carcinoembryonic antigen level is not predictive of invasive
cancer in patients with intraductal papillary mucinous neoplasm of the
pancreas. JOP 2012; 13:409-13. [PMID: 22797397]
- Hirono S, Tani M, Kawai M, Ina S, Nishioka R, Miyazawa M et al.
Treatment strategy for intraductal papillary mucinous neoplasm of
the pancreas based on malignant predictive factors. Arch Surg 2009;
144:345-349. [PMID: 19380648]
- Hirono S, Tani M, Kawai M, Okada K, Miyazawa M, Shimizu A, et
al. The carcinoembryonic antigen level in pancreatic juice and mural
nodule size are predictors of malignancy for branch duct type intraductal
papillary mucinous neoplasms of the pancreas. Arch Surg 2012; 255:517-
22. [PMID: 22301608]
- Fukushima N, Mukai K, Sakamoto M, Hasebe T, Shimada K, Kosuge
T, et al. Invasive carcinoma derived from intraductal papillary-mucinous
carcinoma of the pancreas: clinicopathologic and immunohistochemical
study of eight cases. Virchows Archiv 2001; 439:6-13. [PMID: 11499841]
- Ohtsuka T, Matsunaga T, Kimura H, Watanabe Y, Tamura K, Ideno N,
et al. Role of pancreatic juice cytology in the preoperative management
of intraductal papillary mucinous neoplasm of the pancreas in the era of
international consensus guidelines 2012. World J Surg 2014; 38:2994-
3001. [PMID: 25037612]
- Sai JK, Nobukawa B, Matsumura Y, Watanabe S. Pancreatic duct
lavage cytology with the cell block method for discriminating benign and
malignant branch-duct type intraductal papillary mucinous neoplasms.
Gastrointestinal endoscopy 2013; 77:726-35. [PMID: 23290718]
- Pitman MB, Genevay M, Yaeger K, Chebib I, Turner BG, Mino-Kenudson
M, et al. High-grade atypical epithelial cells in pancreatic mucinous cysts
are a more accurate predictor of malignancy than "positive" cytology.
Cancer cytopathol 2010; 118:434-40. [PMID: 20931638]
- Pitman MB, Yaeger KA, Brugge WR, Mino-Kenudson M. Prospective
analysis of atypical epithelial cells as a high-risk cytologic feature for
malignancy in pancreatic cysts. Cancer cytopathol 2013; 121:29-36.
[PMID: 23132817]
- Harada R, Kawamoto H, Fukatsu H, Kato H, Hirao K, Kurihara N, et al.
Nonprevention of postyendoscopic retrograde cholangiopancreatographic
pancreatitis by pancreatic stent after aspiration of pure pancreatic juice in
patients with intraductal papillary mucinous neoplasms of the pancreas.
Pancreas 2010; 39:340-344. [PMID: 19823100]




