Keywords
Endoscopic ultrasound; Acute Pancreatitis;Pancreatic
cancer; Neoplasm
Abbreviations
EUS Endoscopic ultrasound; BISAP Bedside
Index of Severity in Acute Pancreatitis; CT Computed Tomography;
MRI Magnetic resonance imaging; MRCP Magnetic resonance
cholangiopancreatography; FNA Fine-Needle Aspiration; IPMN Intra-
Ductal Papillary Mucinous Neoplasm
INTRODUCTION
As high as a third of patients with acute pancreatitis
do not have an identifiable cause after initial evaluation
on history, physical examination, laboratory testing, and
abdominal imaging [1]. Endoscopic ultrasound (EUS)
provides high resolution imaging of the pancreatobilliary
system, which is important for evaluating causes of acute
pancreatitis, while maintaining a favorable safety profile
[2, 3]. Society guidelines recommend EUS for patients
>40 years of age with acute pancreatitis when standard
evaluation does not reveal a definite etiology, given the
possibility of occult pancreatic adenocarcinoma [4].
The timing of EUS in the setting of acute pancreatitis
is controversial given concerns that inflammation from acute pancreatitis may lead to missed lesions and impact
the safety of the procedure [2, 3]. In clinical practice,
endoscopists commonly delay performing EUS for >4-8
weeks after a presentation of acute pancreatitis, based
on expert opinion [2, 5, 6]. However, the disadvantages
of delaying EUS include missed or delayed diagnosis of
occult pancreaticobiliary tumors [3]. Limited studies
demonstrate that EUS without fine-needle aspiration (FNA)
in the setting of acute biliary pancreatitis can accurately
evaluate choledocholithiasis without impacting safety
[7, 8]. However, performing early EUS with FNA during
hospitalization among patients with acute pancreatitis is
currently not well described. The aim of the study is to
evaluate the diagnostic yield, safety, and completeness
of performing EUS in hospitalized patients with acute
pancreatitis, compared to those who received EUS after
hospitalization.
METHODS
Study Design
The study was approved by the Institutional Review
Board at Loma Linda University Medical Centre prior to
initiating the study. Consecutive patients who received
EUS for the primary indication of acute pancreatitis,
between 2007 and 2014, were searched using the internal
endoscopy database. The inclusion criteria consisted of
patients who received diagnostic EUS during or following
hospitalization for acute pancreatitis. Acute pancreatitis was defined by patients meeting at least 2 of the 3 criteria:
characteristic abdominal pain; amylase or/and lipase
elevated >3 times the upper limit of normal; and/or
radiographic evidence of pancreatitis on cross-sectional
imaging [9]. Patients who received EUS for drainage of
pancreatic fluid collections were excluded. Furthermore,
patients who were pregnant or age <18 years were also
excluded. In patients who had multiple EUS performed
during the study period, the initial procedure that
met inclusion criteria was considered the index case.
Patients’ medical records were reviewed to characterize
the clinical course before and after EUS following acute
pancreatitis.
The final cause of acute pancreatitis was determined
based on consistent history, biochemical testing,
abdominal imaging, and endoscopic ultrasound findings.
Clinical outcomes were obtained by reviewing medical
records including radiographic, endoscopic, surgical, and
histologic report to characterize the clinical course and to
establish the cause of acute pancreatitis. When possible,
telephone consent and survey were conducted to clarify
patient’s clinical status, recurrence of acute pancreatitis,
and change in cause of acute pancreatitis.
Data Collection
Demographic data including sex, age, and race/
ethnicity were obtained. Furthermore, first or recurrent
episodes of acute pancreatitis, smoking history, alcohol
use, family history of pancreatitis, and weight loss in the
last 6 months were recorded. Laboratory values including
serum amylase, lipase, bilirubin and alkaline phosphatase
levels at presentation of acute pancreatitis were recorded.
Triglycerides, calcium, APACHEII score (age, vital signs,
complete blood count, basic metabolic profile and Glasgow
coma scale on admission) were also documented. All
radiographic studies (ultrasound, computed tomography
(CT), magnetic resonance imaging/magnetic resonance
cholangiopancreatography (MRI/MRCP) were reviewed.
Focal solid lesion in the pancreas was defined by
presence of a localized pancreatic or peri-pancreatic
mass, prominence, fullness, or enlargement documented
on ultrasound, CT, and/or MRI/MRCP. Focal cystic lesion
in the pancreas was defined by presence of a localized
pancreatic or peri-pancreatic cystic lesion documented
on ultrasound, CT, and/or MRI/MRCP. The Bedside
Index of Severity in Acute Pancreatitis (BISAP) score
was calculated for each patient [10]. Furthermore, the
severity of acute pancreatitis and presence of pancreatic
and/or peri-pancreatic fluid collections were categorized
according to the 2012 Atlanta Classification [11]. EUS
findings were reviewed in detail, noting specifically for the
presence of common bile duct stones/sludge, cystic and/
or solid mass, choledochal or pancreatic cysts, pancreatic
divisum, and the overall pancreatic parenchyma, as well as,
completeness of the examination. Chronic pancreatitis on
EUS was categorized on the basis of the Rosemont criteria
(consistent, suggestive, indeterminate, or normal) based
on index EUS findings [12].
Study Endpoints
The primary endpoint of the study was the proportion
of patients with a new cause of acute pancreatitis
identified following EUS. New cause of acute pancreatitis
was defined by typical EUS findings of microlithiasis,
choledocholithiasis, pancreatic divisum, or a cystic/
solid pancreatic mass as documented by the endoscopist.
Findings of chronic pancreatitis on EUS were not
considered a cause of acute pancreatitis. Secondary
endpoints were the proportion of patients with incomplete
EUS examination, adverse events associated with EUS, and
repeat EUS. An incomplete EUS examination was defined
by failure to advance the echoendoscope to the ampulla
and/or incomplete visualization of the pancreas.
Analysis
Descriptive statistics are reported as mean±standard
deviation (SD) for continuous variables or as median
and range otherwise. Comparison of proportional data
between the study groups was performed using Chi-square
or Fisher’s exact test where appropriate, and continuous
data was compared using t-test. Two-sided p-values <0.05
were considered significant.
RESULTS
Patient Characteristics
During the study period, 61 patients received EUS following
hospitalization for acute pancreatitis (Table 1). The mean
age was 50.2±18.7 years, 30 (49%) were male, and 21 (34%)
had a prior episode of acute pancreatitis. On presentation, the
median BISAP score was 1 (range 0-4), and 38 (62%) patients
had no definite etiology of acute pancreatitis after 47 (77%)
receiving documented cross-sectional imaging with CT and/
or MRI/MRCP. Cross-sectional imaging studies revealed solid
with or without cystic lesions in 12 (20%) patients and cystic
lesions in 17 (28%) patients. Of the 23 (38%) patients with a
possible cause of acute pancreatitis (alcohol in 12, gallstone
in 5, hypertriglyceridemia in 3, medication-induced in 2, and
ischemic in 1), 14 (61%) had solid and/or cystic lesions in
the pancreas on cross-sectional imaging. Of the 38 patients
without a cause of acute pancreatitis, 15 (39%) had solid
and/or cystic lesions in the pancreas on cross-sectional
imaging (Table 2).


Endoscopic Ultrasound Outcomes
Following acute pancreatitis, EUS was performed at
a median of 23 days (range 1-438) from presentation
including 29 (47%) during the index hospitalization and
32 (53%) after discharge. Eight (13%) patients received
EUS<72 hours, 8 (13%) received EUS 3-7 days, 18 (30%)
received EUS 7-28 days, and 27 (44%) received EUS>28
days from the onset of acute pancreatitis. Fifty-five (90%)
of patients received EUS with moderate sedation and 23
(38%) received FNA.
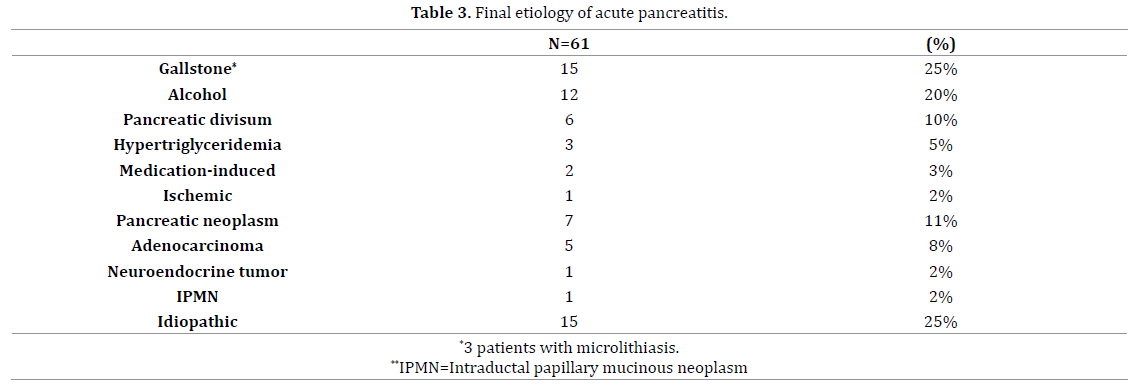
Following EUS, 15 (24%) patients received a new
diagnosis (Table 3) including 6 (10%) with pancreatic
neoplasm (adenocarcinoma in 4, neuroendocrine tumour in 1, intra-ductal papillary mucinous neoplasm (IPMN) in 1)
and 9 (14%) with benign etiologies (pancreatic divisum in
6, microlithiasis/choledocholithiasis in 3). Furthermore of
the 28 patients with solid with or without cystic pancreatic
lesions (N=11) or cystic pancreatic lesions (N=17) on
cross-sectional imaging, 3 (10%) were diagnosed with
pancreatic neoplasms (pancreatic adenocarcinoma in
1, pancreatic neuroendocrine tumour in 1, and IPMN in
1). Four (7%) patients, including 3 receiving moderate
sedation and 1 receiving anaesthesia assistance, had
incomplete EUS examinations (difficulty with sedation in
2, inability to intubate the second portion of the duodenum
in 1, altered anatomy in 1). No adverse events related to
the EUS were documented. Subsequently, 9 (7%) received repeat EUS at median of 21 days (range 1-1,078 days) from
the initial examination without a change or new diagnosis
in any of the patients.
Clinical Outcomes
During mean follow up of 3.7±3.5 years, one patient
who received EUS during hospitalization had a change in
diagnosis (pancreatic adenocarcinoma). Furthermore, 3
(5%) patients including 2 who received EUS during and 1
after hospitalization developed recurrent acute pancreatitis
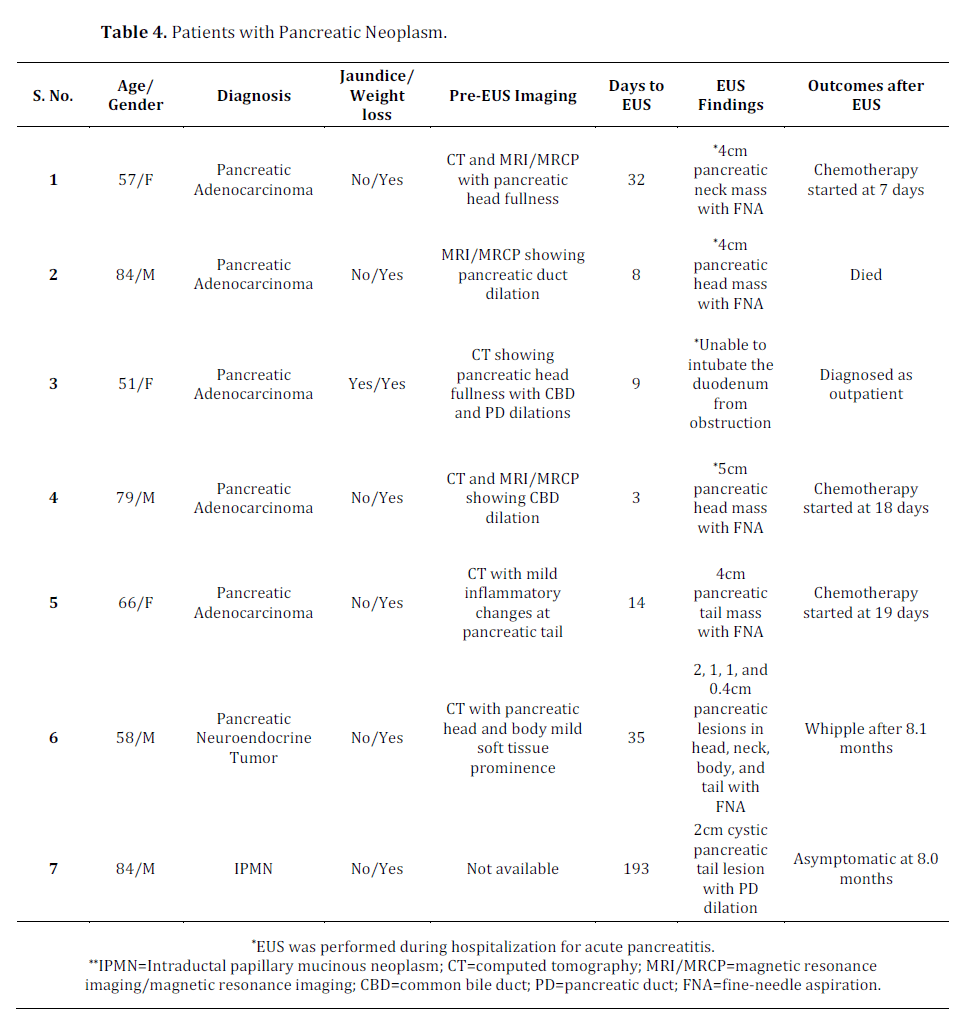
Diagnosis of Pancreatic Neoplasm
Among the 7 patients diagnosed with pancreatic
neoplasm, 6 were diagnosed at the time of EUS. However, one patient was later diagnosed with pancreatic
adenocarcinoma after receiving an incomplete EUS
examination performed during the hospitalization for
acute pancreatitis. Of the 5 patients diagnosed with
pancreatic adenocarcinoma, 3 received chemotherapy
for pancreatic adenocarcinoma 1 died, and 1 was lost to
follow-up. One patient received curative resection for
pancreatic neuroendocrine tumour (Table 4).
DISCUSSION
In a single centre study of 61 hospitalized patients with
acute pancreatitis, 38 (62%) did not have a cause of acute
pancreatitis and 29 (48%) had focal pancreatic lesions
identified on cross-sectional imaging prior to receiving
EUS. EUS was performed at a mean of 2 months earlier
(mean difference=61.2 days, 95%CI 33.0-89.4) during
hospitalization in 29 (47%) compared to 32 (53%) patients
who underwent EUS after hospitalization. Of the patients
receiving EUS during hospitalization, FNA was performed
in 14 (50%) and a new cause of acute pancreatitis
was identified in 4 (pancreatic adenocarcinoma in 3,
choledocholithiasis in 1). No difference in diagnostic yield,
proportion of incomplete procedure, or adverse events
was observed among patients receiving EUS during or
after hospitalization. Among patients who received EUS
during hospitalization, 2 (7%) developed recurrent acute
pancreatitis, and one was later diagnosed with pancreatic
adenocarcinoma after an incomplete index exam.
American Society for Gastrointestinal Endoscopy
guidelines recommend EUS for evaluation of idiopathic
acute pancreatitis in patients >40 years of age when
clinical symptoms, biochemical testing, and crosssectional
abdominal imaging are unrevealing [4]. The
recommendation is based on the rationale that 20% of
such patients will develop recurrent acute pancreatitis,
and clarifying the etiology may potentially prevent a
future attack [1]. Furthermore, acute pancreatitis is the
initial presentation in 5% of patients with pancreatic
adenocarcinoma, associated with a small window of
opportunity for curative resection [13]. In a systematic
review, EUS identified a cause or associated pathology
in 1,096 (62%) of 1,850 patients with idiopathic acute
pancreatitis [14]. Furthermore, EUS demonstrated higher
diagnostic accuracy (64% vs. 34%, P<0.001) compared to MRCP in a systematic review of 477 patients with idiopathic
acute pancreatitis [15]. Although the diagnostic yield is
high, the optimal timing to perform EUS in the setting of
acute pancreatitis remains unclear. During the acute phase
of acute pancreatitis, anatomic derangements including
duodenal wall edema, peri-pancreatic fluid collections,
or pancreatic necrosis may interfere with deep duodenal
intubation of the echoendoscope, precluding complete
visualization of the pancreas or the bile duct. Furthermore,
diffuse hypoechoic changes from edematous pancreatic
parenchyma may obscure visualization of pancreatic
duct changes or occult lesions [6]. Finally, performing
a EUS prior to clinical resolution of acute pancreatitis in
patients who are generally treated with potent analgesics,
may impact the ability to achieve adequate sedation or
increase the risk of adverse events. Subsequently, some
experts have advocated delaying EUS for >4-8 weeks after
presentation of acute pancreatitis [2, 5, 6]
In our study, EUS was performed relatively early
at a median of 23 days from presentation in patients
with mostly mild pancreatitis (median BISAP=1). Focal
pancreatic lesions were observed in a high proportion of
patients on cross-sectional imaging likely given typical
findings associated with acute pancreatitis and high
prevalence of chronic pancreatitis (consistent or suggestive
of chronic pancreatitis in 12 (20%)) in this population.
Performing EUS identified a new cause in 15 (24%) of
61 patients including 6 (10%) with pancreatic neoplasm.
More importantly, the diagnostic yield, proportion with
incomplete procedures, or need for repeat procedure was
similar between patients who received EUS during and
after hospitalization. Furthermore, no procedure-related
adverse events were documented despite half the patients
receiving EUS with FNA during hospitalization for acute
pancreatitis. However, EUS failed to diagnose pancreatic
adenocarcinoma in one patient after an incomplete
procedure due to duodenal obstruction. Interestingly,
prior cross-sectional imaging with CT and/or MRI failed
to demonstrate an obvious mass in all patients with
pancreatic neoplasm, although non-specific changes
were commonly observed (pancreatic head fullness in 2,
bile duct changes in 2, pancreatic duct changes in 2, and
pancreatic head soft tissue prominence in 1). In a study of
107 patients receiving EUS for non-specific abnormalities of the pancreas on CT (i.e. enlarged pancreas, fullness of
the pancreas, abnormal pancreas, prominent pancreas,
or ill-defined pancreas), 29 (27%) were diagnosed with
pancreatic neoplasm, including 22 (21%) with pancreatic
adenocarcinoma [14, 15, 16].
Previous studies examined variable time to performing
EUS in patients with acute pancreatitis. In a prospective
study of 71 patients with acute biliary pancreatitis,
EUS performed <48 hours from presentation identified
choledocholithiasis in 31 (44%) with complete evaluation
in all patients [17]. However, the study excluded 110
patients with severe acute pancreatitis, concurrent
cholangitis, clinical instability, or other possible causes
of acute pancreatitis including 5 (3%) with pancreatic
neoplasm. In another prospective study of 65 patients, EUS
performed <48 hours from the time of hospitalization for
acute pancreatitis following a negative CT, demonstrated
choledocholithiasis in 23 (35%) patients and pancreatic
adenocarcinoma in one (2%) [7]. In 31 patients receiving
EUS performed >2-3 weeks after hospitalization, 8 (26%)
received a new diagnosis including 1 (3%) with pancreatic
adenocarcinoma [17]. In 370 patients with acute
pancreatitis receiving EUS>4 weeks after hospitalization,
108 (29%) had a new diagnosis including 3 (1%) with
pancreatic neoplasm [18]. In a prospective study of 201
patients with acute pancreatitis, EUS performed >1 month
from hospitalization demonstrated a cause in 90 (45%)
but none with pancreatic neoplasm [5]. Furthermore,
recurrent acute pancreatitis occurred in 46 (33%) of
139 and 17 (28%) of 60 patients with or without a cause
identified on EUS [5]. Finally in a study of 40 patients
who received EUS >1 month after the episode of acute
pancreatitis without abdominal pain, a biliary source was
identified in 20 (50%) patients and one (3%) with occult
pancreatic neoplasm [19]. Our study demonstrated the
highest reported prevalence of pancreatic neoplasm as
a cause of acute pancreatitis of 11% compared to other
studies (0-3%), which is likely reflective of institutional
EUS practice patterns and analysing unselected patients
who received EUS regardless of hospitalization status [5, 17, 18, 19, 20]
Our findings have clinical implications. In patients
receiving EUS after acute pancreatitis, nearly half the
patients had focal pancreatic lesions and more than a
tenth were found to have a time-sensitive diagnosis,
including pancreatic adenocarcinoma. Cross-sectional
imaging in this population may commonly identify benign
focal lesions that raise concerns for malignancy but also
fail to identify occult pancreatic neoplasm as a cause of
acute pancreatitis. Furthermore, an incomplete procedure
was infrequent, while procedure-related adverse events
were not documented in patients who received EUS
during hospitalization for acute pancreatitis. Therefore,
performing EUS during the hospitalization may lead to
rapid diagnosis and reduce the risk of lost to follow-up in
patients with potential diagnosis of pancreatic neoplasm.
Finally, one patient with pancreatic adenocarcinoma was
missed after having an incomplete EUS examination. If the index EUS is non-diagnostic or incomplete, a repeat EUS
should be performed as soon as possible in patients with
high suspicion for pancreatic neoplasm based on clinical
features (i.e. jaundice or weight loss) or radiographic
findings (e.g. presence of focal lesions or changes in bile or
pancreatic duct).
There are several limitations of our study. Given the
retrospective study design, patients selected to receive
EUS in our study are likely reflective of local physician
and institutional practice patterns, and the results may
be less generalizable to other settings. For example, a
proportion of patients in our study with a possible cause of
acute pancreatitis after standard evaluation received EUS
given suspicion for alternative cause of acute pancreatitis,
inability to receive contrast-enhanced cross-sectional
imaging, or follow-up evaluation for abnormal findings
detected on cross-sectional imaging. Furthermore, despite
telephone follow-up, complete follow-up was not available
in all the patients.
CONCLUSION
In summary, nearly half the patients with acute
pancreatitis had focal pancreatic lesions detected on
cross-sectional imaging and a tenth were diagnosed with
pancreatic neoplasms. EUS performed in acute pancreatitis
during hospitalization led to a more rapid diagnosis of
pancreatic neoplasm without differences in diagnostic
yield compared to those performed after hospitalization.
Incomplete procedures were infrequent, and procedural
complications were not observed. In patients with acute
pancreatitis with high suspicion for underlying neoplasm,
EUS performed during the hospitalization may lead to a more
rapid diagnosis, without increased risk of adverse events.
Conflicts of Interest
No competing or conflicting interests to declare.
References
- Yadav D, O'Connell M, Papachristou GI. Natural History Following the First Attack of Acute Pancreatitis. Am J Gastroenterol 2012; 107:1096-1103. [PMID: 22613906]
- Vila JJ. Endoscopic ultrasonography and idiopathic acute pancreatitis. World J Gastrointest Endosc 2010; 2:107-111. [PMID: 21160725]
- Somani P, Sunkara T, Sharma M. Role of endoscopic ultrasound in idiopathic pancreatitis. World J Gastroenterol 2017; 23:6952-6961. [PMID: 29097868]
- Chandrasekhara V, Chathadi KV, Acosta RD, Decker GA, Early DS, Eloubeidi MA, et al. The role of endoscopy in benign pancreatic disease. Gastrointest Endosc 2015; 82:203-214. [PMID: 26077456]
- Wilcox CM, Seay T, Kim H, Varadarajulu S. Prospective Endoscopic Ultrasound-Based Approach to the Evaluation of Idiopathic Pancreatitis: Causes, Response to Therapy, and Long-term Outcome. Am J Gastroenterol 2016; 111:1339-1348. [PMID: 27325219]
- Thevenot A, Bournet B, Otal P, Canevet G, Moreau J, Buscail L. Endoscopic ultrasound and magnetic resonance cholangiopancreatography in patients with idiopathic acute pancreatitis. Dig Dis Sci 2013; 58:2361-2368. [PMID: 23508982]
- Kim DB, Paik CN, Song DS, Kim HA, Kim YJ, Lee JM, et al. The Role of Endoscopic Ultrasonography and Magnetic Resonance Cholangiopancreatography in Patients with Acute Pancreatitis after Negative Computed Tomography Findings of the Etiology. Pancreas 2018; 47:1165-171. [PMID: 30142119]
- Anderloni A, Galeazzi M, Ballarè M, Pagliarulo M, Orsello M, Piano MD, et al. Early endoscopic ultrasonography in acute biliary pancreatitis: A prospective pilot study. World J Gastroenterol 2015; 21:10427-10434. [PMID: 26420969]
- Tenner S, Baillie J, DeWitt J, Vege SS, American College of Gastroenterology. American College of Gastroenterology Guideline: Management of Acute Pancreatitis. Am J Gastroenterol 2013; 108: 1400-1415. [PMID: 23896955]
- Papachristou GI, Muddana V, Yadav D, O'Connell M, Sanders MK, Slivka A, et al. Comparison of BISAP, Ranson's, APACHE-II, and CTSI scores in predicting organ failure, complications, and mortality in acute pancreatitis. Am J Gastroenterol 2010; 105:435-441. [PMID: 19861954]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG, et al. Classification of Acute pancreatitis--2012: Revision of the Atlanta Classification and Definitions by International Consensus. Gut 2013; 62:102-111. [PMID: 23100216]
- Catalano MF, Sahai A, Levy M, Romagnuolo J, Wiersema M, Brugge W, et al. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointest Endosc 2009; 69:1251-1261. [PMID: 19243769]
- Munigala S, Kanwal F, Xian H, Scherrer JF, Agarwal B. Increased risk of pancreatic adenocarcinoma after acute pancreatitis. Clin Gastroenterol Hepatol 2014; 12:1143-1150. [PMID: 24440214]
- Pereira R, Eslick G, Cox M. Endoscopic Ultrasound for Routine Assessment in Idiopathic Acute Pancreatitis. J Gastrointest Surg 2019; 23:1694-1700. [PMID: 31197695]
- Wan J, Ouyang Y, Yu C, Yang X, Xia L, Lu N. Comparison of EUS with MRCP in idiopathic acute pancreatitis: a systematic review and meta-analysis. Gastrointest Endosc 2018; 87:1180-1188. [PMID: 29225082]
- Singh S, Reddymasu S, Waheed S, Vail M, He J, Talapaneni J, et al. Endoscopic Ultrasonography Findings in Patients with Non-Specific Changes of the Pancreas on Computed Tomography: A Single-Center Experience. Dig Dis Sci 2008; 53:2799-2804. [PMID: 18320316]
- Anderloni A, Galeazzi M, Ballarè M, Pagliarulo M, Orsello M, Piano MD, et al. Early endoscopic ultrasonography in acute biliary pancreatitis: A prospective pilot study. World J Gastroenterol 2015; 21:10427-10434. [PMID: 26420969]
- Tandon M, Topazian M. Endoscopic ultrasound in idiopathic acute pancreatitis. Am J Gastroenterol 2001; 96:705-709. [PMID: 11280538]
- Yusoff IF, Raymond G, Sahai AV. A prospective comparison of the yield of EUS in primary vs. recurrent idiopathic acute pancreatitis. Ann Gastroenterol 2012; 25:133-137. [PMID: 15557941]
- Rana SS, Bhasin DK, Rao C, Singh K. Role of endoscopic ultrasound in idiopathic acute pancreatitis with negative ultrasound, computed tomography, and magnetic resonance cholangiopancreatography. Ann Gastroenterol 2012; 25:133-137. [PMID: 24714266]

