Keywords
Diabetes Mellitus, Type 1; Diabetes Mellitus, Type 2; Metformin; Pancreatic Neoplasms
Abbreviations
GPCR: G protein-coupled receptor; ASCO: American Society of Clinical Oncology
Introduction
Pancreatic cancer carries a poor prognosis. It is the fourth leading cause of cancer death in men and fifth leading cause of cancer death in women in the United States [1]. The overall five-year survival remains low. Surgical resection is the only chance at cure; however, majority of the patients present with unresectable disease. Additionally, the five-year survival rate of patients who even undergo pancreatectomy remains low. In one study based on a National Cancer database from 1985 to 1995, five-year survival of patients who underwent pancreatectomy alone was 32.8%, 24.8% for those with pancreatectomy followed by radiation and chemotherapy, and less than 9% for those treated without pancreatectomy [2].
Risk factors that have been associated with pancreatic cancer include family history, smoking, chronic pancreatitis and diabetes mellitus [1]. Previous studies have revealed a positive association between diabetes and pancreatic malignancy, but the causal relationship has not been clearly established. The pathogenesis from diabetes to development of pancreatic cancer is also unknown. The causal relationship is controversial because previous studies revealed diabetes to be present in 60% to 81% of the pancreatic cancer patients and many patients have new onset diabetes [3, 4, 5]. This is supported by one study that showed new onset diabetes to be 52.3% of pancreatic cancer patients when comparing to controls of 23.6% (P<0.0001) [6]. In another study, 40.2% of patients were diagnosed with diabetes at time of diagnosis of pancreatic cancer while 15.9% of patients were diagnosed within two years prior [7]. Additionally, pancreatectomy has been shown to resolve some patients’ new onset diabetes and glucose intolerance. Thus, the diabetes appeared to be more of a clinical manifestation of the malignancy itself rather than a direct causal relationship.
What We Knew Before the 2011 American Society of Clinical Oncology (ASCO) Annual Meeting
Diabetes and Pancreatic Cancer: A Causal Relationship?
In 1994, the Italian Pancreatic Cancer Study Group had performed a case control study, where they studied 720 patients with pancreatic cancer and 720 patients as controls [8]. They had discovered a three-fold risk of pancreatic malignancy in diabetic patients (odds ratio: 3.04; 95% CI: 2.21-4.17) [8]. However, when they repeated the analysis to include only patients with diabetes for more than 3 years, there was no statistical significance (odds ratio: 1.43; 95% CI: 0.98-2.07). They then further pursued similar analysis in patients with diabetes for more than 10 and 15 years and discovered no statistically significant associations. Additionally, they also reported that 40.2% of patients with pancreatic cancer and diabetes were diagnosed concomitantly or 15.9% were diagnosed within two years prior to diagnosis of cancer. Thus, they concluded that increased prevalence of diabetes in pancreatic cancer patients was likely related to the diabetes caused by the tumor.
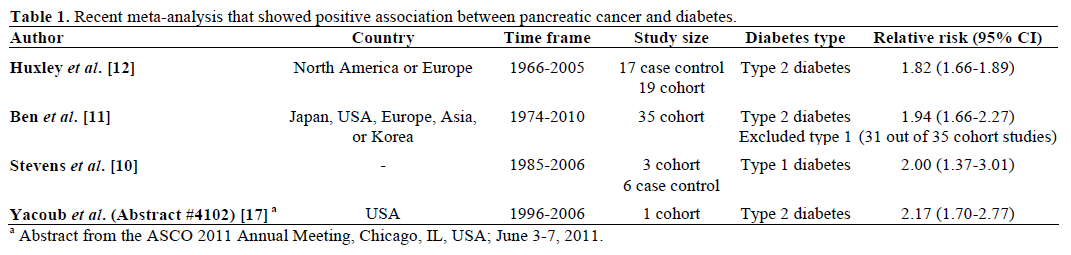
However, repeated studies have confirmed an increased risk, and one study even confirmed an increased risk in patients with longstanding diabetes. In 1995, Everhart and Wright showed from a meta-analysis that in patients with more than five years of diabetes, the pooled relative risk remained at 2.0 (95% CI: 1.2-3.2) [9]. In that study, the relative risk of pancreatic malignancy, irrespective of the duration of diabetes, is 2.1 (95% CI: 1.6-2.8) [9]. Other meta-analysis studies have also reported a similar two-fold risk of pancreatic malignancy in diabetic patients (Table 1) [10, 11, 12]. One meta-analysis study revealed even a two-fold risk in type 1 diabetes patients (Table 1) [10]. In that study, type 1 diabetes was defined as young onset diabetes, diagnosed less than 30 years old or insulin dependent diabetes [10].
Many of the cohort and case control studies that showed a positive association between diabetes and pancreatic malignancy used self-reported diabetes as inclusion criteria rather than clinical data. A Korean ten-year prospective study investigated serum fasting glucose and its associations with malignancy [13]. In this study, the overall risk of malignancy was higher in the group with fasting serum glucose greater than 140 mg/dL than those with fasting serum glucose less than 90 mg/dL, and the association was strongest in pancreatic cancer [13]. The hazard ratio was 1.91 (95% CI: 1.52-2.41) in men and 2.05 (95% CI: 1.43-2.93) in women with fasting serum glucose greater than 140 mg/dL [13]. They also investigated duration of diabetes and associated pancreatic risk, and discovered consistent associations in only men. The hazard ratio was 2.0 (95% CI: 1.2-3.3), 2.4 (95% CI: 1.4-4.3), and 3.0 (95% CI: 1.8-5.0) for men with diabetes duration of less than 4.9 years, 5.0 to 9.9 years, and more than 10 years, respectively. Therefore, in men, the risk of pancreatic cancer increased with longer duration of diabetes.
Metformin Decreases Risk of Pancreatic Malignancy
Based on the positive association between hyperinsulinemia, diabetes and pancreatic cancer, researchers are currently investigating associations between metformin and pancreatic malignancy. Metformin decreases hyperglycemia by inhibiting hepatic gluconeogenesis and enhancing peripheral insulin sensitivity. It allows for increased glucose uptake in skeletal and adipose tissues. It improves insulin binding to insulin receptors [14]. In one study, hyperinsulinemia created by feeding hamsters with high fat diet normalized when the hamsters were treated with two weeks of metformin [15]. In that study, hamsters fed high fat diet and metformin had lower numbers of pancreatic carcinoma, proliferative lesions, pre-neoplastic lesions than hamsters who were fed high fat diet alone [15]. The implications are further supported by a clinical study. In a Taiwanese cohort study, metformin users had decreased risk of pancreatic malignancy with hazard ratio of 0.15 (95% CI: 0.03-0.79) [16].
What We Learned at ASCO 2011 Annual Meeting
Evidence Supporting the Increased Risk of Pancreatic Malignancy in Diabetes Patients
Yacoub et al. (Abstract #4102) [17] conducted a retrospective cohort study based on the health-care database maintained by the Veterans Integrated Services Network 16 (VISN16), consisting of 10 Veterans Health Administration hospitals in South- Central USA. They studied patients from 1996 to 2006, comparing 110,919 diabetic patients to 211,695 nondiabetic patients. One-hundred and twenty-four (0.112%) patients in diabetic cohort and 140 (0.066%) in non-diabetic cohort developed pancreatic malignancy. Using stratified Cox regression, the hazard ratio for incidence of pancreatic cancer was 2.17 (95% CI: 1.70-2.77) when comparing the diabetic cohort to non-diabetic cohort (Table 1). This relative risk is similar to the risk described in other studies in Table 1.
Evidence Supporting Positive Benefit of Metformin in Pancreatic Cancer Patients with Diabetes
Sadeghi et al. (Abstract #4063) [18] performed a retrospective cohort study to investigate the survival benefit of metformin in patients with diabetes and pancreatic malignancy. The data was obtained from the MD Anderson Cancer Center (MDACC) from 2000 to 2009, with additional cases taken from tumor board registry at MDACC. A total of 302 patients were studied. Multivariate Cox proportional hazard regression model was used to determine the effects of metformin on survival in such patients. They report the median survival to be longer in metformin users when compared to non-users: 16.6 vs. 11.5 months (P=0.0044). They also report a 33% decrease risk of death in patients who used metformin compared to those who did not, with hazard ratio of 0.67 (95% CI: 0.51-0.88; P=0.005). Overall, patients who had smaller and resected tumor, lower surgical stage, negative surgical margins, low serum CA 19-9, and metformin use had longer survival. With adjustment for insulin usage or other clinical predictors, the hazard ratio remained significant.
Discussion
The causal relationship between diabetes and pancreatic cancer is controversial. In 1994, the Italian Pancreatic Cancer Group showed that with longer duration of diabetes, the association between diabetes and pancreatic cancer was not statistically significant. However, in a subsequent study in 1995, the relative risk of pancreatic cancer in patients with diabetes for more than five years remained 2.0. In various metaanalysis studies, the pooled relative risk is also approximately two-fold risk. Abstract #4102 presented at the 2011 ASCO Annual Meeting [17] further supports this two-fold increased risk. Although many of the patients with pancreatic cancer have new onset diabetes, there have been studies that still show a positive association even in patients with longstanding diabetes. Thus, it seems likely that diabetes is a risk factor for pancreatic malignancy. The exact pathogenesis would need to be further delineated.
Based on the positive association between hyperinsulinemia, diabetes and pancreatic cancer, therapeutic targets aimed to treat diabetes should decrease risk of pancreatic malignancy. In an aforementioned cohort study, metformin users do have a decreased risk of pancreatic malignancy [16]. In the Abstract #4063 presented at the 2011 ASCO Annual Meeting [18], patients with pancreatic cancer, diabetes, and metformin use had longer median survival and decreased risk of death. This implies that metformin may have some beneficial effects on slowing the progression of pancreatic malignancy. However, specific pathogenesis is unclear and would have to be further explored. There have been mice models revealing of metformin to significantly decrease the growth of pancreatic cancer cells xenografted into the flank of nude mice [19]. In that study, the authors propose that metformin interrupts the G proteincoupled receptor (GPCR), insulin receptor signaling by down-regulating the mTOR pathway [19]. The GPCR and insulin receptor pathways are associated with increased DNA synthesis and pancreatic cancer cell growth [19]. By negatively regulating GPCR and insulin receptor signally, and interrupting their cross talk, metformin is shown to decrease pancreatic cancer cell growth in mice (Figure 1). Translation from basic science research to clinical practice is yet to come. Additionally, in the abstract, the median survival is only prolonged by four months in patients who are metformin users compared to those who are non-users. This is still fairly poor prognosis, and further other treatments that work synergistically with metformin would have to be further explored.
Figure 1. Metformin disrupts G protein-coupled receptor and insulin signaling and pancreatic cancer growth.
Conflict of interest
The authors have no potential conflicts of interest
References
- Krejs GJ. Pancreatic cancer: epidemiology and risk factors. Dig Dis 2010;28(2):355-8.
- Sener SF, Fremgen A, Menck HR, Winchester DP. Pancreatic cancer: a report of treatment and survival trends for 100,313 patients diagnosed from 1985-1995, using the National Cancer Database. J Am CollSurg 1999 Jul;189(1):1-7.
- DiMagno EP. Pancreatic cancer: clinical presentation, pitfalls and early clues. Ann Oncol 1999;10Suppl 4:S140-2.
- Permert J, Larsson J, WestermarkGTet al. Islet amyloid polypeptide in patientswith pancreatic cancer and diabetes. N Engl J Med 1994; 330:313-8.
- Schwarts SS, Zeidler A, Moossa AR et al. A prospective study of glucoseintolerance, insulin, C-peptide, and glucagon in patients with pancreaticcarcinoma. Am J Dig Dis 1978; 23: 1107-14.
- Chari ST, Leibson CL, Rabe KG, et al. Pancreatic cancerassociated diabetes mellitus: prevalence and temporal association with diagnosis of cancer. Gastroenterology 2008;134:95-101.
- Gullo, L. Diabetes and risk of pancreatic cancer. Ann Oncol 1999;10Suppl 4 S79-81.
- Gullo L, Pezzilli R, Morselli-Labate AM. Italian Pancreatic Cancer Study Group: Diabetes and the risk of pancreatic cancer. N Engl J Med 1994; 331:81-4.
- Everhart J, Wright D. Diabetes mellitus as a risk factor for pancreatic cancer. A meta-analysis. JAMA 1995; 273(20):1605-9.
- Stevens RJ, Roddam AW, Beral V. Pancreatic cancer in type 1 and young-onset diabetes: systematic review and meta-analysis. Br J Cancer 2007;96(3):507-509.
- Ben Q, Xu M, Ning X, Liu J, Hong S, Huang W, Zhang H, Li Z. Diabetes mellitus and risk of pancreatic cancer: A meta-analysis of cohort studies. European Journal of Cancer. March 2011; 1-7.
- Huxley R, Ansary-Moghaddam A, Berrington de González A, Barzi F, Woodward M. Type-II diabetes and pancreatic cancer: a meta-analysis of 36 studies. Br J Cancer 2005;92(11):2076-2083.
- Jee SH, Ohrr H, Sull JW, Yun JE, Ji M, Samet JM. Fasting serum glucose level and cancer risk in Korean men and women. JAMA 2005; 293(2):194-202.
- Bailey CJ, Turner RC. Drug therapy: metformin. N Engl J Med 1996; 334:574-9.
- Schneider MB, Matsuzaki H, Haorah J, et al. Prevention of pancreatic cancer induction in hamsters by metformin. Gastroenterology 2001; 120:1263-70.
- Lee MS, Hsu CC, Wahlqvist M, Tsai HN, Chang, YH, Huang YC. Type 2 diabetes increases and metformin reduces total, colorectal, liver, and pancreatic incidences in Taiwanese: A representative population prospective cohort study of 800,000 individuals. BMC Cancer 2011; 11:20: 1-10.
- Yacoub A, Siegel E, Makhoul E. Pancreatic cancer and diabetes mellitus: A retrospective cohort study. J ClinOncol 2011; 29(Suppl.):4102. 18. Sadeghi N, Abbruzzese JL, Yeung SJ, Hassan M, Li D. Effect of metformin on survival of diabetic patients with pancreatic adenocarcinoma. J ClinOncol 2011; 29(Suppl.):4063.
- Sadeghi N, Abbruzzese JL, Yeung SJ, Hassan M, Li D. Effect of metformin on survival of diabetic patients with pancreatic adenocarcinoma. J Clin Oncol 2011; 29(Suppl.):4063.
- Kisfalvi K, Eibl G, Sinnett-Smith J, Rozengurt E. Metformin disrupts crosstalk between G protein-coupled receptor and insulin receptor signaling systems and inhibits pancreatic cancer growth. Cancer Res 2009;69:6539-45.


