Neeraj Awasthy1*,Pratik Raval2 and Mohan Bhargava2
1Department of Pediatric Cardiology and Congenital Heart Diseases, Max Hospital,Saket, Delhi, India
2Department of Cardiology, Max Hospital Saket, Delhi, India
*Corresponding Author:
Neeraj Awasthy
Department of Pediatric Cardiology and
Congenital Heart Diseases, 2nd Floor
East Block, Max Hospital, Saket, New
Delhi-110017, India
Tel: +919811962775
E-mail: n_awasthy@yahoo.com
Received date: July 26, 2017; Accepted date: August 18, 2017; Published date: August 25, 2017
Citation: Awasthy N, Raval P, Bhargava M (2017) Device Closure of a Large Atrial Septal Defect in a Patient with Lung Pathology. Interv Cardiol J. Vol. 3 No. 2:62. doi:10.21767/2471-8157.100062
The incidence of Atrial Septal Defect (ASD) is approximately 3 per 10,000 live births. Ostium secundum ASD is most common type of ASD accounting for 75% of all ASD cases. Patients with irreversible Pulmonary Arterial Hypertension (PAH) are considered ineligible for shunt closure. It is important to ascertain the cause of PAH particularly to rule out pulmonary cause as in present case. A 56-yearold female patient, known case of Ostium secundum ASD presented with NYHA class IV dyspnea and chest infection. A transthoracic echocardiogram revealed 30 mm ASD with bidirectional shunt, dilated Right Atrium (RA), Right Ventricle (RV), severe Tricuspid Regurgitation (TR) (max PG 85 mmHg) and RV dysfunction. She was intubated and put on mechanical ventilator. CT chest showed right lower lobe bronchiectasis with infective changes. However repeated attempts to wean patient off Bipap support were unsuccessful. Subsequently cardiac catheterization and Balloon Occlusion of ASD revealed Qp/Qs ratio of 8:1 with step up in oxygen saturation of 19%. Mean pulmonary artery pressure was 35 mmHg. Later she underwent successful device closure for ASD with AMPLATZER septal occlude (36 mm) (AGA Medical Corp., Minneapolis, MN, USA). Her physical activity and symptoms were much improved. Follow up transthoracic echocardiography after 5 months revealed normal RV contractility and no PAH. While initially chest infection prevented ASD device closure, underlying bronchiectasis which got worsened by ASD shunt, prevented her from weaning off ventilator. ASD device closure thereby helped to reduce pulmonary blood flow and improvement in lung function enabling her to wean off ventilator support.
Keywords
Atrial septal defect; Lung pathology; Bronchiectasis; ASD hemodynamics; Qp/Qs ratio; ASD
Introduction
The incidence of Atrial Septal Defect (ASD) is approximately 3 per 10,000 live births [1]. Ostium secundum ASD is the most common type of ASD accounting for 75% of all ASD cases and 30% to 40% of all congenital heart disease in patients older than 40 years. Minority of patients of ASD (<1%) may develop severe pulmonary hypertension with shunt reversal.
It is a current practice to assess the reversibility of pulmonary arterial hypertension (PAH) by means of pulmonary vasodilator testing during right heart catheterization in patients with shunt related pulmonary hypertension. Patients with irreversible PAH are considered ineligible for shunt closure because of the risk of right ventricular (RV) decompensation after the intervention [2]. It is important to test the reversibility for all cases of ASD with PAH. It is also important to look for other causes of PAH particularly lung pathology. The present case highlights how an underlying lung pathology influences the decision to close the ASD at various stages. We report such case of a lady with PAH who was followed up as Eisenmenger syndrome.
Case Report
A 56-year-old female patient presented with NYHA class IV dyspnea associated with fever and coughing for 7 days. She was managed at local hospital for lower respiratory tract infection and was discharged before 3 days. Although she was diagnosed as a case of congenital heart disease 30 years ago and she was having NYHA class II dyspnea for 10 years, no further evaluation was done. Her symptoms became worse with time, and she presented with NYHA class IV dyspnea. Her blood pressure was 102/66 mmHg, heart rate was 110/min, respiratory rate was 30/min and temperature of 100 F. A regular heart rate was detected with wide fixed splitting of S2 at the pulmonary area. Chest examination revealed bilateral extensive crepitations. She was deeply cyanosed and no clubbing of the fingers or nails was observed. Her oxygen saturation was 46% on room air and 80% on Bipap support with 100% fio2. She had similar episode of LRTI in last one year and was diagnosed as having severe PAH. She was advised medical management in view of severe PAH with cyanosis. Electrocardiography revealed sinus rhythm with right axis deviation. A transthoracic echocardiogram revealed a large ostium secundum ASD (30 mm) with bidirectional shunt (Figures 1a and 1b). The RV was prominently dilated and revealed significantly decreased contractility and flattened interventricular septum with a D-shaped left ventricle (LV) showing normal contractility with RV dysfunction (TAPSE 6 mm). There was no significant RV hypertrophy. The systolic pulmonary arterial pressure measured by maximal tricuspid regurgitation velocity (TR Vmax) was estimated at 85 mmHg with systolic blood pressure of 102 mmHg (TR Vmax=4.6 m/sec).
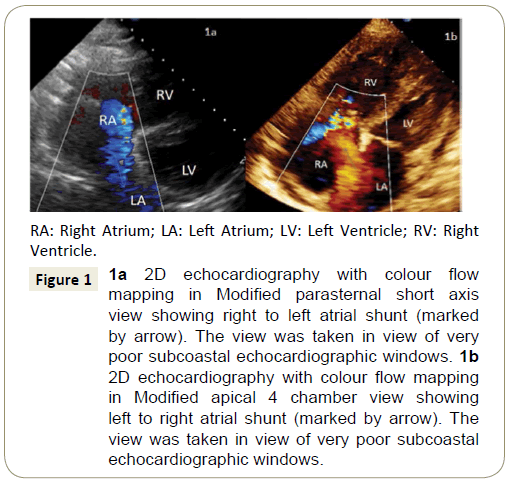
Figure 1: 1a 2D echocardiography with colour flow mapping in Modified parasternal short axis view showing right to left atrial shunt (marked by arrow). The view was taken in view of very poor subcoastal echocardiographic windows. 1b 2D echocardiography with colour flow mapping in Modified apical 4 chamber view showing left to right atrial shunt (marked by arrow). The view was taken in view of very poor subcoastal echocardiographic windows.
In view of severe respiratory distress and desaturation, patient was intubated and put on mechanical ventilator. Her repeat echocardiography showed left to right shunting ASD (Figure 1b) with dilated right atrium and right ventricle with pulmonary artery pressures as estimated from TR velocity of 50 mmHg against systemic pressures of 120/80 mmHg. Chest X-ray showed cardiomegaly and a dilated pulmonary trunk with haziness in bilateral lower zone (Figure 2a). Klebsiella pneumonias was isolated from sputum culture and CT chest showed right lower lobe bronchiectasis with infective changes. She was managed with antibiotics, diuretics, and other supportive measures. She was extubated a week later and was maintaining Spo2 90% to 92% on Bipap support. However repeated attempts to wean patient off Bipap support were unsuccessful. Patient continued to receive supportive care and Ambrisentan.
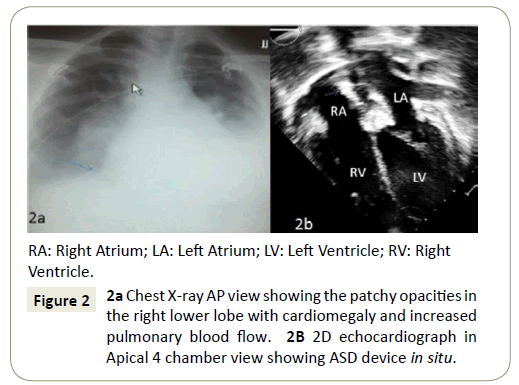
Figure 2: 2a Chest X-ray AP view showing the patchy opacities in the right lower lobe with cardiomegaly and increased pulmonary blood flow. 2B 2D echocardiograph in Apical 4 chamber view showing ASD device in situ.
Subsequently cardiac catheterization and Balloon occlusion of ASD revealed significant shunt with Qp/Qs ratio of 8:1 with step up in oxygen saturation of 19%. Mean pulmonary artery pressure was 35 mmHg (systemic pressure 112/80 mmHg). She underwent device closure for ASD with AMPLATZER septal occluder (36 mm) (AGA Medical Corp., Minneapolis, MN, USA). No residual leak was observed on the follow up transthoracic echocardiography. The patient was given antiplatelet therapy with diuretics. Finally, her physical activity and symptoms were much improved. A chest X-ray showed remarkably decreased pulmonary vascularity, but cardiomegaly remained. Follow up transthoracic echocardiography (Figure 2b) showed ASD device in situ, increased left atrial and LV chamber size. RV size had decreased significantly, and RV contractility was improved in comparison with the initial study. TR Vmax also decreased markedly from 4.6 m/sec to 3.1 m/sec with maximum pressure gradient of 40 mmHg. She is being regularly followed up in OPD and at 3 months of follow up systolic pulmonary arterial pressure was 36 mmHg (measured by maximal tricuspid regurgitation velocity).
Discussion
There have been a lot of questions about safety and efficacy of patients with PAH who undergo surgical or percutaneous ASD closure. Closure of such shunts is associated with decrease of cardiac output and increase of right sided heart failure and death. Thus, defect closure in these patients should be performed only if the benefits of abolishing the shunt outweigh the risks of surgical or percutaneous closure [3,4]. It is important to search for other causes of PAH particularly pulmonary cause.
So, the decision for ASD closure has to be taken keeping in view wholesome approach to the patient including clinical data, echocardiographic findings and cardiac catheterisation data. We had an elderly lady who presented with repeated chest infections. This propensity to chest infection was relatively increased in view of bronchiectatic changes in the lung. Each evaluation at the time of chest infection was suggestive of severe PAH. The decision to close the defect was made after treatment of chest infection. Even after the chest infection subsided, increased blood flow to the other segments of the lung did not allow the patient to be weaned off Bipap support. ASD shunt which would otherwise have been well tolerated became intolerable as this was superimposed on bronchiectasis.
Conclusion
Studies have reported that contributory risk factors including pulmonary vasoconstriction and endothelial dysfunction related to hypoxic state such as chronic lung disease, left ventricular dysfunction and thrombogenic factors have been implicated in and may contribute to, aggravation of long standing shunt related PAH [5-7]. Our patient also had bronchiectatic changes in lung which might have aggravated ASD related PAH. Moreover, high pulmonary blood flow related to ASD might have worsened the lung pathology which led to lower respiratory tract infection and ultimately respiratory failure in our patient. She showed rapid improvement and was successfully weaned off Bipap support after percutaneous ASD closure.
References
- Hossein D, Andrew JB (2012) Percutaneous device closure of secundum atrial septal defect in older adults. Am J Cardiovasc Dis 2: 133-142.
- Schwerzmann M, Zafar M, McLaughlin PR, Chamberlain DW, Webb G, et al. (2006) Atrial septal defect closure in a patient with “irreversible” pulmonary hypertensive arteriopathy. Int J Cardiol 110: 104-117.
- Dimopoulos K, Peset A, Gatzoulis MA (2008) Evaluating operability in adults with congenital heart disease and the role of pretreatment with targeted pulmonary arterial hypertension therapy. Int J Cardiol 129: 163-171.
- Balint OH, Samman A, Haberer K, Tobe L, McLaughlin P, et al. (2008) Outcomes in patients with pulmonary hypertension undergoing percutaneous atrial septal defect closure. Heart 94: 1189-1193.
- Rubin LJ, Baum GL, Crapo JD, Celli BR (2004) Pulmonary heart disease. EDS Textbook of pulmonary diseases. (6th edn). Lippincott-Raven Publishers, Philadelphia, USA. pp. 773-786.
- Rebeiro A, Lindmarker P, Johnsson H, Juhlin DA, Jorfeldt L (1999) Pulmonary embolism. One year follow up with echocardiography doppler and five-year survival analysis. Circulation 99:1325-1330.
- Fedullo PF, Auger WR, Kerr KM, Rubin LJ (2001) Chronic thromboembolic pulmonary hypertension. Review articles. N Engl J Med 345:1465-1472.

