Hafsa Liaqat1, Usama Khalid Choudry2*, Abeer Altaf3, Jibran Mohammad Sauleh4, Syed Ata ur Rahman5, Ammar Khalid Choudry6, Akash Kumar7 and Ghazala Usman8
1Sindh Medical College, DUHS
2Department of Post Graduate Medical Education, Aga Khan University Hospital, Karachi Pakistan.
3Sindh Medical College, DUHS
4Department of Biomedical Sciences, Aga khan University Hospital.
5Sindh Medical College, DUHS
6Jinnah Medical and Dental College, Karachi Pakistan
7Jinnah Medical and Dental College, Karachi
8Department of Community Health Sciences, Jinnah Sindh Medical University
*Corresponding Author:
Usama Khalid Choudry
Department of Post Graduate Education
Aga Khan University Hospital
Karachi, Pakistan.
Tel: +923456165524
E-mail: uk_choudry@hotmail.com
Received date: December 27, 2016; Accepted date: January 30, 2017; Published date: February 06, 2017
Citation: Liaqat H, Choudry UK, Altaf A, et al. Deranged Mental Homeostasis in Medical Students: Evaluation of Depression Anxiety and Stress among Home and Hostel Students. Acta Psychopathol. 2017, 3:1. doi: 10.4172/2469-6676.100074
Copyright: © 2017 Liaqat H, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Medical Students; Dormitories; Family Residence; Depression; Anxiety; Stress
Introduction
Psychological breakdowns and mood disorders are becoming increasingly common among university students generating a lot of concern [1,2]. Depression is a state of low mood and aversion to activity or apathy that can affect a person's thoughts, behaviour, feelings, and sense of well-being [3]. We could therefore refer it as an overall impairment of the personal functioning, with special emphasis on the affective sphere. Recent data has shown that depression is significantly high in medical students [4].
Psychological stress occurs when an individual perceives that environmental demands exceed his or her adaptive capacity [5]. Sometimes stress can be of beneficial value and can elevate ones need to work harder and achieve better results but when the level of mental pressure increases it starts affecting the mood, behaviour and outlook of the person, sleeping and eating habits, hence not just afflicting physical health risks but mental in capacitance as well [6,7].
Anxiety is defined as a chronic condition characterized by an excessive and persistent sense of apprehension with physical manifestations [8]. It can be referred as a subjectively unpleasant feeling of dread over anticipated events [9]. Anxiety has been proved as a major contributor of negative emotional state in medical students [10]. Physical tension can be dealt with a sound overnight sleep but depression, stress and anxiety, if gets chronic, then it can cause major health problems and increase psychological morbidity [4].
Unfortunately depression, stress and anxiety among medical students are usually not only under diagnosed but also not properly attended [11]. This may lead to impairment of their academic achievement, leading to deterioration in relationships [12] thus affecting future employments [13]. Some students deal with stress, depression and anxiety with a positive approach and are less likely to be affected with major psychological disorders, but when stress increases specifically during examinations; it can lead to aggressive episodes or profound social neglects [14]. They might have a low self-esteem; their quality of life may deteriorate. Some may get addicted to drugs and tobacco [15,16]. Some may resort to self-harm and suicidal attempts [17]. In addition to all of this, some recent studies have shown that students living away from their families to get higher dealing with a different alienated environment than their hometown are subjected to a lot of psychological pressures [18].
Aim of this study was to evaluate and compare psychological depression, anxiety and stress among the medical students living with family and those living in dormitory to find out whether psychological state of mind of a student was affected by their residential conditions.
Material and Methods
A comparative cross sectional study was done from July to Dec 2013 including MBBS students from freshman year to final year studying in three medical schools following curriculum of Dow University of Health Science (DUHS) i.e. Sindh Medical College (SMC), Dow Medical College (DMC) and Dow International Medical College (DIMC) Karachi, Pakistan. Ethical approval for the study was obtained from the institutional ethical committee. Sample size was calculated using WHO sample size calculator for the total population of 4000 medical students from 3 medical colleges. 250 students were approached using convenient sampling; confidence level was kept at 95% with confidence interval of 6.0. Students were instructed to fill the questionnaires independently. The purpose of the study was communicated to the students, confidentiality was assured and their participation in the research was voluntary. Informed consent was taken. The first section of questionnaire covered socio-demographic factors such as age, gender, educational details, status of residence, use of recreational drugs and past psychiatric history. The second section comprised of depression, anxiety and stress scale questions (DASS-42). These questions evaluated their somatic symptoms, defence mechanisms and psychological state of mind.
It has been validated as a screening tool by many researchers in a variety of socio demographic conditions [19]. Excluding factors in the study were previous psychiatric history and consistent drug abuse. To minimize the risk of bias due to exam stress the study was conducted during the mid-semester period.
Inclusion criteria
All home and hostel Students enrolled in the study must be MBBS students following DUHS curriculum, participation should be voluntary with no previous psychiatric history or history of any drug abuse.
Exclusion criteria
MBBS students not following DUHS curriculum (to avoid any potential bias), having any significant past psychiatric history or reporting any previous drug abuse were excluded from the study. Students having any recent examination up ahead were also excluded. After exclusion, a total of 211 students were enrolled in the study.
Statistical analysis
Data analysis was done using SPSS 20.0.1. MS excel was used to calculate mean and standard error. Independent samples t-test was used to measure any possible associations, odds ratio were estimated among the two groups.
Results
Over a study period of 6 months, 211 students participated in the study. Out of which 80 (37.9%) were males and 131 (62.1%) were females, the mean age of presentation was 21.052, the mean age for females was 20.984 and 21.162 for males. According to our data the number of students included from first year MBBS were 18 (8%); second year 61 (28.9%); third year 87 (41.23%); fourth year 22 (10.42%) and final year 23 (10.90%). Furthermore students living with family were 122 (57.81%) and those living in dorms were 89 (42.18%). Male students living in home were 24 (19.6%) and dorm students were 98 (80.32%), Female students with home residence were 56 (62.92%) and living in dorms were 33 (37.07%) (Tables 1 and 2).
| Characteristics |
Male |
Female |
All |
| Mean Age ± SD |
21.162±1.64(n=80) |
20.984±1.54
(n=131) |
21.052±1.58
(n=211) |
| Academic year |
| 1st year MBBS |
10 (4.7%) |
08(3.3%) |
18 (8%) |
| 2nd year MBBS |
22(10.42%) |
39(18.48%) |
61 (28.90%) |
| 3rd year MBBS |
26(12.32%) |
61(28.91%) |
87 (41.23%) |
| 4th year MBBS |
13(6.16%) |
09(4.26%) |
22 (10.42%) |
| 5th year MBBS |
09(4.26%) |
14(6.64%) |
23 (10.90%) |
| Residence |
| Home students |
24 (19.6%) |
98 (80.32%) |
122 (57.81%) |
| Hostel Students |
56 (62.92%) |
33 (37.07%) |
89 (42.18%) |
Table 1: Characteristics of study participants.
| Students |
Home Students |
Hostel Students |
Mean |
T Value |
P Value |
Odds
Ratio |
| Normal on Dass 42.0 |
65.07%(n=80) |
57.03% (n=51) |
0-9 |
- |
- |
- |
| Students with Depression |
34.93%(n=42) |
42.70%(n=38) |
8.98 |
-0.507 |
0.612 |
1.41 |
| Normal on Dass 42.0 |
54.91%(n=67) |
56.17%(n=50) |
0-7 |
- |
- |
- |
| Students with Anxiety |
45.09%(n=55) |
43.80%(n=39) |
8.21 |
0.294 |
0.768 |
0.95 |
| Normal on Dass 42.0 |
63.93% (n=78) |
69.66%(n=62) |
0-14 |
- |
- |
- |
| Students with Stress |
30.07%(n=44) |
30.34%(n=27) |
12.02 |
1.194 |
0.233 |
0.77 |
Table 2: Statistical analysis of the study.
To find out the proportion of our medical students amongst two groups suffering from depression, anxiety and stress, we calculated the prevalence in each group. It was 34.42% and 40.4% among home students and dorm students respectively in case of depression, whereas we observed that the prevalence of anxiety among our two groups was 45.08% and 43.82% respectively, while as far as the stress was concerned prevalence among home students was 36.06% and that of dorm students was 30.33%. DASS-42 questionnaire also provided us data regarding the severity of psychological pressures as well which is shown in Figures 1-3.
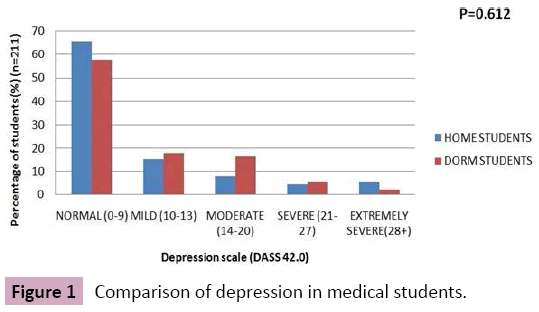
Figure 1: Comparison of depression in medical students.
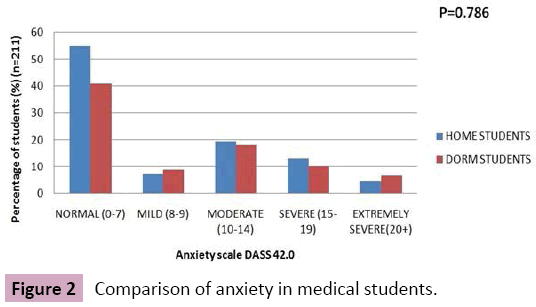
Figure 2: Comparison of anxiety in medical students.
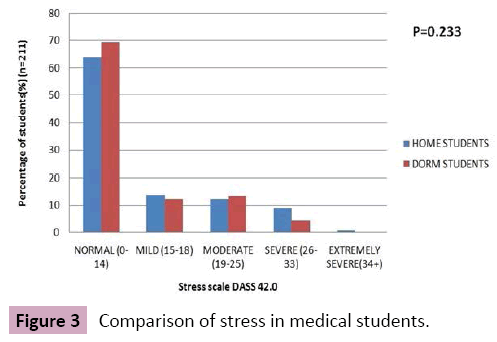
Figure 3: Comparison of stress in medical students.
The mean value of depression as per DASS 42.0 score was 8.98 ± 8.26. Comparison of depression amongst the medical students is given in Figure 1. Our data shows that 80 (65.57%) home students and 51 (57.30%) dorm students were normal on depression scale whereas 19 (15.57%) home students and 16 (17.97%) dorm students had mild depression, regarding moderate depression there were 10 (8.19%) home students and 15 (16.85%) dorm students respectively, 6 (4.91%) home students and 5 (5.61%) dorm students were severely depressed while 7 (5.73%) home students and 2 (2.24%) dorm students suffered from extreme depression on DASS 42.0. The mean value of anxiety was 8.21 ± 6.595. Comparison of anxiety is given in Figure 2. Our data showed that 67 (54.91%) home students and 50 (40.980%) dorm students were normal on anxiety scale whereas 9 (7.37%) home students and 8 (8.988%) dorm students had mild anxiety, we had 24 (19.67%) home students and 16(17.97%) dorm students with moderate anxiety and 16 (13.11%) home students and 9 (10.11%) dorm students with severe anxiety while 6 (4.91%) home students and 6 (6.74%) dorm students suffered from extreme anxiety on DASS 42 scale. The mean value of stress was 12.02 ± 8.206. Comparison of stress amongst the medical students is given in Figure 3. Our data represented that 78 (63.93%) home students and 62 (69.66%) dorm students were normal on stress scale, 17 (13.93%) home students and 11 (12.35%) dorm students had mild stress whereas 15 (12.29%) home students and 12 (13.48%) dorm students were suffering from moderate stress. We had 11 (9.01%) home students and 4 (4.49%) dorm students with severe stress while 1 (0.81%) home students and no dorm students suffered from extreme stress as per DASS 42.0.
Further analysis was done by calculating the odds ratio among both groups. Students living in home were considered the control group while dorm students were taken as the exposed group. The OR value for depression was 1.41, for anxiety OR=0.95 and for stress OR=0.77.
For statistical association among the two groups of medical students under consideration, students test was applied. The two tail significance for depression was 0.612, indicating that depression was not a statistically significant factor for a particular sub-group. Similarly for anxiety and stress the statistical two tail significance according to t test was 0.768 and 0.233 respectively, indicating that anxiety and stress were also not statistically significantly inclined to either sub-group.
Discussion
Adequate psychological health is important for medical students [19]. DASS-42, applied in this research, has the advantage that it can discriminate between the negative emotional symptoms of depression, anxiety, and stress. In our population of medical students the prevalence of depression was considerably high in both groups; this finding was consistent with medical students of Karnataka who had a total prevalence of 71.25% in all students [20]. Another systemic review done in Malaysia stating that the prevalence of depression in Malaysians medical schools is 39% and comparison to that prevalence of depression in Pakistani medical student is 60% which is near to our results, thus the review confirm the strong trend of depression in medical students of Pakistan [21]. Furthermore the prevalence of stress among our two groups of students is relatable with a research done in Putra University Malaysia where the prevalence of psychological stress was as high as 41.9% [22]. The prevalence of anxiety among the two groups corresponded to the study done on the mental health problems on undergraduate students in Public University Malaysia, where anxiety prevalence was 60% [23]. Study done in another Pakistani Medical university denotes prevalence of depression and anxiety of 70% in their medical students which correlates with our study where we had 34.42% depression in home student, 40.8% depression in dorm student respectively and prevalence of anxiety was 45.08% and 43.82% respectively for home and dorm students respectively [6]. Another DASS study contradictory to our study done on students living in dormitories of Tarbiat Modares University showed high levels of anxiety (39.5%) and stress (71.7%) in students living in dormitories however they didn’t have home students as a comparison group [24]. A study done in Aga khan medical University of Pakistan to evaluate coping strategies for stress among Day scholars and hosteliets showed 93.2% day scholars being stressed in their medical school life and 92.1% hosteliets were stressed which is much relatable to our study but they didn’t have depression and anxiety as the constituent to evaluate mental health of students [25]. The mean values for depression; anxiety and stress in our study were in accordance with another cross sectional study done in Davengere, Karnataka which had mean values of 8.88 ± 7.31, 8.29 ± 6.41, 10.46 ± 6.767 for depression, anxiety and stress respectively. It can be inferred from above data that depression and stress might be a subclinical entity at an upper normal limit while the mean level of anxiety has surpassed the basal cutoff value of DASS-42 in our medical students and globally as well.
Additional objective of this study was to perform a detailed comparison of depression, anxiety and stress among the two factions. The fraction of students living with family being extremely depressed was nearly double the number of dorm students depressed as per DASS scale. However the students in severe depression category were nearly equal, moderate level of depression was found to be considerable more in dormitory students i.e., 16.85% as compared to 8.19% home students respectively. While mild depression showed an equivocal prevalence. For anxiety our data showed us that students suffering from extreme anxiety were more abundant in dormitory students i.e. 6.74% as compared to 4.91% home students. Prevalence of moderate and mild anxiety state was almost equal in our both study groups as per the DASS scale.
In our study population, severe stress was considerably higher in home students. Following the similar pattern as was for anxiety scale; students from both the study groups presented with similar numbers having of mild and moderate stress state.
In a nutshell, Our analysis showed that the Odds of having depressive state of mind was more if a medical student was living in a dormitory (OR=1.41) while medical students living with families were prone to be affected by psychological anxiety (OR=0.95) and even more susceptible to psychological stress (OR=0.77). It can be inferred from the above data that depression was found to be relatively high among dorm students, however living in a hostel came out to be a protective exposure considering stress and anxiety in our population. Based on a statistically insignificant P-value it is concluded that negative emotional states were equally distributed among students living with families and in dormitories. Our findings are contradictory to the study done at Allama Iqbal Medical College, Lahore Pakistan [26]. There data showed that the medical students living in dormitory have considerably higher amount of depression and anxiety as compared to students living with families. Another study reported considerable level of stress was found in high density as well as low density dorms [27] but our study showed similar levels of depression, anxiety and stress in home students. This equivocal distribution tells us that probably depression anxiety and stress are associated with a multitude of factors, which might be different or parallel in the two study groups under consideration. Undergraduate medical life predisposes a person to a number of stressors, depressors and anxiety inducers like academic demands, pre-exam preparation, inability to cope up, helplessness, increased psychological pressures, too much work load [25], facing new or sometimes difficult school work, lack of self-esteem, death or loss of loved one(s). [28] Lack of leisure time, material to be learned and frequent academic examinations in a competitive environment predispose the students to depression anxiety and depression [29]. Students living in dormitory might be susceptible to additional stressors like financial issues [26], Adaptation to the new environment, being away from home for the first time, changes in living arrangements [28].
All this can result in decreased life satisfaction among students [30]. Further studies have shown that Stress during medical school can lead to problems later in professional life compromising patient care [31]. Hypothetically it can be said that the life of medical student undergoes a handful of turmoil, capable of affecting his current life as well as his future plans. Considering the fact that a health care worker has to play a substantial role in the society, the adequate care regarding his juvenile training during his years of medical school needs to be addressed and dealt with concern.
Conclusion
The prevalence of depression, anxiety and stress was uniformly high in both home and hostel medical students, yet still, correlation with residential conditions was not established. Depression was more prevalent in dormitory students while anxiety & stress were elevated in home students based on risk estimation. Our study provides an insight regarding a very serious health issue which demands further exploration for development of effective health programs with a more targeted approach for the benefit of young physicians of Pakistan.
Limitations
Our study was limited due to a small sample size and purposive sampling technique. Due to our limited resources we were not able to perform toxicology screens of the students. We used only a single scale to assess depression anxiety and stress, using more than one scale could have minimized response bias.
Recommendations
Based upon our results, we strongly emphasize the need for a study on a larger scale with a prospective design. Targeting the causative factors for such higher rates of depression, anxiety and stress among medical students in Pakistan was beyond the scope of our study, but it is imperative that such a study should be performed.
References
- Voelker R (2007) Campus tragedy prompts closer look at mental health of college students. JAMA 297:2335-2337.
- Sandra S (1997) Depression: questions you have–answers you need. People's Medical Society.
- (2004)Diagnostic and Statistical Manual of Mental Disorders (5thedn.). American Psychiatric Association.
- Aktekin M, Karaman T, Senol YY, Erdem S, Erengin H, et al. (2001) Anxiety, depression and stressful life events among medical students: a prospective study in Antalya, Turkey. Med Educ35: 12-17.
- Refaatl TM (2014) Medical profession strain and cardiovascular disorders: a longitudinal study on a cohort of egyptian physicians.In: Refaatl TM, Ewis AA, Gamall HM, Ahmedz SS, ArafaAE, et al. (eds.) Department of Occupational Medicine, Faculty of Medicine, El-Minia University, El-Minia, Egypt. Life Sci50:7.
- Khan MS, Mahmood S, Badshah A, Ali SU, Jamal Y (2006) Prevalence of depression, anxiety and their associated factors among medical students in Karachi, Pakistan. J Pak Med Assoc56:583
- Rosal MC, Ockene IS, Ockene JK, Barrett SV, Ma Y, et al. (1997) A longitudinal study of students' depression at one medical school. Acad Med 72:542-546.
- Seligman MEP, Walker EF, Rosenhan D (2000) Abnormal psychology (4thedn.). NY, USA: W.W. Norton & Company.
- Gerald CD (2008) Abnormal psychology. Toronto: Veronica Visentin, p: 154.
- Shamsuddin K, Fadzil F, Ismail WS, Shah SA, Omar K, et al. (2013) Correlates of depression, anxiety and stress among Malaysian university students. Asian J Psychiat 6:318-323.
- Tjia J, Givens JL, Shea JA (2005) Factors associated with under treatment of medical student depression. J Am Coll Health 53:219-224.
- Misra R, McKean M (2000) College students' academic stress and its relation to their anxiety, time management, and leisure satisfaction. Am J Health Stud 16:41.
- Eisenberg D, Gollust SE, Golberstein E, Hefner JL (2007) Prevalence and correlates of depression, anxiety, and suicidality among university students. Am J Orthopsychiat77: 534-542.
- Kadison R (2005) Getting an edge-use of stimulants and antidepressants in college. N Engl J Med 353:1089-1091.
- Silver HK, Glicken AD (1990) Medical student abuse: incidence, severity, and significance. JAMA 263:527-532.
- Dyrbye LN, Thomas MR, Shanafelt TD (2005) Medical student distress: causes, consequences, and proposed solutions. Mayo ClinProc80: 1613-1622.
- Frank E, Biola H, Burnett CA (2000) Mortality rates and causes among US physicians.Am J Prev Med 19:155-159.
- Barikani A (2009) Stress in medical students. J Med Educ11: 1-2.
- Lovibond SH, Lovibond PF (1995) Manual for the depression anxiety stress scales: Psychology Foundation(2ndedn.), Sydney.
- Kumar GS, Jain A, Hegde S (2012) Prevalence of depression and its associated factors using beck depression inventory among students of a medical college in Karnataka. Indian J Psychiat54:223.
- Saravanan C, Wilks R (2014) Medical students’ experience of and reaction to stress: the role of depression and anxiety. The Scientific World Journal.
- Yusoff MS, Rahim AF, Baba AA, Ismail SB, Pa MN (2013) Prevalence and associated factors of stress, anxiety and depression among prospective medical students. Asian J Psychiatr6:128-133.
- Latiff LA, Aszahari MA, AbKhalek NF, Fang KJ, Ibrahim N (2014) Prevalence of mental health problems and the associated factors among undergraduate students in a public university, Malaysia. IJPHCS 1:59-69.
- Rezaei AM, Azadi A, Ahmadi F, Vahedian AA (2007) Comparison of depression, anxiety, stress and quality of life in dormitories students of TarbiatModares University. IJNR 2: 31-38
- Shaikh BT, Kahloon A, Kazmi M, Khalid H, Nawaz K, et al. (2004) Students, stress and coping strategies: a case of Pakistani medical school. Educ Health (Abingdon) 17: 346-353.
- Rab F, Mamdou R, Nasir S (2008) Rates of depression and anxiety among female medical students in Pakistan.East Mediterr Health J14:126-133.
- Miller S, Rossbach J, Munson R (1981) Social density and affiliative tendency as determinants of dormitory residential outcomes. J ApplSocPsychol11:356-365.
- Kallingappa PB, Ashokan S (2014) Psychosocial perspective of first year medical students entered in a professional course–a cross sectional study from Davangere, Karnataka. Med Sci 2:110-116.
- Sohail N (2013) Stress and academic performance among medical students. J Coll Physicians Surg Pak 23:67-71.
- Kjeldstadli K, Tyssen R, Finset A, Hem E, Gude T, et al. (2006) Life satisfaction and resilience in medical school–a six-year longitudinal, nationwide and comparative study. BMC Med Educ6:48.
- Tyssen R, Vaglum P, Grønvold NT, Ekeberg Ø (2001) Factors in medical school that predict postgraduate mental health problems in need of treatment: a nationwide and longitudinal study. MedEduc35:110-120.

