Keywords
Depression; Epidemiology; Pancreatic Neoplasms; /physiopathology; Therapeutics
Abbreviations
MAOI: monoamine oxidase inhibitor; SSRI: selective serotonin re-uptake inhibitor
INTRODUCTION
Several studies, dating back as early as the 1930s, have been conducted in order to examine the association between depression and pancreatic cancer [1]. A study in 1967 showed that more than half of patients with pancreatic cancer had psychological symptoms occurring as early as 43 months before physical symptoms [2]. When depression is considered a normal phenomenon in cancer patients, its impact on the quality of life is trivialized. This review studies the literature regarding the association between depression and pancreatic cancer as well the appropriate therapeutic approach.
Incidence
Depression has long been known to have greater incidence in pancreatic cancer patients than in patients with other malignancies. Fras et al. [2] conducted a study based on patients admitted for possible pancreatic or colon cancer and found that 76% of patients with pancreatic cancer had depressive symptoms prior to surgery as compared to 20% of colon cancer patients. A retrospective study comparing patients diagnosed with pancreatic and gastric cancers reached the conclusion that depression was initially present in 14% of patients with pancreatic cancer but in only 4% of stomach cancer patients [3]. In 1986, two prospective studies concerning the incidence of depression in gastrointestinal tract malignancies were conducted. Joffe et al. [4] concluded that 50% of patients who were finally diagnosed with pancreatic cancer met the criteria for the diagnosis of depression while none of the patients that were finally diagnosed with gastric cancer met the criteria. Holland et al. [5] found that patients with pancreatic cancer in advanced stages have more severe depression, anxiety and total mood disturbance as compared to patients with other advanced abdominal neoplasms. In 1993, 52 pancreatic cancer patients were studied, out of which 71% had depressive symptoms and 48% had “anxiety-related” symptoms [6]. According to Massie et al. [7], the prevalence of depression in people with pancreatic cancer ranges from 33% to 50%.
Presentation
Since the 1930s, a triad of symptoms has been described preceding or accompanying the diagnosis of pancreatic cancer of pancreatic cancer: depression, anxiety and a sense of impending doom [1]. Symptoms of clinical depression may include anorexia and weight loss, but there might also be cachexia-related symptoms misattributed to depression [8, 9, 10]. Other common symptoms are negative thoughts and behaviour, sleep disturbances, loss of interest and joy in many aspects of daily life and feeling of hopelessness. Level of fatigue has been found to correlate significantly with depression levels [11, 12]. Symptoms may also include panic, social isolation or even suicidal ideation [13]. Cognitive impairment may be present, a phenomenon called depressive pseudodementia, in which the patient’s results on the Mini Mental State Examination (MMSE) are better than expected [14]. Most studies have been based on newly diagnosed patients, so there is danger of recall bias influencing their psychological status.
Pain should be the first to be assessed and controlled [14]. It has been found that it is a presenting symptom in 80% of pancreatic cancer patients and has occurred at some point of the disease in 90% of patients [15]. Kelsen et al. [16] concluded that increasing pain and depressive symptoms were strongly correlated and that patients awaiting to start chemotherapy had higher levels of measured depression than did patients awaiting surgery.
Diagnosis of Depression in Cancer Patients
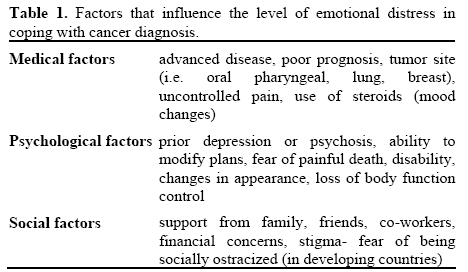
Depression has been found to worsen a patient’s pain and should not be considered “normal” in the terminally-ill [17, 18, 19, 20]. After the diagnosis of cancer, there is usually a process that patients go through in order to cope: initial shock and denial of diagnosis, anxiety and depressive symptoms, impaired cognitive ability, a decreased appetite and a disrupted sleep pattern. In 50% of patients, these symptoms subside within 10 days with family support and treatment that offers hope [14, 19]. The actual level of psychological distress experienced by the patient depends on:
1. medical factors: advanced disease, treatment, pain, physical disability, family history of depression;
2. psychological factors: such as a patient’s coping ability or history of depression. The patient’s perception of cancer and its manifestations is significant, mainly fear of losing control over body functions and of painful death;
3. social factors: whether emotional and financial support from family and friends is available (Table 1) [13, 14, 19].
The physician should be able to recognize when this distress exceeds “normal”. Intervention is needed when depressive symptoms are highly disruptive or when their intensity and duration are greater than expected, provided that these do not qualify for diagnosis of a depressive episode (Diagnostic and Statistical Manual IV) [19]. Major depressive disorder is 4 times more often in cancer patients [13]. While diagnosis of depression in physically healthy patients is based on symptoms like anorexia, weight loss and fatigue, which are common in cancer, psychological or cognitive symptoms of depression (hopelessness, loss of self-esteem, anhedonia, guilt, suicide ideation) are the basis for diagnosing depression in cancer patients [14, 19]. A physician should not be afraid to ask a patient about suicidal ideation out of fear of “giving him the idea”, because, on the contrary, this gives him the chance to talk about his feelings and these thoughts are justified [13, 14]. Some sub-threshold forms of depression, which go undiagnosed and untreated, are often observed in cancer patients. These can be prodromes of major depression, residual symptoms post treatment or a new medical condition altogether [21].
Paraneoplastic Syndrome Depression
Depression may be a manifestation of a more generalized paraneoplastic syndrome, which consists of remote effects of the tumor without direct metastatic activity. Depressive symptoms are found in 58% of paraneoplastic limbic encephalitis cases [22]. Paraneoplastic limbic encephalitis is also characterized by anxiety, irritability, hallucinations, memory loss, seizures, episodes of depersonalization and, sometimes, dementia [22, 23]. It is most common in lung, breast and testis cancer. Paraneoplastic limbic encephalitis’s symptoms usually precede the diagnosis of cancer while the tumor might still be undetectable. Thorough testing must be performed until the malignancy is diagnosed [24]. Diagnosis of paraneoplastic limbic encephalitis requires neuropathological exams or the presence of the four following criteria:
1. compatible clinical presentation;
2. interval of less than 4 years between the development of neurological symptoms and cancer diagnosis;
3. exclusion of other neuro-oncological problems;
4. at least one of the following: cerebrospinal fluid with inflammatory changes but no positive cytology, MRI with temporal lobe abnormalities or EEG with epileptic activity in the temporal lobe [22]. Pathophysiology is believed to be immunological with cancer-induced auto-antibodies attacking the patient’s central nervous system [24].
Pathophysiology
The main question consists of whether pancreatic cancer causes depression or whether depression and its treatments can cause pancreatic cancer. It is believed that the main link between depression and cancer in general is immune dysregulation. In cancer, cytokines are locally produced in the brain and become mediators of neurologic manifestations. They can have a direct effect on brain mechanisms (by altering neuronal processes) or indirect (by altering brain chemistry) [25]. Cytokine dysregulation due to malignancy involves increase of pro-inflammatory cytokines, such as IL-1beta, TNF-alpha, Il-6, IL-18. Studies have shown that, in depressive disturbances, there is a compromised cell-mediated immune function as well as changes in the hypothalamic-pituitary-adrenal axis activity [21]. Increased levels of cytokines in the hypothalamus play a vital role in the cachexia-anorexia syndrome in cancer. Studies on tumor-bearing rodents have shown that peripheral tumor development activates paracrine interactions within the brain. These sustain cytokine production, independently of cytokine concentration in body circulation [25].
On the other hand, it seems possible that depression may increase the risk of subsequent cancer. Depression impairs cell-mediated immunity and the body’s defense against malignancy. Therefore, there seems to be a bidirectional relationship between depression and immunological dysregulation in cancer patients [21]. A meta-analysis based on 13 prospective studies showed a small but increased cancer risk after depression. This result was shown only after reviewing studies with a follow-up of ten years or more. Possible pathophysiological mechanisms are the following:
1. depression indicates physical changes related to the first stages of oncogenesis;
2. depression and cancer are related to common or adjacent genes;
3. greater cancer risk has mainly been proven in breast cancer studies, which can be explained by the fact that depressed women are less likely to have many children;
4. antidepressants have been suggested to be carcinogenic, but more research is necessary to establish this [26].
Some of the confounding factors in the relation between depression and cancer are smoking and alcohol, obesity and family history. These affect a person’s immune system and risk of developing cancer [26, 27].
Review of literature regarding pancreatic cancer showed that nearly 50% of patients with this kind of cancer experience depressive symptoms before diagnosis [6, 27]. This study also showed that diagnosis of depression is made approximately 1.5 years before the pancreatic cancer diagnosis and, therefore, it is unlikely to mask physical symptoms of pancreatic cancer, as symptoms appear only 10 weeks before cancer diagnosis [27]. Many theories have been proposed in order to explain the pathophysiology of depression preceding pancreatic cancer (Figure 1):
1. immunological: pancreatic tumor cells release a protein inducing the production of antibodies that block central nervous system serotonin receptors or antiidiotypic antibodies act as alternate receptors and make serotonin less available in synapses [3, 28, 29];
2. hormonal: urinary excretion of 5-hydroindoleacetic acid (5-HIAA), 5-hydroxytryptophan (5- HTP) or 5-hydroxytryptamine (5-HT:serotonin) has been found in some pancreatic tumors. Increased serotonin secretion depletes serotonin stores and causes depression [28];
3. paraneoplastic: the tumor might produce a false neurotransmitter which alters the patient’s mood and leads to non-suppression of the dexamethazone suppression test [4, 28];
4. biochemical: acid-base abnormalities, anemia, and metabolic abnormalities are possible but they are not present in all patients [6, 28, 30]. It is thought that tumors of the gastro-intestinal tract, which is rich in neuropeptides, may lead to production of biogenic amines that alter the psychological state [5].
Figure 1. Pathophysiology of depression in pancreatic cancer.
Scales for Screening
Several depression scales have been developed for routine screening and for mood change evaluation during treatment, but they are not useful for diagnosis [21, 31]. Such scales are the Beck Depression Inventory [32], the Distress Thermometer [31], the Hospital Anxiety and Depression Scale (HADS) questionnaire [33], the Brief Edinburgh Depression Scale (BEDS) [34], and the Cancer Communication Assessment Tool for Patients and Families (CCAT-PF) scale [35]. By using these tools, physicians are alerted when patients have depressive symptoms, and referral to mental health counseling should be routine occurrence.
Impact of Depression on Survival
Depression has been found to have a significant impact on morbidity in patients with advanced metastatic cancer rendering effective intervention imperative Breast cancer patients with high score of depression have worse survival rates [18] and this has also been shown in patients with hepatobiliary carcinoma [36]. Several reviews have reached the same conclusion for cancer patients in general [37, 38].
Treatment
What must be determined is whether there are underlying organic causes of the depression by conducting thorough physical, endocrinological, neurological and cognitive testing. Causes of organic depressive disorders in cancer patients are:
- metabolic (i.e., hypercalcemia);
- hematologic (i.e., anemia, that should be corrected with recombinant human erythropoietin);
- endocrinologic (i.e., hyperthyroidism, corticosteroid administration);
- infections (i.e., Epstein-Barr virus infection) and antibiotics (i.e., amphotericin);
- nutritional (i.e., vitamin B12 deficiency);
- biologic therapies (i.e., interferon and interleukin);
- whole-brain radiation;
- drug side-effects (i.e., b-adrenergic antagonists, chemotherapeutic agents, such as vinca alkaloids, procarbazine, asparaginase, tamoxifen, intrathecal methotrexate) [14, 19, 21, 39]. Chemotherapy can also cause depression and cognitive deficits after its completion, a phenomenon called “chemobrain”. It consists of impairment of attention, psychomotor functions and memory and is caused by vascular injury, inflammation, neuronal and oxidative damage [40]. In any of the above cases, the organic disorder must be treated first. We often start antidepressant administration concurrently when the treatment is estimated not to suffice, when depression is caused by a drug that cannot be discontinued (i.e., chemotherapeutic drug) or in order to have more rapid results [14]. Administration of various antidepressant drugs is effective but no individual drug has been proven to be relatively more effective than the rest, partly because few studies have been conducted regarding the effectiveness of antidepressants in cancer patients [19, 41].
Choice of antidepressant therapy should rely on:
- the patient’s overall clinical presentation (i.e. hepatic dysfunction);
- cognitive functions;
- other concomitant psychiatric condition;
- main target symptoms in each patient (i.e., insomnia, fatigue);
- family history of psychiatric disorders and previous personal response to antidepressants;
- the need to avoid side-effects caused by antidepressants;
- tolerability by the patient;
- potential interaction with other co-administered drugs; and
- patient’s preference [19, 21, 41].
Pharmacologic Therapy
The treatment can consist of one of the following or a combination (Table 2).
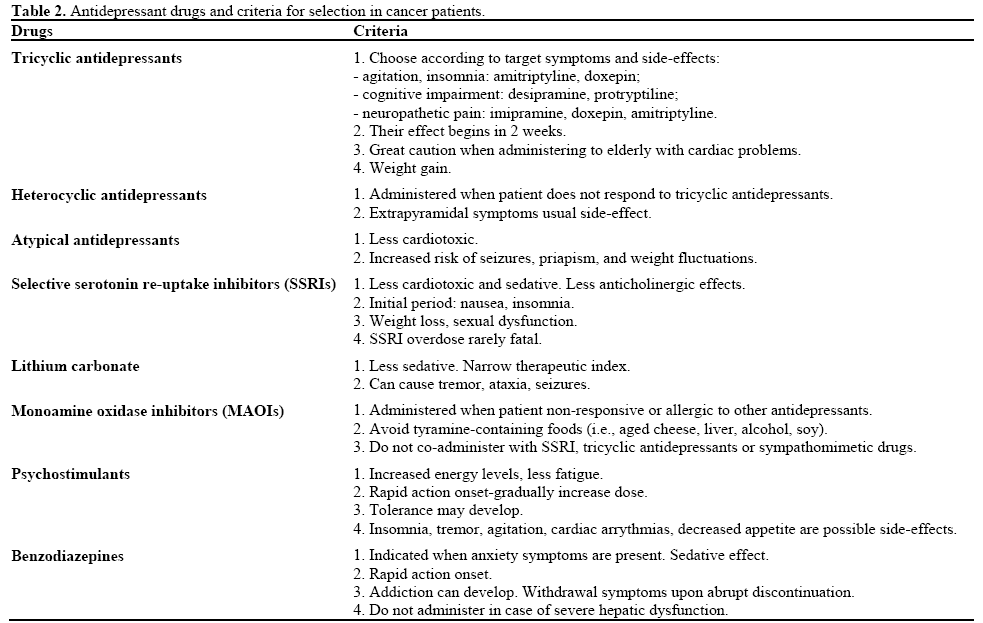
1. Tricyclic antidepressants (i.e., amitriptyline, doxepin, imipramine, nortriptyline, doxapine, protryptyline) are the most commonly used drugs to treat depression in cancer patients in general, and pancreatic cancer in particular. These drugs are initiated at low doses and their doses are slowly increased until adequate response is achieved. It has been noticed that cancer patients show a therapeutic response at much lower doses than usually required but the reason for this remains unknown [14, 19]. The choice of a specific drug of this category is mainly based on the target symptoms and side-effects. If the patient is experiencing agitation and insomnia, a tricyclic antidepressant with sedating effects (i.e., amitriptyline or doxepin) is preferred. If there is psychomotor dysfunction, compounds with less sedating effect are preferred (i.e., protryptyline or desipramine). If there is concomitant neuropathetic pain, then imipramine, doxepin, amitriptyline or desipramine are administered as they have been proven effective in this kind of pain [14, 21, 28]. Nortriptyline is preferred for patients with hepatic dysfunction [19]. If our main concern is to avoid urinary retention and constipation, if there is stomatitis or if drugs with anticholinergic properties are concomitantly used, desipramine or nortriptyline are prescribed, as they have the least anticholinergic effects. If a patient is unable to swallow pills, antidepressant is administered as an elixir (amitriptyline, nortriptyline or doxepin) or by intramuscular route (amitrityline, imipramine) [14, 19]. There are also drugs in this category that can be administered parenterally (amitriptyline, imipramine and clomipramine) in case of absent swallowing reflex, intestinal obstruction or gastric tube. Close monitoring of cardiac conduction is needed when using the parenteral route [14].
2. Heterocyclic antidepressants (i.e., maprotiline, amoxapine). These are prescribed when the patient is not responsive to tricyclic antidepressants or there are serious side-effects. Maprotiline increases the risk of seizures whereas amoxapine can cause extrapyrimidal symptoms if taken with other dopamine blockers, such as antiemetics [14, 19].
3. Atypical antidepressants (i.e., trazodone, buproprion). These are less cardiotoxic than tricyclic antidepressants. Buproprion increases the risk of seizures. Trazodone is strongly sedating and therefore preferred in insomnia but must be administered with great caution in male patients as it can cause priapism [14, 19, 28].
4. Selective serotonin re-uptake inhibitors (SSRIs) (i.e., paroxetine, sertraline, fluoxetine, fluvoxamine, citalopram). These drugs have fewer sedative and autonomic effects than tricyclic antidepressants [14, 19, 28]. Pancreatic tumors have been found to have increased serotonin secretion. This exuberant metabolism decreases the serotonin in the central nervous system thereby resulting in depression [27]. For a brief initial period, SSRIs can cause nausea, headache, somnolence, insomnia, increased anxiety and appetite suppression [14, 19, 28]. There is no evidence of interaction between SSRIs and chemotherapy in inducing nausea [33]. Paroxetine and sertraline have shorter half-life than fluoxetine, which is important in order to avoid drug accumulation [14]. SSRIs are also co-administered with interferon in treatment of melanoma, in order to achieve targeted prevention of depression secondary to interferon, but also because studies have shown that sertraline downregulates the anti-apoptotic Akt molecule. Therefore, they might improve the efficacy of interferon [32, 42].
5. Lithium carbonate. If the cancer patient had bipolar disorder before the diagnosis, lithium should be continued with fluid and electrolyte monitoring. It can be nephrotoxic if co-administered with cisplatin [14].
6. Monoamine oxidase inhibitors (MAOIs) (i.e., phenelzine, isocarboxazid, tranylcypromine). If a patient is already on MAOI with good response, it should be continued. Caution should be exercised in their administration. Tyramine-containing foods should be avoided. If co-administered with narcotic analgesics, there may be myoclonus and delirium, whereas sympathomimetic drugs combined with MAOIs can cause hypertensive crisis [14, 19]. MAOIs have significant interactions with tricyclic antidepressants increasing their concentration [43].
7. Psychostimulants (i.e., methylphenidate, dextroamphetamine). These drugs are energizing, improve attention span, and decrease weakness. They have rapid action onset and counteract sedation caused by narcotic analgesics enhancing their analgesic effect [14, 19, 28]. The dose is gradually increased until adequate response or side-effects appear (nervousness, insomnia, blood pressure increase, dyskinesia, psychosis). Tolerance may develop and in this case dose should be adjusted. Pemoline is available in chewable form and it is absorbed by the buccal mucosa. It is useful in patients with difficulty swallowing or intestinal obstruction but must be avoided in renal impairment [14, 19].
8. It is suggested that when rapid effect is needed, we start with an initial dose of methylphenidate, 2.5 mg orally increased every couple of days up to a maximum dose of 30 mg. When the patient has a greater life span, SSRIs are administered, as they may take up to 4-6 weeks to become effective. They can be given concurrently with psychostimulants that are progressively tapered as antidepressants start to have therapeutic effect [20, 44]. A specialist must be consulted when the patient does not respond after 4-6 weeks of antidepressant therapy or if depression relapses concurrently [33].
9. Benzodiazepines (i.e., diazepam, alprazolam, flurazepam, temazepam, triazolam). They are administered when the patient has anxiety symptoms [14, 28].
10. Electroconvulsive therapy. This kind of therapy is indicated for patients with depression refractory to antidepressant drugs, with suicidal or psychotic features or when antidepressants are contraindicated [14, 19, 21]. Psychotic depression includes delusions, hallucinations or grossly disorganized behavior. In these cases, antipsychotic drugs are co-administered (preferably high potency antipsychotics to minimize risk of delirium and anticholinergic effects) [14, 19].
Psychotherapeutic Treatment, Psychosocial Support, and Role of the Social Worker
When cancer occurs, patients may experience any combination of fear, sadness, anxiety and/or depression. Family members may also experience such feelings. Anger over the reality of a diagnosis, concerns about shifting roles and responsibilities, foreseeable economic burdens and questions about doing what is needed often surface. These feelings may appear at any time in the course of the illness, even after treatment ends. While these feelings may be predictable, there are times when feelings can overwhelm and take control over aspects of daily life. Social workers play an important role in helping the patient and family manage these symptoms, through short-term counseling or cognitive-behavioral stress management therapy. The patient and family should be taught coping strategies, so that he and his relatives can cope more effectively and the feeling of helplessness diminished [13, 19, 33, 41]. The target is to help the patient return to his earlier psychological baseline [19]. Anti-depressants are co-administered, if necessary [45]. It is also important to address the potential need for treatment of family members. It has been shown that survival rates are greater in cancer patients after psychotherapy but other studies have shown no significant improvement [38]. Planning of treatment for psychosocial intervention must take into account factors that determine a patient’s emotional distress, such as individual temperament and family support, as discussed earlier. When faced with a limited prognosis, transition to hospice care should be implemented. These services may take place at home or at a freestanding or in-patient facility. Psychosocial care continues to be provided to both the patient and his/her family. This allows the patient to be reassured that he/she will not die alone or in pain [14, 19, 28] and will assist the family in coping with their grief (Figure 2). Social workers are the key participants throughout the cancer continuum: at time of diagnosis, treatment, relapse, survivorship, end of life, and bereavement. Clinical social workers are uniquely qualified to manage these challenges for the patient and family, as well as address the concrete concerns that may arise, which often result in referrals to community resources. As part of the standard of care, the social worker should be introduced on the initial visit and participate in the discussion that the physician has with the patient and family after examination. This normalizes the role of the social worker and validates the need for subsequent sessions. Although patients and families may not need to consult with the social worker on every visit, it allows for a connection to the social worker and subsequent increased comfort communicating with the social worker when a crisis does occur. One model of care that should be considered is that of continuity of care. The same social worker is able to provide therapeutic intervention regardless of site of care (in-patient, infusion units, diagnostic imaging, etc.) and be a consistent presence throughout the course of illness. The ability to obtain mental health counseling within the medical setting takes into account a patient’s fatigue and allows them to receive comprehensive care in one setting, without necessitating extra appointments, potential rides or other resources. According to the Institute of Medicine (IOM) [46], many providers do not consistently ask about psychosocial issues nor do they provide an adequate link to resources, which has a detrimental impact on patients. It also recommends that all patients with cancer have a psychosocial treatment plan.
Figure 2. Algorithm for treatment of patient with pancreatic cancer
and depression.
Conclusion
Depression in pancreatic cancer is a condition that must be diagnosed and treated, as studies have shown that depression is a detrimental factor in the last stages of life of cancer patients. Treatment for depression has also been shown to impact quality of life and may bring increased comfort during end of life.
Conflict of interest
None
Helsinki declaration
Conformed
References
- Yaskin JD. Nervous symptoms at earliest manifestations of cancer of the pancreas. JAMA 1931; 96:1664-8. [PMID 10390740]
- Fras IL, Litin EM, Pearson JS. Comparison of psychiatric symptoms in carcinoma of the pancreas with those in some other intra-abdominal neoplasms. Am J Psychiatry 1967; 123:1553-62. [PMID 4381627]
- Jacobsson L, Ottosson JO. Initial mental disorders in carcinoma of pancreas and stomach. Acta Psychiatr Scand Suppl 1971; 221:120- 7. [PMID 5286323]
- Joffe RT, Rubinow DR, Denicoff KD, Maher M, Sindelar WF. Depression and carcinoma of the pancreas. Gen Hosp Psychiatry 1986: 8:241-5. [PMID 3744031]
- Holland JC, Korzun AH, Tross S, Silberfarb P, Perry M, Comis R, Oster M. Comparative psychological disturbance in patients with pancreatic and gastric cancer. Am J Psychiatry 1986; 143:982-6. [PMID 3524279]
- Green AI, Austin CP. Psychopathology of pancreatic cancer. A psychobiologic probe. Psychosomatics 1993; 34:208-21. [PMID 8493302]
- Massie MJ. Prevalence of depression in patients with cancer. J Natl Cancer Inst Monogr 2004; 32:57-71. [PMID 15263042]
- Savage C, Butcher W, Noble D. Psychiatric manifestations in pancreatic disease. J Clin Exp Psychopathol 1952; 13:9-16. [PMID 14927728]
- Perlas AP, Faillace LA. Psychiatric manifestations of carcinoma of the pancreas. Am J Psychiatry 1964; 121:182. [PMID 14194218]
- Karliner W. Psychiatric manifestations of cancer of the pancreas. N Y State J Med 1956; 56:2251-2. [PMID 13334839]
- Visser MR, Smets EM. Fatigue, depression and quality of life in cancer patients: how are they related? Support Care Cancer 1998; 6:101-8. [PMID 9540167]
- Hann DM, Denniston MM, Baker F. Measurement of fatigue in cancer patients: further validation of the Fatigue Symptom Inventory. Qual Life Res 2000; 9:847-54. [PMID 11297027]
- Mishra SK, Mohapatra PK, Bhattacharya K, Gupta T, Agarwal JP. Prevalence of psychiatric disorder in asymptomatic or minimally symptomatic cancer patients on treatment. J Cancer Res Ther 2006; 2:136-9. [PMID 17998693]
- Massie MJ, Gagnon P, Holland JC. Depression and suicide in Patients with Cancer. J Pain Symptom Manage 1994; 9:325-40. [PMID 7963785]
- Foley KM. Pain assessment and cancer pain syndromes. In: Doyle D, Hanks GWC, MacDonald N, Eds. Oxford Textbook of Palliative Medicine. 2nd ed Oxford, New York: Oxforfd University Press;1998.
- Kelsen DP, Portenoy RK, Thaler HT, Niedzwiecki D, Passik SD, Tao Y, et al. Pain and depression in patients with newly diagnosed pancreas cancer. J Clin Oncol 1995; 13:748-55. [PMID 7884435]
- Barkwell DP. Ascribed meaning: a critical factor in coping and pain attenuation in patients with cancer-related pain. J Palliat Care 1991; 7:5-14. [PMID 1941361]
- Watson M, Haviland JS, Greer S, Davidson J, Bliss JM. Influence of psychological response on survival in breast cancer: a population-based cohort study. Lancet 1999; 354:1331-6. [PMID 10533861]
- Passik SD, Breitbart WS. Depression in patients with pancreatic carcinoma. Diagnostic and treatment issues. Cancer 1996; 78:615-26. [PMID 8681300]
- Block SD. Perspectives on care at the close of life. Psychological considerations, growth, and transcendence at the end of life: the art of the possible. JAMA 2001; 285:2898-905. [PMID 11401612]
- Spoletini I, Gianni W, Repetto L, Bria P, Caltagirone C, Bossù P, Spalletta G. Depression and cancer: an unexplored and unresolved emergent issue in elderly patients. Crit Rev Oncol Hematol 2008; 65:143-55. [PMID 18068997]
- Cornelius JR, Soloff PH, Miewald BK. Behavioral Manifestations of Paraneoplastic Encephalopathy. Biol Psychiatry 1986; 21:686-90. [PMID 3011132]
- Gultekin SH, Rosenfeld MR, Voltz R, Eichen J, Posner JB, Dalmau J. Paraneoplastic limbic encephalitis: neurological symptoms, immunological findings and tumour association in 50 patients. Brain 2000; 123:1481-94. [PMID 10869059]
- Farrugia ME, Conway R, Simpson DJ, Kurian KM. Paraneoplastic limbic encephalitis. Clin Neurol Neurosurg 2005; 107:128-31. [PMID 15708228]
- Plata-Salamán CR. Central nervous system mechanisms contributing to the cachexia-anorexia syndrome. Nutrition 2000; 16:1009-12. [PMID 11054608]
- Oerlemans ME, van den Akker M, Schuurman AG, Kellen E, Buntinx F. A meta-analysis on depression and subsequent cancer risk. Clin Pract Epidemol Ment Health 2007; 3:29. [PMID 18053168]
- Carney CP, Jones L, Woolson RF, Noyes R Jr, Doebbeling BN. Relationship Between Depression and Pancreatic Cancer in the General Population. Psychosom Med 2003; 65:884-8. [PMID 14508036]
- Shakin EJ, Holland J. Depression and Pancreatic Cancer. J Pain Symptom Manage 1988; 3:194-8. [PMID 3057080]
- Brown JH, Paraskevas F. Cancer and depression. Cancer presenting with depressive illness : an autoimmune disease? Br J Psychiatry 1982; 141:227-32. [PMID 6182940]
- Alter CL. Palliative and Supportive Care of patients With Pancreatic Cancer. Semin Oncol 1996; 23:229-40. [PMID 8623059]
- Tuinman MA, Gazendam-Donofrio SM, Hoekstra-Weebers JE. Screening and referral for psychosocial distress in oncologic practice: use of the Distress Thermometer. Cancer 2008; 113:870-8. [PMID 18618581]
- Greenberg DB. Barriers to the Treatment of Depression in Cancer. J Natl Cancer Inst Monogr 2004; 32:127-35. [PMID 15263054]
- Ballenger JC, Davidson JR, Lecrubier Y, Nutt DJ, Jones RD, Berard RM; International Consensus Group on Depression and Anxiety. Consensus statement on depression, anxiety, and oncology. J Clin Psychiatry 2001; 62 (suppl 8):64-7. [PMID 12108825]
- Lloyd-Williams M, Shiels C, Dowrick C. The development of the Brief Edinburgh Depression Scale (BEDS) to screen for depression in patients with advanced cancer. J Affect Disord 2007; 99:259-64. [PMID 17055588]
- Siminoff LA, Zyzanski SJ, Rose JH, Zhang AY. The Cancer communication Assessment Tool for Patients and Families (CCATPF): a new measure. Psychooncology 2008; 17:1216-24. [PMID 18504807]
- Steel JL, Geller DA, Gamblin TC, Olek MC, Carr BI. Depression, immunity, and survival in patients with hepatobiliary carcinoma. J Clin Oncol 2007; 25:2397-405. [PMID 17557953]
- Angelino AF, Treisman GJ. Major depression and demoralization in cancer patients: diagnostic and treatment considerations. Support Care Cancer 2001; 9:344-9. [PMID 11497387]
- Spiegel D, Giese-Davis J. Depression and cancer mechanisms and disease progression. Biol Psychiatry 2003; 54:269-82. [PMID 12893103]
- el-Kamar FG, Grossbard ML, Kozuch PS. Metastatic pancreatic cancer: emerging strategies in chemotherapy and palliative care. Oncologist 2003; 8:18-34. [PMID 12604729]
- Nelson CJ, Nandy N, Roth AJ. Chemotherapy and cognitive deficits : Mechanisms, findings, and potential interventions. Palliat Support Care 2007; 5:273-80. [PMID 17969831]
- Rodin G, Katz M, Lloyd N, Green E, Mackay JA, Wong RK. Treatment of depression in cancer patients. Curr Oncol 2007; 14:180- 8. [PMID 17938701]
- Reddy KK, Lefkove B, Chen LB, Govindarajan B, Carracedo A, Velasco G, et al. The antidepressant sertraline downregulates Akt and has activity against melanoma cells. Pigment Cell Melanoma Res 2008; 21:451-6. [PMID 18710373]
- Bernard SA, Bruera E. Drug Interactions in Palliative Care. J Clin Oncol 2000; 18:1780-99. [PMID 10764440]
- Ellison NM, Chevlen E, Still CD, Dubagunta S. Supportive care for patients with pancreatic adenocarcinoma: symptom control and nutrition. Hematol Oncol Clin North Am 2002; 16:105-21. [PMID 12063822]
- Roth AJ, Modi R. Psychiatric issues in older cancer patients. Crit Rev Oncol Hematol 2003; 48:185-97. [PMID 14607382]
- Committee on Psychosocial Services to Cancer Patients/Families in a Community Setting, Adler NE, Page AEK. Cancer Care for the Whole Patient: Meeting Psychosocial Health Needs. IOM Report, October 23, 2007.



