Keywords
Obesity; Decision-making; Black women; Food choices; Physical activity
Introduction
The prevalence of obesity among Black1 women is alarming and it takes a toll causing human suffering related to morbidity and mortality. The burden of obesity distresses the equilibrium of the individual, their family and the community. The stresses are physio-psycho-social with diseases such as hypertension, type 2 diabetes mellitus [1], along with depression, loss of selfesteem and social isolation [2]. The graph shown illustrates that Black women have the highest prevalence of obesity at 57% in the US [2,3] (Figure 1).
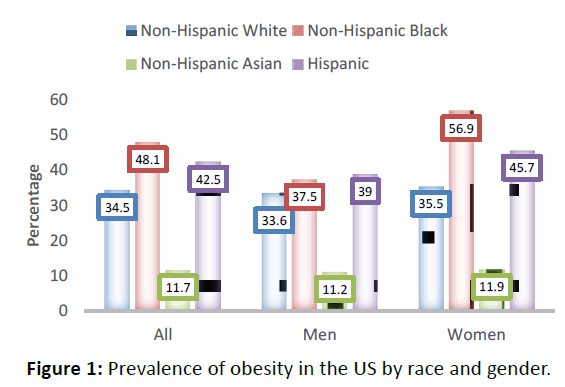
Figure 1: Prevalence of obesity in the US by race and gender.
There is an abundance of information regarding obesity among women, but a unique dimension of this topic remains poorly examined. Specifically, there are gaps in the literature about the decision-making process that Black women use to determine food choices and physical activity. Government data support the need for a better understanding of the underlying mechanisms contributing to the problem of obesity (Figure 1).
The Simplified Model of Decision-Making provides an opportunity to examine factors contributing to decisions, behaviors and outcomes [4,5]. Their model shows how decisions are the result of an interconnection among information, values and preferences.
Conceptual framework
The conceptual framework for this study was the newly created Adapted Model of Decision-Making which was based on Wills and Holmes-Rovner ‘s Simplified Model of Decision Making, [4] adapted from Rothert et al. [5]. The Simplified Model of Decision Making defined the concepts of the decisionmaking process as: 1) Information 2) values, 3) preferences, 4) decision, 5) behavior and 6) outcomes (Figure 2).
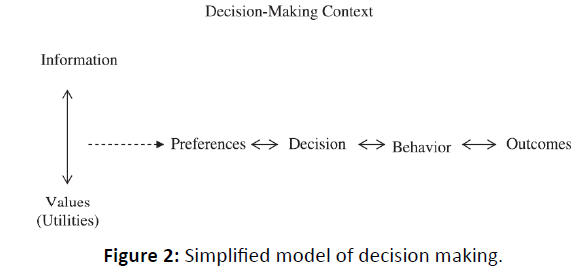
Figure 2: Simplified model of decision making.
The interaction of information and values leads to preferences which influence decisions. Decisions then lead to behaviors that will produce outcomes. Wills and Holmes-Rovner explain that over time, there is a dynamic interaction among these concepts [4,5].
The Adapted Model of Decision-Making, the following concepts: Information, values and preferences interact with an added fourth concept-environment (Figure 3). Placed within the decision-making process circle at the beginning of the model, environment interacts with the other three concepts and provides depth and meaning to the understanding of how decisions are made.
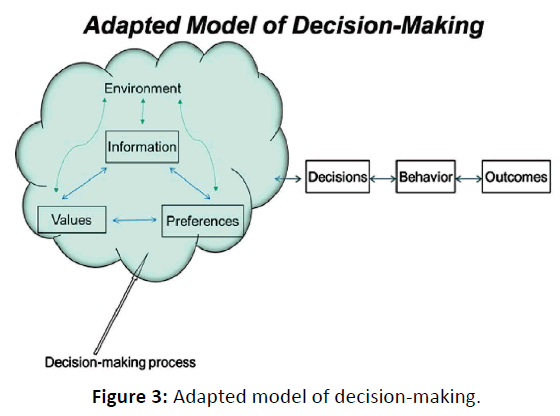
Figure 3: Adapted model of decision-making.
Purpose of the study
This study explores and reports the decision-making process of Black women utilizing the interaction of information, values, preferences and environment in their food choices and physical activity.
Literature Review
The literature suggests information influences decisionmaking, both directly and indirectly [6-8]. In the broadest sense, Citroen found that relevant information supported decisionmaking among business executives. Citroen contends that relevant information helps reduce uncertainty and improves the quality of decision-making. Chen et al. were more specific and studied calorie information and food choices [7]. Based on data from the Behavioral Risk Factor Surveillance System, Chen and colleagues reported that, after the implementation of calorie information on menus in chain restaurants in Kings County, Washington, three times as many customers used the calorie information. To improve consumers’ food choices by providing nutritional information in grocery stores, Nikolova and Inman developed a scoring system. They found that the scoring system helped consumers make healthier food choices. In contrast, Amaro et al. suggested nutritional knowledge is a factor in food choices, but may not be enough to produce behavior change [9]. In fact, they suggested mindfulness, such as awareness, attention and self-regulation are elements of food choice.
In a quantitative study of environment based on the 2002- 2006 NYC Community Health Survey dataset, Viola et al. found a significant negative relationship between supermarket density with being overweight and obesity [10]. In other words, environments with fewer supermarkets had people with higher BMIs. While their study documented the importance of environment, there is still a need to understand the underpinnings of decisions towards food choices based on information, values and preferences.
The literature supports the notion that a person’s preferences are important in weight management, food choice and types of physical activity. Specifically, Auchincloss et al. found that nutritional facts were less of a motivator than taste, preference and price among 36 focus group participants [11]. Taste took priority over knowledge of nutritional information. The authors discussed the barrier to the use of nutritional information resulting from confusing and conflicting information. These investigators did not consider the decision-making process that includes a person’s lived environment and preferences that informs their decision-making process. Therefore, this study will examine the underlying factors contributing to an understanding of the decision-making process about food choices and physical activity among Black women.
Methods
Research design and setting
An exploratory qualitative research design was selected for this study. Focus groups provided the venue for gaining new insights from women to generate knowledge fundamental to understanding decisions about their food choices and physical activity. The study took place in a private childcare center in Brooklyn, New York on Saturday mornings. As part of a larger study, mother and daughter dyads were recruited to:
1. Explore and describe how Black women combine information, values, preferences and environment in their decision-making process concerning food choices and physical activity,
2. Describe the relationship between the resultant decisions, behaviors changes and specific outcomes,
3. Describe the influence that mothers’ decisions and behaviors about food choices and physical activity have on their 6 to 8 years old daughters’ attitudes and behaviors about food choices and physical activity,
4. Provide preliminary data to support theory-based, culturallysensitive and developmentally appropriate interventions to break the cycle of obesity-related behaviors.
This article presents findings from the first two objectives.
Data collection
Following the Institutional Review Board for Protection of Human Subject’s approval of the study, a focused group format was used to collect data. After providing a detailed explanation about the study, women completed an investigator developed characteristic profile which included the following: Income, age, BMI, level of physical activity, perceptions of body weight and healthy eating and weight goals. All focus group sessions were tape-recorded and accurately transcribed. After completing the project, an honorarium was provided to the participants ($25.00).
Unit of analysis
Consistent with focus group analysis, responses from individuals and responses from group interactions were the units of analysis [12]. There was one focus group session with four participants, one focus group session with three participants and one individual interview.
Content Analysis
The analytic strategy utilized for this project included: Coding, comparing and contrasting focus group and individual participant responses to categorize and interpret data. Specifically, responses to questions generated from the Adapted Model of Decision-Making were coded. The codes were then compared across individual and focus group responses to identify recurrent themes within each concept of the model [12]. A holistic approach was maintained and the model guided and provided the context for interpreting the participants’ responses.
Results
Characteristics of the study participants
A total of eight Black women participated in the study. All of the women were employed and chose the ‘$50,000 and above’ income category. The mean age of the women was 39.25 (SD=5.96) years old with a mean BMI of 31.16 kg/ m2 (SD=6.78). Shown in the table below, two women had normal BMIs, two women were overweight and four women were obese. Their perception of their body weight appeared to match their BMIs except for three participants. All but two of the participants had appropriate weight goals. In addition, table 1. summarizes behaviors related to physical activity showing that none of the participants reported their physical activity level as very active. Specifically, when asked to rate their level of physical activity on a scale of 1-5 with 5 being very active, none of the participants selected very active. However, when asked how many days/week they engaged in moderate to vigorous physical activity, two participants reported moderate to vigorous physical activity 5 or more days/week. Participants had the option of selecting from the following four categories: None, 1-2 days/week, 3-4 days/week or 5 or more days/week. Thus, some of the participants were inconsistent in reporting level of physical activity and the number of days/week they were physically active. All the participants had the goal of weight lost, but it was inappropriate for two of the participants (Table 1).
| ID. Label |
Level of Physical Activity |
Days/wk of Physical Activity |
Perception of Body Weight |
BMI |
Age |
`Perception of Healthy Eating |
| A |
Active |
None |
Slightly overweight |
27.4 |
44 |
Slightly healthy |
| S |
Active |
1-2 days |
Slightly overweighta |
33.3 |
39 |
Healthy |
| C |
Active |
1-2 days |
Slightly overweight |
26.6 |
38 |
Slightly healthy |
| K |
Active |
5+ days |
Slightly overweightb |
24.7 |
27 |
Slightly healthy |
| H |
Active |
1-2 days |
Slightly overweightb |
23.8 |
38 |
Slightly healthy |
| P |
Inactive |
None |
Very overweight |
35.8 |
46 |
Slightly healthy |
| B |
Very Inactive |
None |
Very overweight |
34.0 |
40 |
Healthy |
| L |
Slightly active |
5+ days |
Very overweight |
43.7 |
42 |
Unhealthy |
Table 1: Summary of behaviors related to physical activity and weight (a = the weight perception was underestimated. b = the weight perception was overestimated).
Presentation of qualitative responses/findings
Analysis of the interviews was conducted within the context of the model’s following four concepts: (1) Information, (2) values, (3) preferences and (4) environment-(IVPE). Exploration of the responses resulted in at least three themes per major concept. The concepts and themes are outlined below:
(1) Information:
a. knowledge about food
b. healthy and unhealthy foods
c. nutritional content and requirements
(2) Value:
a. culture
b. physical activity
c. mindfulness/default-thinking
(3) Preferences:
a. weight preferences
b. physical activity preferences
c. food preferences
(4) Environment:
a. context
b. availability
c. access
d. affordability
Model construct: Information
The participants obtained information from numerous sources and seemed to be knowledgeable of healthy/unhealthy foods, but the participants’ understanding of nutritional labels appears lacking (Table 2).
| Concept |
Theme |
Individual Quotes |
Individual Quotes |
| Information |
Knowledge about food |
L: From my mom, that’s the way my mother cooked you know that’s what I’ve learned and that’s what I know that’s fast and that’s what I do. BMI=43.7, Age=42 |
Knowledge about food was obtained from their mothers and external sources such as schools, training programs, physicians, nutritionists and/or TV. |
| C: Um...doctor visits...uh...sometimes the nutritionist from my daughter's school and sometimes from TV. BMI=26.6, Age=38 |
| Healthy and unhealthy foods |
C: er...a lot of fruits and vegetables um...I try to stay away from the red meat, I try to, you know, eat as much chicken. I am supposed to eat the chicken with the skin off…but mainly a lot of fruits and vegetables. I try, but didn't get the 100% you know…BMI=26.6, Age=38 |
Healthy foods were fruits, vegetables and chicken. Unhealthy foods were fat, salt and sugar. There was a need to avoid over eating and control portion sizes. |
| L: …so you definitely want to go reach for a fruit before you reach for a bag of chips. So, if you feel yourself needing to reach for a bag of chips like 3 times a day. Something you eat a carrot instead of chips, so I think that all the foods can be healthy for you in moderation….BMI=43.7, Age=42 |
| B: Just a little bite not too much. Because fruit turns into sugar, that’s what my doctor told me; I eat too much fruit. BMI=34.0, Age=40 |
| Nutritional content and requirements |
B: We tend to do what we like even though we know how to read labels…but if you don’t know then you don’t make good choices. BMI=34.0, Age=40 |
Awareness of nutritional labels is helpful, but may not be enough to make the best food choices. |
| L: I think it gives you the option, I mean because you have the option to make that choice, it will make you stop and think before, even if you choose to still go with the chips maybe next time you won’t go with the chips, so it makes you more conscious of your choices. BMI=43.7, Age=42 |
| H: It wouldn't affect my weight. I think sometimes you can become obsessed with…watching the calories and the fat, and how much is in this. You want to be educated about it and really have a sense for yourself of what's healthy, so not for me...I guess it may affect other people. BMI=23.8, Age=38 |
Table 2: Example quotes highlighting the construct information.
Model construct: Values
The participants explaining that their culture emphasizes the importance of having food at every gathering (Table 3). As with many other cultures, food is celebratory in Black culture. The participants placed high value on balanced nutritious meals: However, valuing balanced meals may conflict with southern/Caribbean style meals. Physical activity values were not explicitly stated: The importance of physical activity appeared to need improvement since the participants seemed to be misinformed about the amount and type of physical activity needed weekly to remain healthy (Table 3).
| Concept |
Theme |
Individual Quotes |
Group Analysis |
| Values |
Culture
Physical Activity |
L: Well Southern. So, there's lots of meat, fried meat. Pork and I think in terms of my eating and the way that I prepare my meals for my family is what I've learned from my mother. And so that now is something that I’ve been trying to change.
BMI=43.7, Age=42 |
Southern/Caribbean style foods are the major focus at all gatherings. |
| B: I would say Sunday you expect macaroni and cheese and collard greens along with either fish or chicken or in my family we have a lot of people that had a stroke, so they mostly eat baked food…but our unhealthy food is the macaroni and cheese. We’re from the south so we grew a lot of our vegetables, so we like a lot of vegetables even here in Flatbush we have a house in Flatbush. We grow the cucumbers, we grow the tomatoes and we grow the lettuces, so we eat a lot of that still. And we love a lot of pecan pie. BMI=34.0, Age=40 |
| P: My mother’s people and my father's…were from the south so the southern cooking is more the genre…and food is a part of everything. I mean food is a part of every celebration, you feel that the food kind of sets the tone for the event so food is very much a part of almost every kind of gathering whether it’s family gathering having friends over or even going away somewhere to a picnic or an amusement park. So, food is in everything and because of that you know I don't know it’s kind of hard to separate food healthy eating from a celebration. BMI=35.8, Age=46 |
| P: Do you have to have the whole meal! People are just going to be there for an hour or can you have something light, but then you know culturally food is the welcoming you know, so it’s like [someone else agrees “right”] are the people going to feel real welcomed if you only have some cheese and crackers, or wait where's the chicken! [laughter] That’s the kind attachment I have with food and culture, so I don't have people over if I’m not cooking. [laughter] BMI=35.8, Age=46 |
| H: Well food is definitely a focus in my culture especially, my family is from the south, my husband's family is Caribbean, so whenever we have events, there's lots of food, so it's a focus. BMI=23.8, Age=38 |
| P: 20 min a day at least of some sort of movement…S: I’m gonna say about half an hour is good. BMI=35.8, Age=46 |
| L: I mean just from hearing and reading and stuff, exercise is supposed to be something, I guess, where your heart rate is supposed to get over a certain amount of something, so whether that could be in 15 or 20 min and you know, 20-30 min. BMI=43.7, Age=42 |
| S: Well I would say try to get the fifteen-min workout every day, if I could do that every day I think I would start seeing some results. Because I was starting to see, but then I fell off again and you know, cause fat, all it does is just turn into muscle when you work out and then when you stop working out the muscle turns back into fat. BMI=33.3, Age=39 |
| H: Well at least an hour a day for me. BMI=23.8, Age=38 |
| |
Mindfulness/Default
Thinking |
C: For me it’s like a balance…a balanced meal, nutritious meal, not so much of the…fast food, the take-out stuff. BMI=26.6, Age=38 |
Balanced nutritious meals that include all food groups, water, small/appropriate portions and limited junk foods. |
| B: I just think of the pyramid, you think healthy. Some grains, some meat, some vegetable, some fruits, some dairy. BMI=34.0, Age=40 |
| P: Not too much in excess! So not too much of any one food group, also I think eating healthy is eating small meals. A lot of small meals and frequent eating as opposed to you know big. BMI=35.8, Age=46 |
Table 3: Example quotes highlighting the construct culture.
Model construct: Preferences
The participants preferred not to utilize a number to describe a healthy weight and they defined a healthy weight as anything other than a number. Specifically, they used significant others, friends, media and pop culture to shape their preferences of a healthy weight. The participants also preferred dancing, skating and walking over gym-based exercises and home cooked meals with large portions of starches (Table 4).
| Concept |
Theme |
Individual Quotes |
Group Analysis |
| Preferences |
Weight preferences |
P: I think that society looks at those charts…and from the time I was a kid, I look at those charts, this is ridiculous, that’s not me, that’s not made for my body. Because whatever the weight was that was considered the large frame, you know, those little charts you see with small, medium, large frame…what am I? This is when I thought I wasn’t in reasonably good shape, so it’s hard to know what to consider a normal/healthy weight. Well one measure I used and I’m still way over, I remember when my daughter was born, the weight that I was when I went in to deliver her and so it’s like, I should at least be below that [laughter] and I’m still way over. The weight that I was when I went in to deliver, so that’s sort of like a threshold, you know, kind of pre-pregnancy weight/size…That’s kind of a milestone for me right now anyway. BMI=35.8, Age=46 |
A normal/healthy weight is anything other than a number. Family members, friends, the media, society and culture help shape their view of what is considered a normal/healthy weight. |
| |
B: I guess if you feel good and you’re not at-risk health wise you’re okay. I used to…the weight used to be a thing for me, but it’s not any more, my husband loves me just the way I am. He always tells me that if you don’t get small, I love you just the way you are, so it’s not, I’m not focused on my weight, so I just focus on you know I have my exercise, my walking. I do watch what I eat most of the time, so it’s not; the weight is not a focus for me. BMI=34.0, Age=40 |
|
| |
|
L: What I try to gauge it by is what size clothes I feel good in. And so, I can fit into a certain size, so then the number on the scale doesn’t matter to me because then I know that this is what made me feel good or I know if I’m fitting into this size clothes then I think that this is the size for me. BMI=43.7, Age=42 L: Because if I go any lower which I went like to one of those Mac crazy diets once to the weight that they said that I should be and my father said you look like a crack head. I’m sorry you know, so it’s like really bad. And so, you know it’s like we just can’t go by those charts you have to go by how you feel. What makes you feel happy because then you’re going to continue to try to maintain that weight as much as possible and you know as long as you go to your appointments and you’re healthy with everything else, then that’s what, that’s all that matters. I think it’s just your clothes size and what clothes size you feel most comfortable in and that is how you would gauge it. BMI=43.7, Age=42 |
|
| |
Physical activity preferences |
S: Well like I say: Consistency. We have the equipment, um…now and then we do get to it. Well last night, my oldest daughter, we like to dance. So, she loves reggae and she’ll put the reggae music on and we’ll wind it up and (laughing) so we’ll get the workout in like that. BMI=33.3, Age=39
S: We do a lot of walking. Yeah, I mean she, she just graduated as a medical assistant, so her dad bought her a convertible. It’s in the back yard because we plan to do driving lessons together. And, um, I mean I’m still not enthused about driving. I don’t know what it is. I like to be driven, but I’m trying to change my thinking about it. But before the car issue we walk everywhere. I don’t like to take cabs too much. So, we’ll get the workout in by walking. BMI=33.3, Age=39. |
|
| |
|
K: Well I do believe in physical, um activities and exercise, um…as far as…do we get…? Well, on the weekends, um we go upstate, and she has a big yard to play, she got a bike. We do ride, we play like, well it’s mostly in the, um…summer cause in the winter it’s cold, but um…from time to time we play volley ball together. We’ll go bowling…we do a lot of things. Not exercise, exercise on a regular basis, but we do physical activities. BMI=24.7, Age=27 |
|
| H: I think it's important; as I said earlier, I don't like it; I don't like working out. I do like dancing. I do like fun activities. I like roller-skating, things like that but I don't like the gym and the treadmill and those things. BMI=23.8, Age=38 |
| |
Food preferences |
K: Well I’m trying to stick with healthy stuff, um…I’m trying to…I just buy chicken and fish and um…I’ll get lettuce, tomato, cabbage, carrots…um celery, all that stuff…I’m limiting the rice, um by using the brown rice instead of white rice. I’ll get potatoes and…well…I’m trying to go healthy. BMI=24.7, Age=27 |
|
| |
|
A: Well, from the West Indian culture, again, we have an extended family in the household and most of the times I’m not the one that’s cooking and my choices are totally different from the rest of the family’s choices, so we eat what’s there. So, it’s mostly starches, um…I would prefer more vegetables in our diet. BMI=27.4, Age=44 |
|
| H: I prefer to eat like I said French fries, I love French"-fries and pizza, but I don’t buy them for home. I eat them out. I like vegetables; I love beans; I love beans and buy beans for home and I usually prepare them. And I like fish and shrimp I usually don't buy shrimp for home; I eat it out. BMI=23.8, Age=38 |
|
Table 4: Example quotes highlighting the construct perferences.
Model construct: Environment
The participants described their contextual environment as urban living with small spaces that impacted their food purchases as well as storage and daily meals. A description of what was available in their environment revealed that they had access to fresh foods. However, time, convenience and cost were issues for both activity and fresh food. In addition, access to green spaces, parks and places for increased activity were hampered by safety concerns and various levels of motivation. Finally, food variety and freshness were sacrificed for price since nearby store owners had small spaces and only supplied smaller quantities that would sell within 2 or 3-days (Table 5).
| Concept |
Theme |
Individual Quotes |
Group Analysis |
| Environment |
Context |
K: Yes, Well, it depends on where I go to shop, because there’s a super market right by me, their fruits and vegetables are expensive, but going a little further away, things are more reasonable. BMI=24.7, Age=27. |
•Location, price and time mainly influenced their food purchases.
•Their level of physical activity was mainly influenced by time, health and desire.
•
While the participants agreed they had access to exercise or could participate in recreational activities in your neighborhoods, ease or difficulty with physical activity depended on desire, motivation, and interest
|
| A: Chains are more expensive than others; I venture out of my neighborhood and have to go to Fort Hamilton, where the produce is much cheaper. I would venture out towards Mendon Boulevard to get my meats, so having a vehicle is helpful in order to get affordable fruits, vegetables and meats. BMI=27.4, Age=44 |
|
| |
P: The time, yeah. My job is kind of beyond 35 hours a week. It’s until it’s done, so sometimes I have to be up early and sort of working from home; working from home on the weekends, so many times going into things on the weekend, so I don’t have a lot of time, so that’s a major factor in determining how much exercise. [laughter]. BMI=35.8, Age=46 |
|
| A: My day is really long. Um, by the time I get home, well it depends, sometimes I get off at 3:30 and sometimes I get off at six. By the time I get home it’s late, you know and homework and stuff like that. BMI=27.4, Age=44 |
|
| |
H: Time...time...time, time, time and the desire to do it. BMI=23.8, Age=38 |
|
| L: Well basically mine was time and the limited health issue. BMI=43.7, Age=42 |
|
| Availability |
P: In my neighborhood, I live in Harlem, in immediate walking distant there are 2 markets. In the farther away they carry some organic lines but not much, but the markets close to me rarely have anything organic they certainly have fruits and vegetables and other healthy choices. What I tend to do is once every 2 weeks or so try to go a whole foods type market or something like that when it’s on the way. But it’s not always convenient and the things that I need. I try to buy frozen organic broccoli…but I have a small fridge and small freezer, so I have to go shopping every couple weeks anyways so it sort of isn't convenient in terms of just getting there to and from work or after activities verses it would be better if I could just walk around the corner on a Saturday. BMI=35.8, Age=46 |
|
| |
L: There’s a health food store that has just come on Fulton Street and they offer smaller portions and I think that’s where my problem comes in because I'm used to purchasing my food in bulk, once every 3 months. Because I think if you want to do organic and you want to do vegetables this means a stop at the super market every day or every other day and then that becomes the time factor. So, that makes you go back to cooking these frozen vegetables, there’s meat that I have already in the freezer. My neighborhood is changing now they’re trying to change some of the items that they bring into the super market, so you do have an option of getting some organic foods and again it is pricey; they also have the farmers market I think now in Fort Green. Fort Green Park on some Saturdays, but you can only purchase so many vegetables because if you don’t cook it right away then it’s going to go to waste. BMI=43.7, Age=42 |
|
| |
H: There are opportunities [to exercise], they cost, you have to pay for them; there's nothing really free in my neighborhood. BMI=23.8, Age=38 |
|
Access,
Affordability |
S: We do have opportunities to exercise; I don’t particularly like to go to a gym. I don’t know what it is. I’ve never been a type to want to sign up. I like to just work out at home. I like to do everything at home (laughing). So, I’m the homely type. BMI=33.3, Age=39 |
•There are opportunities to exercise in the neighborhood but are not free.
•There were opportunities to exercise in their communities. However, the participants were conflicted between desire to be active, time commitments and efforts to participate.
|
A: There are opportunities [to exercise] in my neighborhood. We have the YMCA. They have parks, and they have fitness centers and stuff like that, but…Um, I don’t know if they are conveniently located or affordable. BMI=27.4,
Age=44. |
| |
K: Well, um in my neighborhood there are the parks and there’s the fitness program. But I never was to the fitness program, so I don’t know how much it is. I did have YMCA membership and I used to go, but…I don’t get time to go no more. Cause some of the weekends I do work…BMI=24.7, Age=27 |
|
| K: Well, it depends on where I go to shop, because there’s a super market right by me and their fruits and vegetables are expensive, but going elsewhere I’ll get things more reasonable. BMI=24.7, Age=27 |
•Quality may be adjusted or sacrificed for price. Participants traveled outside of their immediate neighborhoods, suggesting they did not have affordable quality fresh foods in their neighborhoods.
|
| A: Some chains are more expensive than others. I venture out of my neighborhood where I go to Fort Hamilton. Around that area where the produce is much cheaper. I would venture out towards Mendon Boulevard to get my meats, so having a vehicle is helpful in order to get affordable groceries. BMI=27.4, Age=44 |
| H: They're very expensive in my neighborhood. I mentioned earlier that I was from Brooklyn, so a lot of the prices are very different in terms of the fruits and the vegetables. In my opinion, most healthy things are much more expensive then the non-healthy things. It’s more expensive on Long Island then it was in Brooklyn. So sometimes, especially in this economy, making a choice about fruits and vegetables, I'm not getting as much as I might have before. BMI=23.8, Age=38 |
Table 5: Example quotes highlighting the construct environment.
In summary, the interaction of the four concepts of the model: Information, values, preferences and environment (IVPE) suggest that the participants combined these in their decisions concerning food choices and physical activity. While there were areas of strength, the following areas need improvement: 1) Information on how-to read and understand nutritional labels, 2) values about the amount and type of physical activity needed weekly to remain healthy, 3) preferences based on science, research and guidelines and 4) environment that promotes desire for physical activity and access to local markets with a variety of fresh foods.
Discussion
Findings
We found that the decision-making process involves the interconnection of information, values, preferences and environment (IVPE) from the Adapted Model of Decision- Making among Black women. Decisions about food choices and physical activity stemmed from the interaction of IVPE. The interaction of a four-concept design suggests that decisionmaking is a process that includes the environment. Moreover, the study suggests specific food and physical activity-relatedbehaviors may influence weight outcomes.
Information
Information about food and physical activity, gained from multiple sources, while sometimes inaccurate, resulted in decisions reflected in the participant’s weight outcomes. Specifically, the participants with BMIs in the overweight and obese categories had inaccurate information about food preparation, types of foods and portion sizes. The amount of physical activity needed to remain healthy and types of physical activity most helpful to control their BMI were also inaccurate. Participants over or under estimated the amount of physical activity with misinformation ranging from 105 to 420 min/week. The participants’ types of activity ranged from minimal movement (sedentary) to moderately active movement (walking and dancing). The US Department of Health and Human Services and US Department of Agriculture (USDHHS & USDA) recommends adults should do at least 150 min a week of moderate-intensity activity or 75 min a week of vigorous-intensity aerobic activity or an equivalence combination of moderate- and vigorous-intensity aerobic activity [13,14]. Gummelt defined physical activity as “movement that is carried out by the skeletal muscles that requires energy”. More specifically, exercise is a subcategory of physical activity [15]. They explain that exercise is structured, planned, intentional and repetitive movement with the intent to improve or maintain one’s physical health. Government recommendations that speak of aerobic activity were beyond the information base of our participants. This lack of information may contribute to obesity among Black women.
Values
The participants’ values were not unique to Black culture. Similar to past posits by Rodin, Silberstein and Striegel-Moore and Fieldhouse, even today, many cultures view food as a way of expressing love, warmth and acceptance [16-20]. The participants reported that they valued balanced meals. However, they also reported that most of their meals consisted of southern and/or Caribbean style foods that were often fried and there were large portions of starches and small portions of vegetables. Thus, their description of meals was not a balance of proteins, carbohydrates and fats. In fact, their meals were high in fat and calories which may have lacked essential vitamins and minerals [13,14]. Moreover, the participants did not place a high value on physical activity. This may be due in part to their lack of accurate information regarding the amount and type of physical activity needed to achieve and maintain a healthy lifestyle.
Preferences
The participants preferred to use non-scientific indicators to determine whether they were a normal/healthy weight. Instead of using a BMI, they favored the fit of their clothing or their significant others’ opinion of their appearance. These findings are similar posits from Johnson and Wesley [21]. Their method may have shielded their self-esteem and protected them from depression, but the method did little for them to achieve a healthy lifestyle. Furthermore, following inaccurate measures of a healthy weight lead the women to decisions about food and physical activity that put them at increased risk of obesity and obesity-related illnesses. By denying scientific danger signals, some women’s sense-of-self may have been less threatened and they may have avoided emotional upset, but it did little to improve their decisions about food and physical activity. These findings were similar to Kwan’s findings, among 42 obese or overweight participants that BMI fails to acknowledge emotional and/or psychological dimensions of health and is not a good measure of overall health [22]. Despite scientific evidence, Kwan’s participants rejected the evidence and resorted to their lived experiences and personal views to achieve what Kwan labels as happiness.
Environment
The environment provided the context which shaped the participants’ information, values and preferences, yielding an impact on decisions regarding both food choice and physical activity. While availability and accessibility were not seen as barriers, affordability and time constraints posed a challenge to healthy eating and physical activity according to the participants. These findings were similar to Onubogu, et al. finding among 19 adults, that time was a barrier to completing their action plan on self-management of weight [23].
An understanding of the context that was created by the environment exposed a default-type of decision-making found among the participants. These default or pre-set decisions ranged from eating whatever was most convenient at the time such as fast foods or pre-packed less nutritious, high carb/ fat foods to home cooked meals with vegetables. Similar to Mason and colleagues’ study of 194 obese individuals revealed that increased use of mindful eating rather than default-type decisions had better weight loss and less eating of sweets than participants who reverted to default-type decisions [24].
In addition, how the women shopped for their families varied from frequent local market purchases to less frequent bulk purchases at big box stores. In local markets, fresh foods were costlier while bulk purchases raised the issue of limited space to store large quantities. Therefore, frequent trips to the market yielded time issues, whereas bulk purchases created storage issues. Unlike comments from this study’s participants about their shopping environments, Amaro et al. addressed the shopping environment, suggesting that the design, placement and choice of items create an overwhelming array of tempting unhealthier options that persons who are not mindful may give way to temptation thereby making poor food choices [9].
Consistent with food choices, decisions regarding physical activity were impacted by the environment. While government guidelines from 2015 recommended daily brisk walking to improve one’s health, the participants’ decisions regarding activity levels ranged from inactivity to very active. Default-type decisions were made within an environment where there was a lack of access to tennis courts, swimming pools and green spaces. The lack of free access to physical activity in a park was overshadowed by safety concerns. As suggested by Frieden public health interventions that change default-type decisions and the environment have potential for long-term health impact [25]. Interventions that highlight the benefits of changing default-type decisions may help increase healthy living despite environmental constraints.
In contrast to findings from our study, Richardson and colleagues’ study of 791 Black adults found that an environment with walkability was a better predictor of moderate to vigorous activity (β=0.55, p=0.007) than accessible green space or concerns about crime rates [26]. McCormack, et al. also suggested that neighborhood environments with increased walkability improve physical activity based on their findings from adults self-reporting [27]. Similar to McCormack and colleagues, call for public health policies that increase physical activity and decrease health disparities [28].
Limitations
This study attempted to understand the participants’ complex reality of food choices, physical activity and body weight from the theoretical perspective of the Adapted Model of Decision-Making, however, researcher bias is inherent and somewhat inevitable (Polit & Beck, 2017). The ability to replicate the results that were interpreted within the context of a focus group milieu is limited. Although the sample size is small, saturation of responses among the women indicate the results are trustworthy. Another limitation of focus groups is the tendency for certain opinions to emerge more strongly and let certain participants dominate the sessions. To address this issue, data were analyzed on both the individual and group levels. Study participants had a similar demographic profile of residents in the study environment, which provides transferability among similar communities.
Conclusion
The Adapted Model of Decision-Making facilitated an understanding of the complex interconnection of information, values, preferences and environment (IVPE) regarding decisions, behaviors and outcomes. This qualitative study suggested how decisions stem from the interconnection of IVPE, resulting in behaviors that lead to positive or negative outcomes. Thus, decisions about food choices and physical activity stemmed from the participants’ sources of information, family values and personal preferences within the context of their environment. These decisions lead to certain food choices and their level of physical activity that resulted in the BMIs recorded from the study participants.
Implications
Quantitative research is needed to identify the strength of relationships among IVPE among Black women. In addition, quantitative research should determine the impact of IVPE on decisions and subsequent behaviors that may lead to outcomes, before interventions can be designed.
Acknowledgement
We would like to thank the following for their contribution to this project: A. Cespedes, MPH, E. Kade, MSN, APN-C, Y. Martinez, MSW, C. Millman, MSN, APN-C and M. Parrish, MSW, LCSW, C. Brooks-Harrison, MSW, LCSW.
Funding
Pless Center for Nursing Research, New York University College of Nursing at the College of Dentistry.
1In the United States, people of African descent are generally referred to as African American, African Caribbean, or African immigrants. We acknowledge the African Diaspora and the diversity among people of African descent. Therefore, in this article, women of African descent will be referred to as Black.
References
- Saydah S, Bullard KM, Cheng Y, Ali MK, Gregg EW, et al. (2014) Trends in cardiovascular disease risk factors by obesity level in adults in the United States, NHANES 1999-2010. Obesity. 22:1888-1895.
- PapadopoulosS, Brennan L (2015) Correlates of weight stigma in adults with overweight and obesity: A systematic literature review. Obesity. 23:1743-1760.
- Ogden CL, Carroll MD, Fryar CD, Flegal KM (2015) Prevalence of obesity among adults and youth: United States, 2011-2014. NCHS Data Brief. 219:1-8.
- Wills CE, Holmes-Rovner M (2006) Integrating decision-making and mental health interventions research: Research directions. Clin Psychol.13:9-25.
- Rothert ML, Holmes-Rovner M, Rovner D, Kroll J, Breer L, et al. (1997). An educational intervention as a decision support for menopausal women. Res Nurs Health. 20:377-387.
- Citroen CL (2011) The role of information in strategic decision-making. IJM. 31:493-501.
- Chen R, Smyser M, Chan N, Ta M, Saelens BE, et al. (2015) Changes in awareness and use of calorie information after mandatory menu labelling in restaurants in King County, Washington. Am. J. Public Health. 105:546-553.
- Nikolova HD, Inman JJ (2015) Healthy choice: The effect of simplified point-of-sale nutritional information on consumer food choice behavior. J Mark Res. 52:817-835.
- Amaro H, Cortes DE, Garcia S, Duan L, Black D (2017) Video-Based Grocery Shopping Intervention Effect on Purchasing Behaviors Among Latina Shoppers. Am J Public Health. Washington 107:800-806.
- Viola D, Arno PS, Maroko AR, Schechter CB, Sohler N, et al. (2013) Overweight and obesity: Can we reconcile evidence about supermarkets and fast food retailers for public health policy? J. Public Health Policy. 34:424-438.
- Auchincloss AH, Young C, Davis AL, Wasson S, Chilton M, et al. (2013) Barriers and facilitators of consumer use of nutrition labels at sit-down restaurant chains. Public Health Nutr.16:2138-2145.
- Polit DF, Beck CT (2017) Nursing research: Generating and assessing evidence for nursing practice. 10th Edn. Philadelphia. Wolters Kluwer, Lippincott Williams and Wilkins.
- US Department of Health and Human Services and US. Department of Agriculture. (2015a) Dietary Guidelines for Americans. 8th Edition.
- US Department of Health and Human Services and US. Department of Agriculture. (2015b) Dietary Guidelines for Americans. 8th Edition.
- Gummelt D (2015) Physical Activity vs. Exercise: What’s the Difference?
- Rodin J, Silberstein L, Striegel-Moore R (1984) Women and weight: A normative discontent. In Nebraska symposium on motivation. University of Nebraska Press.
- Fieldhouse P (1995) Food and nutrition: Customs and culture. Springer-Science + Business Media, BV, Netherlands.
- Johnson P, Wesley Y (2012) Scholarly Perspectives on Obesity among Black Women. The ABNF Journal. 23:46-50.
- Johnson P, Wesley Y (2013) The Skinny on Fat & Exercise: Truth about Obesity. In Catherine Collins 3rd Edition, African American Women’s Life Issues: Today’s Vital Health and Social Matters. Santa Barbara California: Praeger/Greenwood Publishing.
- Hamburg ME, Finkenauer C, Schuengel C (2014) Food for love: The role of food offering in empathic emotion regulation. Frontiers in Psychology. 5 article 32.
- Johnson P, Wesley Y (2015) Obesity in Black Girls: The Curse of a Poverty Diet and Fast Food. In Catherine Collins (Ed.), Black Girls and Adolescents: Facing Life Challenges. Santa Barbara California: Praeger/Greenwood Publishing.
- Kwan S (2012) Lay perspectives on the biomedical paradigm on 'obesity': Theorizing weight, health and happiness. Soc Theory Health.10:61-77.
- Onubogu U, Graham ME, Robinson TO (2014) Pilot study of an action plan intervention for self-management in Overweight/Obese adults in a medically underserved minority population: Phase I. ABNF Journal. 25:64-71.
- Mason AE, Epel ES, Kristeller J, Moran PJ, Dallman M, et al. (2016) Effects of a mindfulness-based intervention on mindful eating, sweets consumption, and fasting glucose levels in obese adults: Data from the SHINE randomized controlled trial. J. Behav. Med. 39: 201-213.
- Frieden TR (2010) A framework for public health action: The health impact pyramid. Am. J. Public Health.100:590-595.
- Richardson AS, Troxel WM, Ghosh-Dastidar MB, Beckman R, Hunter GP, et al. (2017) One size doesn’t fit all: Cross-sectional associations between neighborhood walkability, crime and physical activity depends on age and sex of residents. BMC Public Health. 17:97
- McCormack GR, McLaren L, Salvo G, Blackstaffe A (2017) Changes in objectively-determined walkability and physical activity in adults: A quasi-longitudinal residential relocation study. Int. J. Environ. Res. Publ. Health. 14:551.
- Hamalainen R, Sandu P, Syed AM, Jakobsen MW (2016) An evaluation of equity and equality in physical activity policies in four European countries. Int J Equity Health.15:191.

