Margaret O’Riordan MD1,Andre´ Dahinden MD2, Zekeriya Aktu¨ rkMD3*, Jose´ Miguel Bueno Ortiz MD4,Nezih Dag? deviren MD5,Glyn Elwyn MD6,Adrian Micallef MD7,Mikko Murtonen MD8,Marianne Samuelson MD9,Per Struk MD10,Danny Tayar MD11and Janecke Thesen MD12
1National Director of Specialist Training in General Practice, Irish College of General Practitioners, Dublin, Ireland
2General Practitioner, SGAM, La Neuveville, Switzerland
3International Officer, Spanish Society of Family Community, SEMFYC International Section, Barcelona, Spain
4Professor, Trakya University Medical Faculty, Department of Family Medicine, Edirne, Turkey
5Professor, Department of General Practice, Centre for Health Sciences Research, Cardiff University, Neuadd Meirionnydd, Wales, UK
6Quality Assurance Secretary, Malta College of Family Doctors, Malta
7General Practitioner, Finnish Association for General Practice, City of Espoo, Espoon kaupunki, Finland
8Professor, De´ partement de Me´ decine Ge´ ne´ rale, Faculte´ de Me´ decine, Universite´ de Caen, Caen, France
9Consultant, Czech Society of General Practice, Praha, Czech Republic
10Consultant, The Mifne Centre, Tel Aviv, Israel
11Senior Registrar Consultant/Researcher, The National Centre for Emergency Primary Health Care, University of Bergen, Bergen, Norway
12Background paper by Members of the European Association for Quality in General Practice/Family Medicine (EQuiP)
Corresponding Author:
Dr Zekeriya Aktu¨rk
Atatu¨rk University Medical Faculty
Department of Family Medicine
Erzurum, 25240, Turkey
Tel: +90 535 7140843
Fax: +90 442 2360968
Email: zekeriya.akturk@gmail.com
Received date: 28 September 2010; Accepted date: 23 March 2011
Keywords
general practitioners, training, uncertainty
Introduction
Uncertainty and unpredictability are core elements in the complex system of healthcare provision, presenting challenges for health professionals, patients and managers.[1] Skills to deal with uncertainty are particularly important in general practice as undifferentiated and unorganised problems are a common challenge for general practitioners (GPs),[2] in contrast to the caseload of many hospital colleagues.[3] Since there is usually no obvious diagnosis at point of patient presentation, one can say that uncertainty is inherent in general practice.
Doctors’ and patients’ level of certainty seem to be directly correlated and interdependent. Validated scales have been developed to measure uncertainty in physicians [4] and as a source of stress for patients.[5] Tolerance of diagnostic uncertainty seems to affect test ordering behaviour,[6] and medico-legal worries have been implicated as one of the reasons for the increasing use of tests by GPs.[7,8] On the other side, uncertainty is a powerful source of stress for patients[9] and GPs[10] and has been linked to burnout.[11] Grol et al linked uncertainty to personality and developed a scale of risk avoidance.[12]
This paper describes management of uncertainty as an essential skill, which should be included in educational programmes for both trainee and established GPs. It was developed as a result of several discussion group meetings of interested EQuiP delegates, general reading around the subject and a focus group held at a European conference.
The conceptual approach to managing uncertainty
It is possible to adopt a number of different approaches which influence the way in which we conceptualise the importance and the implications of managing uncertainty. Taking a philosophical approach, the existentialist believes that most of the time humans manage to bridge the gap between the need for order and constancy on one hand and the unavoidable reality of lonely and limited existence in a chaotic and therefore unpredictable world on the other. Therefore uncertainty arises when a patient presentation produces a sense of helplessness in the doctor (a product of lifelong existential reality).
If we were to adopt a psychological approach we could say that uncertainty can arise due to a cognitive process (difficulty in perception and interpretation of facts by the doctor), and/or a personality clash and/or as an indivisible part of doctor–patient interaction and communication. In contrast, the sociological literature challenges the assumption that human beings are rational decision makers and instead describes the so-called ‘social processes model’ of decision making. [13]
Rational thinking is an important part of the process but is not the whole story. Rather than balancing the pros and cons of any decision in an objective and logical way, the social processes model emphasises the wider context within which decisions are made, risk is managed and uncertainty is dealt with. Decisionmaking is seen as a complex, iterative social process, influenced by personal experiences and by the views of and advice from other people (the validity of which is based on the level of trust between the giver and the receiver of the information). Objective information and rationality therefore play only one, sometimes small, part in a ‘knowledge construction’ process that underlies how people deal with uncertainty as they make clinical decisions.[14]
A practical approach to uncertainty
There are many consultations where there are no straight answers, no clear diagnosis and no obvious treatment, where guidelines and decision-making protocols do not lead to a satisfactory outcome. In this situation, at one extreme the doctor who believes in their own infallibility when faced with diagnostic decisions can be a source of danger, as can the doctor at the other extreme who struggles with indecision on a daily basis. For the majority, however, uncertainty is a normal component of the working day and dealing with it is a necessary skill. The literature on dealing with uncertainty in practice focuses largely on identifying relevant evidence and decision making.
Identifying relevant evidence
In order to identify evidence, one should know that there is appropriate evidence present. Then, one should have access to the evidence at the time it is needed during the consultation. Evidence-based medicine is a useful tool when faced with uncertainty, particularly when discussions of probability[15] are employed. However, when all available evidence has been sought and found wanting it can be a challenge to know when to stop the quest for a definitive answer (e.g. GPs’ desire to understand complaints and meet patient expectations seems to affect their test ordering behaviour even when tests are not indicated according to clinical guidelines).[16] As James[17] so eloquently puts it, ‘the limits of evidence-based medicine and guideline use in clinical practice may be found in the grey zones of uncertainty where science meets art.’
In an interesting approach to test ordering, Sonnenberg[18] appeals to doctors to consider his socalled medical uncertainty principle. This is based on Heisenberg’s uncertainty principle from quantum mechanics. Put in simple terms, the principle implies that as doctors’ diagnostic certainty increases due to the use of diagnostic tests a patient’s health deteriorates as a result of the investigations. In order to use tests rationally and reasonably, doctors need to be able to tolerate a certain amount of uncertainty.
Medical decision making
Science appears to offer a sense of security in medical decision making but this may be lost when faced with uncertainty. Analysing decision making is cited as a key area in helping doctors to deal with uncertainty, and this view is supported by the literature.[19–24]
Patient-related factors such as co-morbid conditions, quality of life indices, the financial situation and restricted access to health care are all important factors in medical decision making.[23] Summerton3 suggests that decision making in primary care is a very different process from that undertaken by hospitalbased doctors. It is particularly important to analyse symptoms from a patient’s perspective, taking context into account. Experienced clinicians seem to base their diagnoses on cognitive structures which they have developed from dealing with a series of similar patients in the past. Having reflected on how they dealt with one patient they then extrapolate their findings to others. This involves a combination of reflection in action (during the consultation) and reflection on action (afterwards).[25]
Arborelius et al26 analysed consultations where GPs appeared unsure in their interactions with patients – this appears to have been compounded by the fact that the GPs did not acknowledge and use their feelings of uncertainty as useful information. Baerheim[20] describes the diagnostic process starting from a patient’s history and proceeding to a result that can be categorised. Patients do not present their symptoms as a list but rather in the context of a story of how these symptoms have affected their lives and the chronological order in which they appeared – a story of illness.
The doctor gathers, sifts and prioritises the information presented in order to identify a few possible diagnoses – much of this process may take place at an unconscious level. Patients rarely present perfect textbook symptoms that can be readily classified into a neat diagnosis – most stories are complicated by multiple symptoms and contextual variations. Some of the most important symptoms from the doctor’s diagnostic perspective may be regarded as trivial by the patient and may be mentioned as an aside to the main story. The ability to pick up these threads seems to be one of the characteristics of an expert and may be missed by the inexperienced doctor. One difficulty at this point arises in patient involvement and shared decision making.
Having arrived at a tentative diagnosis the doctor then tests his or her theory, most commonly by the use of a closed question. There are, therefore, two clearly defined phases to this process – the first is information gathering and the second is applying tests to check if the initial diagnosis can be verified. These tests include checking the patient’s perspective – after all, the doctor is the expert on the disease but the patient is the expert on their own illness. Some authors categorise doctors’ competence into ‘Professional readiness’ and ‘Working behaviour’, where professional readiness comprises the inclination to understand and act based on medical knowledge, modified by experience, knowledge of the patient, involvement and uncertainty. [27] As to Wulff ’s suggestion,[28] it is not possible to offer the patient ‘just the facts’, explain the different options, and then leave it to the patient to make the choice. He claims that there is an inherent element of paternalism in clinical decision making and that clinical practice presupposes a mutual trust between physician and patient.
The new science of the probabilistic paradigmis one that accepts a degree of uncertainty as an inherent part of reality and includes values and feelings as an inescapable concern of science. Within the new paradigm decision making is no longer based on ‘optimal’ solutions provided by scientists.29 The actors involved must agree on the definition of perceptions, narratives, interpretation of models, data and indicators that are selected by the scientists. The role of scientists still remains crucial, though it is somewhat changed. They have to contribute to the definition of acceptable compromises. For this purpose, scientists have to contribute to society by learning as quickly as possible about different perceptions towards options, problems and constraints, instead of seeking deep ultimate knowledge.30
Traditionally doctors are trained to seek certainty and their concept of rationality is grounded in the mechanistic paradigm, which has no place for uncertainty, therefore making it difficult to be rational about uncertainty.31 The probabilistic paradigm describes a set of probable causes in constantly changing configurations replacing the old concept of a definite cause or causes for a given effect.
Training doctors to deal with uncertainty
Training doctors to deal with uncertainty should concentrate on shared decision making, meticulous evaluation, exclusion of relevant worrisome differential diagnosis and establishing a relationship of trust with the patient.32 Rules of thumb or heuristics have been identified as short cuts used by GPs in formulating a diagnosis. Andre´ et al19 demonstrated that GPs could readily identify with this concept and regularly used such rules to simplify their work. In many cases the rules were learnt from respected colleagues. An example19 would be ‘when a patient is able to bear weight on a leg it is not broken’. This suggests a role for GP trainers who as role models need to be aware of their own rules and the influence they may have on trainees.
An important aspect of doctors’ training and uncertainty is the inability of trainers and/or training systemto cope with the highly dynamic and challenging environment of practise. Using an outcomes-based approach and engaging with key stakeholders may provide an opportunity to identify and promote critical capabilities needed by managers to support the challenges confronting health services, including workforce flexibility.33 Richardson’s suggestion on this point is for health management education to acknowledge the uncertainty within a multifaceted and complex health system.34 He states: ‘Health management educators challenged to prepare managers for a complex and volatile systemwill need to be bold in the design of new curriculum’.
When a trainer is analysing a consultation, they should look out for the pitfalls identified in Box 1.

Trainers are often urged to encourage their trainees to involve patients as far as possible in shared decision making. Chalmers38 maintains that explicit admission of uncertainty by doctors can undermine patients’ confidence and may reduce the therapeutic effectiveness of individual encounters. Shared decision making and a patient-centred consultation approach encourages the sharing of uncertainty with patients, but the impact of this on patients has not been researched to any great degree.
In an interesting UK study,39 differences between verbal and behavioural activity during consultations emerged. GPs and patients viewed GP verbal expressions such as ‘I don’t know’ as detrimental to patient confidence. However, GP behaviour such as consulting books, asking a hospital colleague for advice or referring to hospital were regarded as neutral or even positive activities by patients. Overall, doctors underestimated the impact of their verbal comments on patient confidence. Older patients from a higher social class that knew their doctors better were more confident in dealing with doctors’ expressions of uncertainty.39
Complexity theory can be used as a model to teach about management of uncertainty within the consultation. Innes et al40 use the Stacey diagram41 (Figure 1) to illustrate the relationship between the certainty of cause and effect and the uncertainty of diagnosis. Complex problems are a normal part of general practice – the GP who tries to be 100% rational in every diagnostic decision is at risk of burnout. The ability to accept the fact that uncertainty is part of the system a doctor is working in and not a reflection on professional inadequacy is paramount to survival. Box 2 contains a list of useful points for the trainer to consider when teaching about management of uncertainty in general practice.
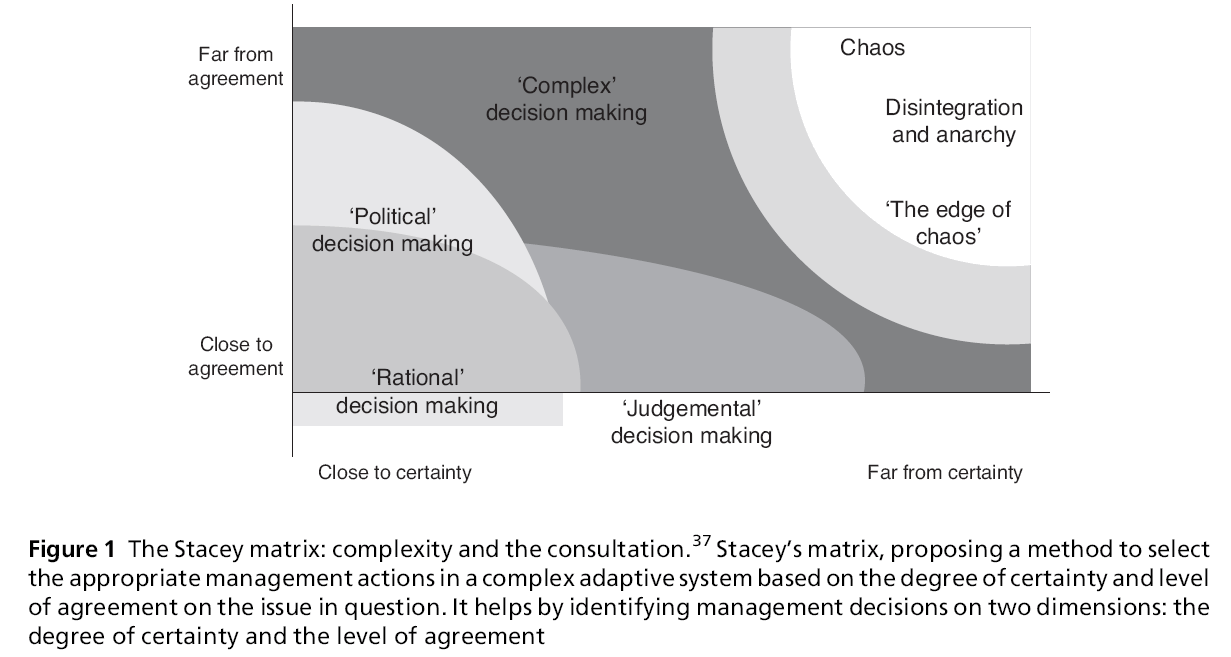
Figure 1: The Stacey matrix: complexity and the consultation.37 Stacey’s matrix, proposing a method to select the appropriate management actions in a complex adaptive system based on the degree of certainty and level of agreement on the issue in question. It helps by identifying management decisions on two dimensions: the degree of certainty and the level of agreement
Conclusion
Existing models of the consultation need to be revised to understand consultations involving uncertainty. An alternative approach focusing on shared decision making42 and understanding the consultation from the patient’s perspective is suggested.43 A good doctor– patient relationship is vital, creating trust and mutual respect developed over time with good communication skills. If the patient believes that the doctor is trying to understand their story and that the doctor’s motivation is to do their best for the patient then they will be empowered to deal with uncertainty. Evidencebased medicine should be used, including discussion of probabilities where available. Trainers need to be aware of their own use of heuristics as they act as role models for trainees. Expression of feelings by trainees should be encouraged and acknowledged by trainers as a useful tool in dealing with uncertainty.
Strategies for dealing with uncertainty need to be considered and debated more explicitly and patients must be involved in this process.43 The public needs to be educated on the limits of the medical knowledge base and the degree of uncertainty that is part of every clinical encounter.
Skills to deal with uncertainty should be regarded as quality improvement tools and included in educational programmes involving both trainee and established GPs.
AcknowledgementS
A focus group comprised of 25 GPs from12 countries (Belgium, Denmark, France, Finland, Germany, Iceland, Ireland, Israel, Norway, Switzerland, Turkey and the UK) produced their own solutions based on personal experience of dealing with uncertainty at an EQuiP workshop in Belgium in 2004. Despite working in diverse healthcare systems there was a unanimous feeling that the solutions arrived at by the group were applicable in all settings.
Peer Review
Not commissioned; externally Peer Reviewed.
Conflicts of Interest
None.
References
- Sweeney KG and Mannion R. Complexity and clinical governance: using the insights to develop the strategy. British Journal of General Practice 2002;52:S4–S9.
- McWhinney IR.A Textbook of Family Medicine (2e). London: Oxford University Press, 1997, pp. 163–5. 3 Summerton N. Making a diagnosis in primary care: symptoms and context. British Journal of General Practice 2004;54:570–1.
- Gerrity MS, Devillis RF and Earp JA.Physician reaction to uncertainty in patient care.A new measure and new insights. Medical Care 1999;28:724–36.
- Mishel MH.The measurement of uncertainty in illness. Nursing Research 1981;30:258–63.
- Van der Weijden T, van Bokhoven MA, Dinant GJ, van Hasselt CM and Grol RP. Understanding laboratory testing in diagnostic uncertainty: a qualitative study in general practice. British Journal of General Practice 2002; 52:974–80.
- Britt H, Knox S and Miller GC.Changes in Pathology Ordering by General Practitioners in Australia 1998–2001. Canberra: AIHW, 2003. Report No.: AIHW General practice series no. 13. Cat. no. GEP 13.
- Winkens R and Dinant GJ. Evidence base of clinical diagnosis: rational, cost effective use of investigations in clinical practice. BMJ 2002;324:783.
- Nessa J and Malterud K. Tell me what’s wrong with me: a discourse analysis approach to the concept of patient autonomy. Journal of Medical Ethics 1998;24:394–400.
- Branthwaite A and Ross A. Satisfaction and job stress in general practice. Family Practice 1988;5:83–93.
- Goehring C, Bouvier GM, Kunzi B and Bovier P. Psychosocial and professional characteristics of burnout in Swiss primary care practitioners: a cross-sectional survey. Swiss Medical Weekly 2005;135:101–8.
- Grol R, Mokkink H, van EijkJThM et al. UnsicherheitbeiarztlichenEntscheidungen. Allgemeinmedizin 1985; 14:149.
- Rogers A, Hassel K and NicolaasG. Demanding Patients? Analysing the use of primary care. Buckingham, Philadelphia: Open University Press, 1999, pp. 39–45.
- Shah P, Mayer R and Hegarty M. Graphs as aids to knowledge construction. Journal of Educational Psychology 1999;91:690–702.
- Custers EJ, Stuyt PM and De VriesRobbe PF. Clinical problem analysis (CPA): a systematic approach to teaching complex medical problem solving. Academic Medicine 2000;75:291–7.
- Van der Weijden T, van VM, Dinant GJ, van HasseltCM and Grol R. Unexplained complaints in general practice: prevalence, patients’ expectations, and professionals’ test-ordering behavior. Medical Decision Making 2003; 23:226–31.
- James P. Guidelines, clinical practice, and uncertainty: finding direction when the maps do not work. Journal of Family Practice 1999;48:669–70.
- Sonnenberg A.A medical uncertainty principle. American Journal of Gastroenterology 2001;96:3247–50.
- Andre´ M, Borgquist L, FoldeviMandMolstad S. Asking for ‘rules of thumb’: a way to discover tacit knowledge in general practice. Family Practice 2002;19:617–22.
- Baerheim A. The diagnostic process in general practice: has it a two-phase structure? Family Practice 2001;18: 243–5.
- Elstein AS and Schwartz A. Clinical problem solving and diagnostic decision making: selective review of the cognitive literature. BMJ 2002;324:729–32.
- Gigerenzer G. The psychology of good judgment: frequency formats and simple algorithms. Medical Decision Making 1996;16:273–80.
- Kee F, Jenkins J, McIlwaine S, Patterson C, Harper S and Shields M. Fast and frugal models of clinical judgment in novice and expert physicians. Medical Decision Making 2003;23:293–300.
- Tversky A and Khaneman D. Advances in prospect theory: cumulative representation of uncertainty. Journal of Risk and Uncertainty 1992;5:297–323.
- Scho¨n D.The Reflective Practitioner. New York: Basic Books, 1983, p. 128.
- Arborelius E, Bremberg S and Timpka T. What is going on when the general practitioner doesn’t grasp the situation? Family Practice 1991;8:3–9.
- Landstro¨m B, Mattsson B and Rudebeck CE.Attributes of competence – on GPs’ work performance in daily practice. Scandinavian Journal of Public Health 2009; 37:598–603.
- Wulff HR.The inherent paternalism in clinical practice. Journal of Medical Philosophy 1995;20:299–311.
- Kunseler E. Towards a New Paradigm of Science in Scientific Policy Advising. NUSAP: the management of uncertainty and quality in quantitative information. 2007. www.nusap.net/download.php?op=getit&lid=44 (accessed 15 September 2009).
- Giampietro M, Allen T and Mayumi K. Science for governance: the implications of the complexity revolution. In: Guimaraes PA, Guedes VS and Tognetti S Dealing with uncertainty in general practice: an essential skill for the general practitioner 181 (eds). Interfaces Between Science and Society. Sheffield: Greenleaf Publishing Ltd, 2006, pp. 7–22.
- BursztajnHj, Feinbloom RI, HammRMand Brodsky A. Medical Choices, Medical Chances; how patients families and physicians can cope with uncertainty. Lincoln, NE: iUniversity Press, 2000, pp. 54–84.
- Ghosh AK. On the challenges of using evidence-based information: the role of clinical uncertainty. Journal of Laboratory and Clinical Medicine 2004;144:60–4.
- Meyer LD, Hodgkinson AR, Knight R, Ho MT, di Corp and Bhalla S. Graduate capabilities for health service managers: reconfiguring health management education @UNSW. Australian Health Review 2007;31:379–84.
- Richardson M and Schneller ES.Out of the box: health management education in the 21st century. Journal of Health Administration Education 1998;16:87–97.
- Graber ML. Educational strategies to reduce diagnostic error: can you teach this stuff? Advances in Health Sciences Education 2009;14:63–9.
- Graber ML, Franklin N and Gordon R. Diagnostic error in internal medicine. Archives of Internal Medicine 2005; 165:1493–9.
- Kuhn GJ.Diagnostic errors. Academic Emergency Medicine 2002;9:740–50.
- Chalmers I. Well informed uncertainties about the effects of treatments. BMJ 2004;328:475–6.
- Ogden J, Fuks K, Gardner M et al. Doctors’ expressions of uncertainty and patient confidence. Patient Education and Counseling 2002;48:171–6.
- Innes AD, Campion PD and Griffiths FE. Complex consultations and the ‘edge of chaos’. British Journal of General Practice 2005;55:47–52.
- Stacey RD. Complexity and Creativity in Organizations. San Francisco: Berrett-Koehler Publishers, 1996, pp. 72– 106.
- Malterud K. Symptoms as a source of medical knowledge: understanding medically unexplained disorders in women. Family Medicine 2000;32:603–11.
- Salmon P. Patients who present physical symptoms in the absence of physical pathology: a challenge to existing models of doctor–patient interaction. Patient Education and Counseling 2000;39:105–13.

