Keywords
Critical Illness; Debridement; Pancreatitis, Acute
Necrotizing; Pancreatitis ; surgery; Treatment Outcome
Abbreviations
AP acute pancreatitis; ANC acute necrotic collection;
APACHE II acute physiology and chronic health evaluation II; DCD
damage control débridement; DCL damage control laparotomy; ERCP
endoscopic retrograde cholangiopancreatography; ICU intensive care
unit; INR international normalized ratio; NP necrotizing pancreatitis;
SAP severe acute pancreatitis; SSD single staged débridement, WON
walled off necrosis
INTRODUCTION
Acute pancreatitis (AP) is a local and systemic
inflammatory disease process responsible for greater
than 275,000 United States hospital admissions per year
[1, 2]. The spectrum of AP severity varies widely. Most AP
patients develop a mild and self-limited course requiring
a short hospital stay; however, others experience multiple
organ failure, severe sepsis, and a protracted hospital
course. Severe acute pancreatitis (SAP) is frequently complicated with infection, need for intervention, multiple
organ support, severe physical deconditioning and
frequent readmissions. Up to 15-25% of all SAP patients
develop necrotizing pancreatitis, with mortality rates in
this subgroup as high as 30% [3]. Necrotizing Pancreatitis
(NP) is defined as a non-enhancing area of pancreatic
parenchyma on contrast-enhanced CT imaging, best
visualized after the first week of the disease [4]. Infection
of pancreatic necrosis or failure to improve in the absence
of infection are the two indications for intervention in
NP [5].
In the last decade, the “step-up approach” has become
the standard of care in patients with pancreatic necrosis
requiring intervention. With failure of more conservative
management, the treatment is then “stepped-up.” This
approach begins with percutaneous drainage, advances to
endoscopic or video-assisted débridement, with surgical
débridement reserved for those patients failing less
invasive measures [6]. Thus, in current practice, those
NP patients undergoing operative débridement have not
improved or resolved with less invasive means and are the
sickest of NP patients. These patients undergo operative
débridement with historically high perioperative mortality
rates, ranging from 5-40% [7, 8, 9, 10]. Despite advances
in technique and critical care, mortality with débridement remains high, likely related to the fact that open pancreatic
débridement is reserved for the most challenging situation.
Damage control laparotomy (DCL) has become a widely
accepted practice in trauma surgery [11]. In DCL, the
surgeon rapidly corrects the underlying pathology in short
fashion, and expeditiously transfers the patient from the
operating room to the intensive care unit for appropriate
resuscitation and correction of metabolic disturbances.
After goals of resuscitation have been achieved, the
patient is taken back to the operating room for definitive
care under more favorable physiologic circumstances.
In our high volume clinical pancreatic surgery practice,
we have begun to apply the principle of DCL selectively
to the most severely ill NP patients requiring operative
débridement. Thus, damage control débridement (DCD)
is a staged approach to operative pancreatic débridement.
The decision to pursue this technique is based on the
clinical judgment of an experienced pancreatic surgeon
intra-operatively, taking into account the patient’s
unique, individual circumstance. Similar to DCL, the major
indications guiding the decision to proceed with DCD are
hemodynamic instability, medical coagulopathy, acidosis,
hypothermia, or a combination of these factors. After a 10-
year experience, we sought to critically evaluate outcomes
associated with this technique.
METHODS
Patient Population
Our institutional necrotizing pancreatitis database is
a prospectively collected database beginning with patient
data from 2006. The database includes all necrotizing
pancreatitis patients treated at our institution’s University
Hospital, regardless of management strategy. Among the
539 patients treated between 2006 and 2016, 356 patients
underwent open pancreatic débridement. 75 patients were
identified who underwent open pancreatic débridement
by a single, experienced pancreatic surgeon. Twelve of the
75 patients underwent DCD. The remainder underwent
traditional single stage débridement (SSD).
Diagnosis of Necrotizing Pancreatitis
Acute pancreatitis is defined according to the revised
Atlanta classification as published in 2012 [4]. Patients
met criteria if they had two or more of the following
three features: “typical” acute onset epigastric abdominal
pain radiating to the back, serum amylase/lipase level
of greater than three times the upper limit of normal, or
characteristic findings of acute pancreatitis on abdominal
cross-sectional imaging studies. Severe acute pancreatitis
is defined as AP with persistent organ failure (>48
hours), or local complication of acute peripancreatic fluid
collection or acute necrotic collection [4].
Organ failure was defined according to the Modified
Marshall scoring system for organ dysfunction: PaO2:FiO2 ratio of <300 defined respiratory failure; serum creatinine
>1.9 mg/dL or 2 times baseline creatinine defined renal
failure; and systolic blood pressure of <90 mmHg after fluid resuscitation or need for vasoactive agents defined
cardiovascular failure [4].
Necrotizing pancreatitis is defined as parenchymal
necrosis and/or peripancreatic necrosis represented as
lack of pancreatic parenchymal enhancement and/or
findings of acute necrotic collection (ANC) or walled off
necrosis (WON) on contrast-enhanced imaging [4].
Necrosis Intervention
Treatment strategy of all patients with NP focuses on
supportive care and avoids intervention of pancreatic
necrosis, if possible. Indications for intervention
on pancreatic necrosis in this study mirror those
now published by the International Association of
Pancreatology and the American Pancreatic Association
[5]. The decision to pursue operative débridement is
always made in consultation with the multi-disciplinary
team, which includes medical pancreatologists, pancreatic
endoscopists, interventional radiologists, and pancreatic
surgeons. Whenever possible, intervention is delayed at
least 4 weeks to allow maturation of the acute necrotic
collection into walled off necrosis; operation is only
performed earlier in the event of emergency, such as
ischemic bowel, perforated viscus, or hemorrhage. At the
time of operation, all patients, regardless of operative
strategy, receive perioperative antibiotics within sixty
minutes of incision, which are re-dosed as appropriate.
Patients with documented infected necrosis based on
intraoperative cultures are given a 7 to 10-day course of
antibiotics postoperatively (after source control).
Damage Control Débridement
Decision to pursue DCD was based on the following
intraoperative findings: hemodynamic instability
requiring increasing doses of vasoactive medications or
persistent acidosis despite volume resuscitation, medical
coagulopathy that was clinically obvious during the operation,
persistent hypothermia despite active rewarming efforts, or a
combination. The primary goal of a damage control operation
was to achieve maximal débridement prior to reaching an
indicated endpoint, as above.
While débridement must be tailored to the individual
patient with NP (based on anatomic distribution,
parenchymal involvement, and individual clinical scenario),
our general principals are as follows. Necrosis tracking
down the paracolic gutters is approached from lateral to
medial to allow safe access into the retroperitoneum. Lesser
sac necrosis is approached after dividing the gastrocolic
ligament. Débridement is performed manually (surgeon’s
fingers) or with a ring forceps, taking only the necrosis that
is freely mobile. Each field is debrided individually and
packed with lap sponges while proceeding to the next field.
Oozing from the inflamed surfaces is common and is often
controlled with packing alone. Finally, vigorous irrigation
helps to dislodge the necrosis.
At termination of damage control débridement, an
open abdomen negative pressure therapy system was applied, and the patient was transported to the ICU setting
for ongoing resuscitation and care. Once stabilized, one to
three days later, the patient returned to the operating room
for the next staged débridement. Following successful
débridement of all necrotic tissue, wide closed-suction
drains were placed, and the patient’s fascia was closed
primarily or with vicryl mesh.
Data and Statistical Analysis
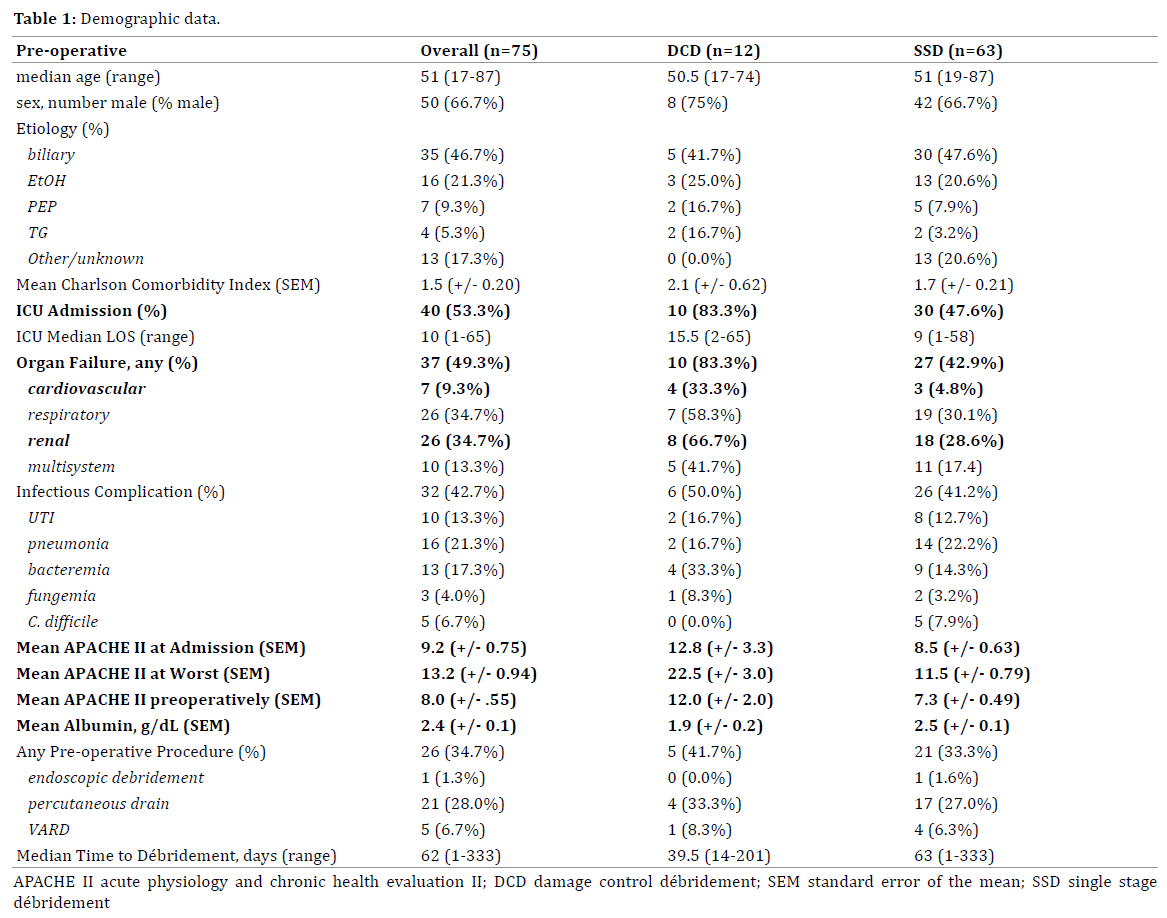
Individual demographic and clinical data were
recorded, including: age, sex, Charlson co-morbidity
index, and etiology (Table 1). Data regarding the
patient’s clinical course were evaluated pre-, peri-, and
post-operatively. Pre-operative data points included:
APACHE II score at admission, worst, and immediately
pre-operatively; cardiovascular, respiratory, and renal
organ system failure; infectious complications including
urinary tract infection, bacteremia, fungemia, pneumonia,
and C. difficile colitis; need for ICU admission and duration;
pre-operative INR, albumin, and total bilirubin; preoperative
means of management and number of days
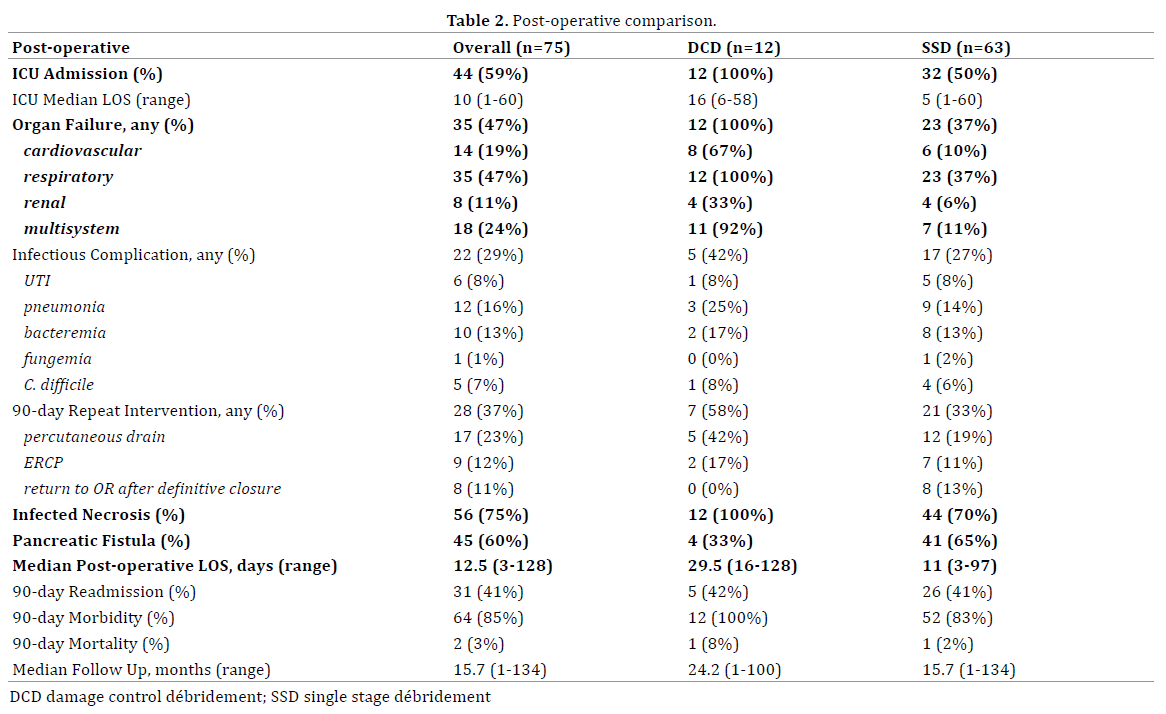
from diagnosis until operation. Peri- and post-operative
data points included: pH, base excess, and temperature
at worst and at the conclusion of the operation, organ
failure, infectious complications, need for ICU admission and duration, pancreatic fistula, need for re-intervention,
discharge disposition, readmission, duration of follow-up,
and mortality.
The aim of this review is to evaluate a novel technique
used in the most severely ill NP patients. As such,
outcomes are not compared statistically as this is purely
a descriptive discussion. A cohort of only 12 patients does
not allow sufficient power in the study group to objectively
compare outcomes. Instead, SSD is used as a baseline to
establish the inherent high morbidity associated with the
disease, particularly those patients that require operative
débridement. This point of reference highlights the
extreme severity of illness in those patients requiring a
staged approach to débridement.
Ethics
Data were compiled and reported in strict compliance
with patient confidentiality protocols set forth by the
Health Care Accountability and Portability Act (HIPAA)
and our Institutional Review Board (IRB), which approved
the conduct of this study. This work has been reported in
line with the STROCSS criteria [12]. Written or oral consent
were obtained from each patient and the study protocol
conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki – Ethical Principles for
Medical Research Involving Human Subjects [13].
RESULTS
Population Characteristics
In 75 patients undergoing open pancreatic débridement,
median age was 51 years (range 17-87). Fifty- (67%) patients
were male and 25 (33%) patients were female. Etiology
of AP was: biliary (47%), alcohol (21%), post-ERCP (5%),
hypertriglyceridemia (5%), and other/idiopathic (17%).
Average Charlson Comorbidity Index was 1.5 (+/- 0.2).
Preoperatively, surgical ICU admission was required in 40
(53%) patients, and 37 (49%) had developed organ failure
(26 respiratory failure, 26 renal failure, 7 cardiovascular
failure, and 10 with multi-system organ failure). Mean
APACHE II score was measured at admission (9.2 +/- 0.8),
worst (13.2 +/- 0.9), and pre-operatively (8.0 +/- 0.6).
Overall, 26 (35%) underwent a pre-operative procedure (21
percutaneous drainage, 5 endoscopic débridement, 1 videoassisted
retroperitoneal débridement). Infected necrosis
was documented by intraoperative cultures in 56 (75%)
patients. Median time to débridement was 62 days (range
1-333). Indications for DCD were hemodynamic compromise
(4, 33%), medical coagulopathy (4, 33%), or both (4, 33%).
Median follow up was 27.6 months (range 1-134) (Table 1).
Comparison of Groups (DCD vs. SSD)
Groups were similar in mean age (DCD 50.5 vs. SSD
51), sex (75% vs. 67% male), and etiology (biliary 42% vs. 48%, alcohol 25% vs. 21%, post-ERCP 17% vs. 8%,
hypertriglyceridemia 17% vs. 3%, or other 0% vs. 21%).
Patients treated by DCD were more severely ill globally
as evidenced by increased need for ICU admission (83% vs. 48%), incidence of organ failure (83% vs. 43%), preoperative
APACHE II score (12.0 vs. 7.3), and malnutrition
(albumin 1.9 vs. 2.5 g/dL) (Figure 1).
Figure 1. Preoperative APACHE II score and albumin displaying the severity of illness and malnutrition in the damage control débridement group.
Intra-operatively, base excess at worst was lower
in DCD patients (DCD -3 +/- 2.4 vs. SSD 0.5 +/- 1.9). The
median number of planned débridements was 2.5 (range
2-4). Primary fascial closure was performed in eight
patients (75%), while the remaining four (25%) required
fascia approximation with vicryl mesh.
Post-operatively, DCD patients had a higher incidence
of need for ICU admission (100% vs. 50%) and organ
failure (100% vs. 37%). Organ failure was more prevalent
in all aspects: respiratory (100% vs. 37%), renal (33% vs.
6%), cardiovascular (67% vs. 10%) and multisystem (92% vs. 11%).
The incidence of post-operative infectious
complications was similar: any (42% vs. 27%), pneumonia
(25% vs. 14%), bacteremia (17% vs. 13%), urinary tract
infection (8% vs. 8%), C. difficile (8% vs. 6%), or fungemia
(0% vs. 2%). Additionally, the need for post-operative
repeat intervention were similar: any (58% vs. 33%),
percutaneous drain (42% vs. 19 %), ERCP (17% vs. 11%), or
return to OR after definitive closure (0% vs. 13%). Median
post-operative length of stay was longer in the DCD group
(30 vs. 11 days). However, DCD and SSD had similar 90-
day readmission (42% vs. 41%), 90-day morbidity (100% vs. 83%), and 90-day mortality (8% vs. 2%) (Table 2).
DISCUSSION
Necrotizing pancreatitis patients requiring operative
débridement have a protracted hospital course with
a high degree of acute illness complicated by organ
failure, infection, and malnutrition. As our treatment
practices have changed over the last several years, NP
patients treated at our quaternary care center often
undergo pancreatic débridement as the definitive step
in the modern algorithmic approach. However, despite
unfavorable operative circumstances, we have reported
acceptable morbidity and mortality in patients undergoing
operative pancreatic débridement [14]. As critical care and
minimally invasive techniques improve survival following
the initial NP insult, more chronically and critically ill NP
patients are undergoing operative débridement. Thus,
there has become a need for new methods of open pancreatic
débridement to salvage these critically ill patients with
acceptable morbidity and mortality (Figure 2).
Figure 2. Similar rates of readmission, morbidity, and mortality between the damage control débridement and single stage débridement groups.
In 2010, the Dutch Pancreatitis Study Group published
a landmark paper describing the “step-up” approach in
managing NP requiring intervention. This randomized
controlled trial compared the traditional gold standard of
open pancreatic débridement to the “step-up” approach: percutaneous drainage, followed, if necessary, by
minimally invasive retroperitoneal necrosectomy. The
“step-up” approach was associated with decreased major
complications or death and long-term complications and
obviates the need for operative intervention in 30% of
patients. This approach has been validated and is now
advocated as the standard of care [15]. Our center has seen
a similar evolution in our practice over the past 10 years
[16]. In the current study, only 35% of patients underwent
a minimally invasive procedure as the initial step in
management. The time-period of the study spans a decade
of significant evolution in the management of NP. Between
2006 and 2010, operative management was applied more
frequently. This evolved into the step-up approach in the
patients treated between 2011-2016. During this latter
time period, more patients were treated initially with
percutaneous or endoscopic therapy [17]. As such, in the modern treatment algorithm, operative débridement is
now reserved for patients refractory to percutaneous
and/or endoscopic therapy. Some of these patients do
not have the physiologic reserve to undergo satisfactory
débridement in a single operation and may represent a role
for a staged-approach in the modern treatment algorithm
for the most severely ill NP patient.
Damage control laparotomy dates to the early 1900s,
with management of liver injuries by gauze packing and
open drainage [18]. Although abandoned following the
early 1900s, it was resurrected by the Detroit Receiving
group in 1976 [19] and gained further interest following
description of survival in 9 out of 10 patients undergoing
perihepatic packing following major hepatic injuries
[20]. Widespread acceptance began by the mid 1980s as
Feliciano and colleagues described “rapid conservative operative technique” in a large volume study with
improved outcomes [21]. Over the next 20 years,
technique was honed and studies continued to validate the
practice in a select population of patients with traumatic
injuries requiring laparotomy [11]. Thus DCL is accepted
as a “rational approach to an apparently hopeless situation
[22].” Damage control techniques have been applied to
pancreatic surgery, but have not been reported to date for
pancreatic débridement [23].
Resolution of NP often takes greater than 6 months,
multiple procedures, several readmissions, and is
associated with high morbidity. NP has profound
systemic effects including organ failure, infection, severe
malnutrition, and physical deconditioning. The mean
worst APACHE II score in our study was 16.8, which carries
a predicted mortality of 25% [24]. Pre-operatively, 49% of
patients developed organ failure, with 21% having multiple
organ failure. Infection was widely prevalent: 43% were
treated pre-operatively for an infectious complication.
The inflammatory response severely effects nutrition as
evidenced by a mean pre-operative albumin of 2.4 mg/dL.
27% of patients surviving to discharge required placement
into a facility for ongoing rehabilitation and care, and
those going home almost ubiquitously required outpatient
nursing and rehabilitation services. The physiologic
consequence of this systemic disease is devastating and far
from the ideal operative scenario.
Given the “stacked-deck” against the surgeon,
application of damage control laparotomy to open
pancreatic débridement seems logical. Historically, multidébridement
approaches to NP have been described.
In 1987, Bradley described a technique of operative
debridement followed by open abdominal packing and
healing by secondary intent [25]. While this laparostomy
technique improved mortality, compared to contemporary
standards, morbidity was significant with high rates of
intestinal fistula and 100% hernia rate. Sarr et al described
an approach with planned re-laparotomy in 1991
[26]. This “zipper” technique also improved morality;
however, the majority of patients underwent greater
than five operations, closure of the abdominal wound was
infrequently performed, and fistula rates were remarkably
high.
Damage control débridement, as described in the
current report, represents a combination of historical
approaches to pancreatic débridement, with the addition
of modern trauma principles based on physiology. DCD
is a staged approach aimed to accomplish complete
débridement, achieve wound closure, and limit the
physiologic insult by terminating operations based on
physiologic derangement. Decision to pursue DCD was
based on the intraoperative findings; however, some preoperative
indices may suggest which patients benefit from
DCD, such as pre-operative APACHE II score, albumin, and
organ failure. Ultimately, decision to pursue DCD is based
on pre-operative indices combined with intraoperative
findings, but importantly the ability of an experienced pancreatic surgeon to critically judge the global picture of
the individual patient.
This review of our experience with damage control
débridement was not intended to compare a novel
technique to a single stage débridement, but instead use
the single stage group as a point of reference. No matter
the technique, patients requiring operative débridement
traditionally have high morbidity and mortality. Our
experience with operative débridement and the postoperative
care of NP patients is extensive; as a result,
the overall cohort has a remarkably low mortality of
4%. Patients undergoing an operative débridement are
incredibly acutely ill, and the subset of patients requiring
a damage control débridement are the most severely ill
of this patient population. A damage control approach to
these patients offers definitive operative therapy with
similar morbidity and mortality to those undergoing
traditional operative débridement despite significantly
increased severity of illness.
Limitations to this study are clear. While data is obtained
prospectively, the study was evaluated retrospectively.
Similar to trauma DCL, application of DCD is at the
discretion of the surgeon and not randomized based on
quantitative data; refinement of discrete indices for DCD
are needed. This study is underpowered to perform a
comparative univariate or multivariate analysis with a
sample size of 12 patients. However, the intent was not
to report the superiority of DCD, but instead to display its
feasibility compared to our reference patients undergoing
single staged débridement.
Moving forward, development of a necrotizing
pancreatitis severity index may help guide the decision
to pursue a damage control approach. Indices could
include: active sepsis, malnutrition, organ failure,
APACHE II score, and close intraoperative monitoring
for acidosis, need for vasoactive agents, coagulopathy,
and hypothermia.
CONCLUSION
A select percentage of NP patients are so severely ill
that a definitive open débridement cannot be tolerated in
a single operation. In these patients a staged approach is
required. Damage control débridement proved to be a very
effective approach in the “sickest of the sick.” Use of this
staged approach to débridement may improve outcomes
for select, critically ill necrotizing pancreatitis patients
who require open débridement.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Fagenholz PJ, Fernandez-del Castillo C, Harris NS, Pelletier AJ, Camargo
CA Jr, et al. Direct medical costs of acute pancreatitis hospitalizations in
the United States. Pancreas 2007; 35:302-7. [PMID: 18090234]
- Peery AF, Dellon ES, Lund J, Crockett SD, McGowan CE, Bulsiewicz WJ,
et al. Burden of gastrointestinal disease in the United States: 2012 update.
Gastroenterology 2012; 143:1179-87 e3. [PMID: ]
- Kokosis G, Perez A, Pappas TN. Surgical Management of Necrotizing
Pancreatitis: An Overview. World J Gastroenterol 2014; 20:16106-12.
[PMID: 25473162]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG,
et al. Classification of acute pancreatitis--2012: revision of the Atlanta
classification and definitions by international consensus. Gut 2013;
62:102-11. [PMID: ]
- Working Group IAP/APA Acute Pancreatitis Guidelines. IAP/APA
evidence-based guidelines for the management of acute pancreatitis.
Pancreatology 2013; 13(4 Suppl 2):e1-15. [PMID: 24054878]
- van Santvoort HC, Besselink MG, Bakker OJ, Hofker HS, Boermeester MA,
Dejong CH, et al. A step-up approach or open necrosectomy for necrotizing
pancreatitis. N Engl J Med 2010; 362:1491-502. [PMID: 20410514]
- Rau B, Bothe A, Beger HG. Surgical treatment of necrotizing
pancreatitis by necrosectomy and closed lavage: changing patient
characteristics and outcome in a 19-year, single-center series. Surgery
2005; 138:28-39. [PMID: 16003313]
- Madenci AL, Michailidou M, Chiou G, Thabet A, Fernández-del Castillo
C, Fagenholz PJ, et al. A contemporary series of patients undergoing open
debridement for necrotizing pancreatitis. Am J Surg 2014; 208:324-31.
[PMID: 24767969]
- Wormer BA, Swan RZ, Williams KB, Bradley JF 3rd, Walters AL,
Augenstein VA, et al. Outcomes of pancreatic debridement in acute
pancreatitis: analysis of the nationwide inpatient sample from 1998 to
2010. Am J Surg 2014; 208:350-62. [PMID: 24933665]
- Banks PA, Freeman ML, Practice Parameters Committee of the
American College of Gastroenterology. Practice guidelines in acute
pancreatitis. Am J Gastroenterol 2006; 101:2379-400. [PMID: 17032204]
- Roberts DJ, Ball CG, Feliciano DV, Moore EE, Ivatury RR, Lucas CE, et al.
History of the Innovation of Damage Control for Management of Trauma
Patients: 1902-2016. Ann Surg 2017; 265:1034-44. [PMID: 27232248]
- Agha R, Borrelli M, Vella-Baldacchino M, Thavayogan R, Orgill DP;
STROCSS Group. The STROCSS Statement: Strengthening the Reporting of
Cohort Studies in Surgery. Int J Surg 2017; 46:198-202. [PMID: 28890409 ]
- Association WM. World Medical Association Declaration of Helsinki:
Ethical Principles for Medical Research Involving Human Subjects. JAMA
2013; 310:2191-4. [PMID: 24141714]
- Howard TJ, Patel JB, Zyromski N, Sandrasegaran K, Yu J, Nakeeb A, et
al. Declining morbidity and mortality rates in the surgical management of
pancreatic necrosis. J Gastrointest Surg 2007; 11:43-9. [PMID: 17390185]
- Freeman ML, Werner J, van Santvoort HC, Baron TH, Besselink MG,
Windsor JA, et al. Interventions for Necrotizing Pancreatitis: Summary of
a Multidisciplinary Consensus Conference. Pancreas 2012; 41:1176-94.
[PMID: ] [PMID: 23086243]
- Roch AM, Maatman T, Carr RA, et al. Evolving treatment of necrotizing
pancreatitis. Am J Surg 2018; 215:526-9. [PMID: ]
- Roch A, Maatman T, Carr R, Easler JJ, Schmidt CM, House MG, et al.
Evolving treatment of necrotizing pancreatitis. Am J Surg 2018; 215:526-
9. [PMID: 29167024]
- Tilton BT. Some Considerations Regarding Wounds of the Liver. Ann
Surg 1905; 41:20-30. [PMID: 17861585]
- Lucas CE, Ledgerwood AM. Prospective Evaluation of Hemostatic
Techniques for Liver Injuries. J Trauma 1976; 16:442-51. [PMID: 778397]
- Feliciano DV, Mattox KL, George JL. Intra-abdominal Packing for
Control of Hepatic Hemorrhage: A Reappraisal. J Trauma 1981; 21:285-
90. [PMID: 7012380]
- Feliciano DV, Burch JM, Spjut-Patrinely V, Mattox KL, Jordan GL Jr.
Abdominal gunshot wounds. An urban trauma center's experience with
300 consecutive patients. Ann Surg 1988; 208:362-70. [PMID: 3421760]
- Burch JM, Ortiz VB, Richardson RJ, Martin RR, Mattox KL, Jordan GL Jr.
Abbreviated Laparotomy and Planned Reoperation for Critically Injured
Patients. Ann Surg 1992; 215:476-83. [PMID: 1616384]
- Morgan K, Mansker D, Adams DB. Not just for trauma patients:
damage control laparotomy in pancreatic surgery. J Gastrointest Surg
2010; 14:768-72. [PMID: 20224981]
- Knaus WA, Draper EA, Wagner DP, et al. APACHE II: A severity of
disease classification system. Crit Care Med 1985; 13:818-29. [PMID:
3928249]
- Bradley EL, 3rd. Management of Infected Pancreatic Necrosis by
Open Drainage. Ann Surg 1987; 206:542-8. [PMID: 3662663]
- Sarr MG, Nagorney DM, Mucha P Jr, Farnell MB, Johnson CD. Acute
Necrotizing Pancreatitis: Management by Planned, Staged, Pancreatic
Necrosectomy/Debridement and Delayed Primary Wound Closure Over
Drains. Br J Surgery 1991; 78(May):576-81. [PMID: 2059810]



