Keywords
Neoplasms, Cystic, Mucinous, and Serous; Pancreatic Cyst; Pancreatic Pseudocyst
INTRODUCTION
Cystic lesions of the pancreas, although rare, represent an important group as its proportion among the pancreatic tumors has increased in the last decades, with prevalence that ranges from 1% in the initial reports to up to 29% in some institutions [1, 2]. This increase is due mainly to the advances in diagnostic studies and surgical techniques that, in many cases, may be curative. As these advances keep changing the clinical approach of patients with pancreatic tumors and cysts, pathologists are better able to characterize the morphology and help to assess the potential behavior of this heterogeneous group of entities.
The increased detection of cystic lesions has also lead to the study of clinical and morphologic features that can help to distinguish between neoplastic and nonneoplastic processes and between benign and malignant cystic neoplasms. Malignant lesions are frequent even in asymptomatic patients [3]. A characterization of specific features for each entity may help to provide a more selective therapeutic approach and spare patients with benign conditions of the morbility and mortality associated with a surgical resection.
Our institution performs approximately 100 pancreatic resections each year, including Whipple procedures, total, central and distal pancreatectomies. In this study we characterize and subdivide the group of pancreatic cysts in our population analyzing the distribution of the different entities and comparing basic clinical and morphologic features associated with them.
PATIENTS
All the pancreatectomy specimens reported from July 2003 to May 2008 were extracted from our Data System (Misys CoPathPlus® v.2.4.2.131, Misys Healthcare Systems, Tucson, AZ, USA). Of 470 pancreatic lesions, 97 cysts (20.6% of the total) corresponding to 95 patients were studied. Sixty-four percent of the cases occurred in women. The mean age was 60.2 years (SD: 15.7 years; range: 16-84 years).
MATERIALS AND METHODS
Pertinent clinical information was extracted, including age, gender, location and size of the tumor, clinical presentation, results of radiologic images and characterization of the fluid when available. The histological material in all cases was retrieved and reviewed by two pathologists with expertise in the field of pancreatic pathology. Their diagnoses were based on the current WHO classification of tumors [4]. The cases were classified in groups: non-neoplastic and neoplastic (benign, borderline and malignant).
ETHICS
Approval by the Institutional Review Board was obtained prior to the study.
STATISTICS
Mean, standard deviation (SD), range, and frequencies were reported as descriptive statistics. The comparison between the observed and the expected frequencies was made by means of the hierarchical log-linear model. The age of the different diagnostic categories was compared with the overall mean by using the deviation contrast applied to the one-way ANOVA. The significance of association was calculated by means of the linear-by-linear association chi-square tests. Twotailed P values less than 0.05 were considered statistically significant. The Episet v.1.0 for Windows (Pontificia Universidad Javeriana, Bogota, Colombia) software was used to make the statistical analyses.
RESULTS
Fourteen different diagnoses were established. Ninetytwo cystic lesions (94.8%) were neoplastic: 58 (59.8%) were benign, 17 (17.5%) were borderline, and 17 (17.5%) were malignant (Table 1). Among the five non-neoplastic lesions, three were inflammatory pseudocysts (3.1% of the total), one corresponded to an enterogenous cyst and one to a squamoid cyst (1.0% each); these three patients with pancreatic pseudocyst presented without symptoms or predisposing factors for pancreatitis, and imaging showed a complex mass suggestive of a neoplastic process. Among the neoplastic lesions, only one had a mesenchymal origin (a cystic schwannoma), while all others were epithelial in origin. Intraductal papillary mucinous neoplasm (IPMN) was the most common entity (51 lesions; overall 52.6%, 55.4% of the 92 neoplastic lesions), followed by serous cystic neoplasms (20 lesions; overall 20.6%, 21.7% of the neoplastic lesions) and mucinous cystic neoplasms (13 lesions; 13.4% overall, 14.1% of the neoplastic lesions). In addition there were 6 solid pseudopapillary tumors (overall 6.2%, 6.5% of the neoplastic lesions) and one neuroendocrine cystic tumor (overall 1.0%; 1.1% of the neoplastic lesions). IPMN was categorized as benign (25/58, 43.1%), borderline (10/17, 58.8%) and malignant (2 noninvasive and 14 invasive lesions: 16/17, 94.1%), showing a significant increased frequency with increasing malignancy (P<0.001; linear-by-linear association chi-square test).
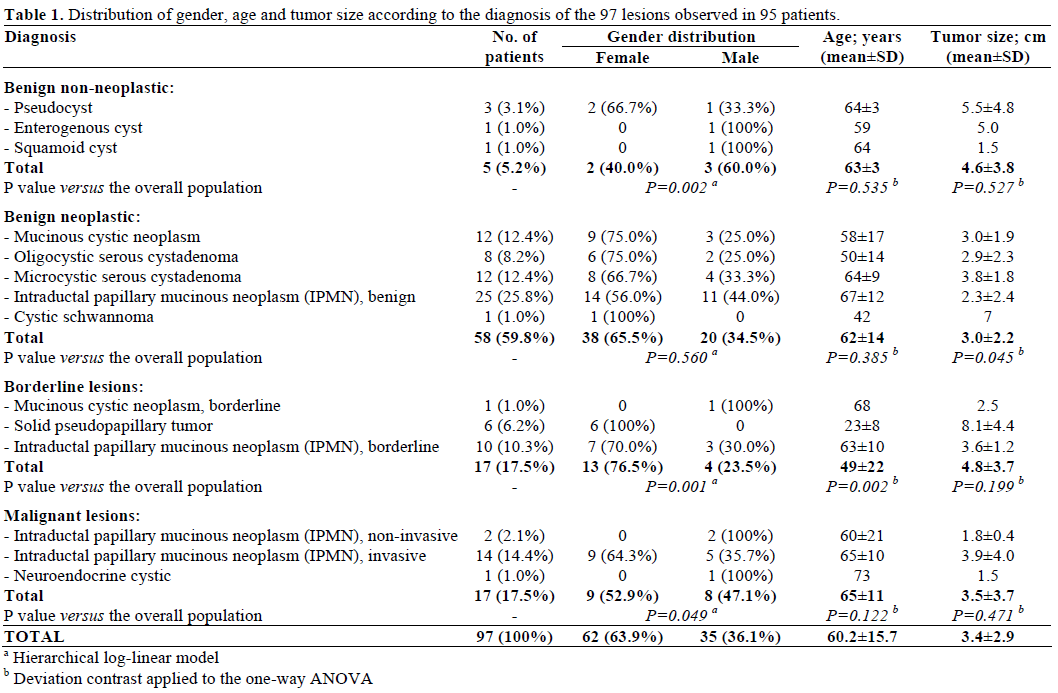
The distribution by gender, age and size of the tumor is shown in Table 1. The majority (63.9%) of these lesions was present in females: a significantly lower frequency of females was observed in non-neoplastic (40.0%, P=0.002) and malignant (52.9%, P=0.049) lesions while a significantly higher frequency of females was observed in borderline lesions (76.5%, P=0.001). Age was significantly lower in borderline
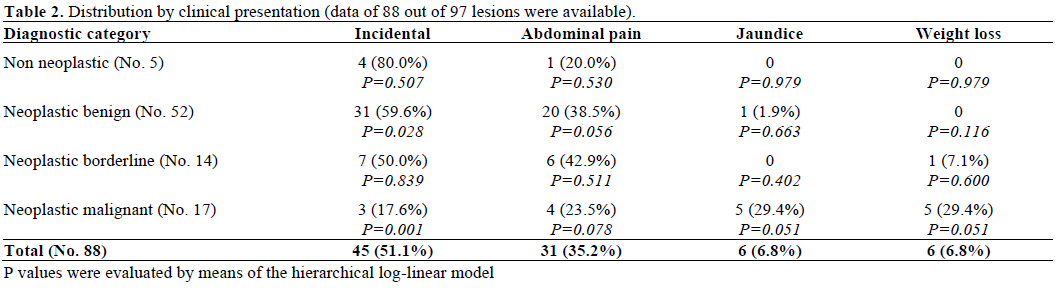
lesions (P=0.002); the benign neoplastic lesions had a significantly lower size (P=0.045) while borderline lesions were the largest ones (mean size 4.8±3.7 cm) but without reaching the statistical significance (P=0.199). The differences in gender, age and tumor size in the borderline category were mainly due to the 6 cases of solid pseudopapillary tumor (all females; average age: 23±8 years; average size: 8.1±4.4 cm). Table 2 shows the distribution of cases according to the clinical presentation, which was available in 88 cases (90.7%). The majority of the cases were identified incidentally by computed tomography (CT) or magnetic resonance (MRI) (45 cases, 51.1%). The most common clinical manifestation among the other patients was non-specific abdominal pain (31 cases, 35.2%). Less frequent manifestations include jaundice and weight loss (6 cases each, 6.8%). Interestingly, incidental identification of the lesions was significantly more frequent in neoplastic benign lesions (P=0.028) and significantly lower in malignant lesions (P=0.001); in particular, almost all the patients with jaundice and weight loss had a malignant lesion, but this association did not reach the significant level (P=0.051).
Results of preoperative radiologic studies were available for 65 patients (66 cystic lesions, 68.0%). Either by CT or MRI, 49 cases were described as complex cysts (75.4%), in 10 cases the mass was described as solid (15.4%) and the remaining 6 cases (9.2%) had a simple cyst.
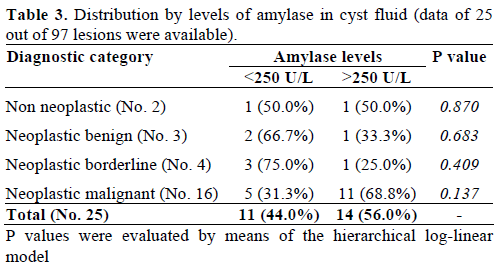
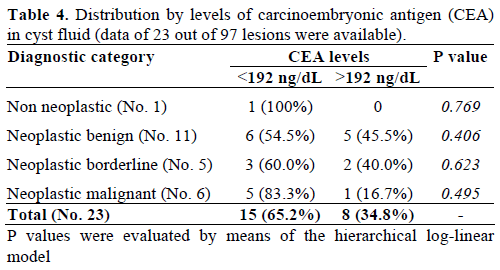
Preoperative amylase levels in the cystic fluid were available in 25 patients (25 cystic lesions, 25.8%; Table 3) while preoperative carcinoembryonic antigen (CEA) levels in cystic fluid were available in 23 patients (23 cystic lesions, 23.7%; Table 4). Cut-off values of 250 U/L and 192 ng/dL were chosen for dichotomizing cystic fluid amylase [5, 6] and CEA [5, 6, 7] levels, respectively. Eleven patients had an amylase level less than 250 U/L (44.0%) while only 8 patients had a CEA level greater than 192 ng/dL (34.8%). Both amylase and CEA cystic fluid levels did not correlate with any diagnostic category analyzed (Tables 3 and 4).
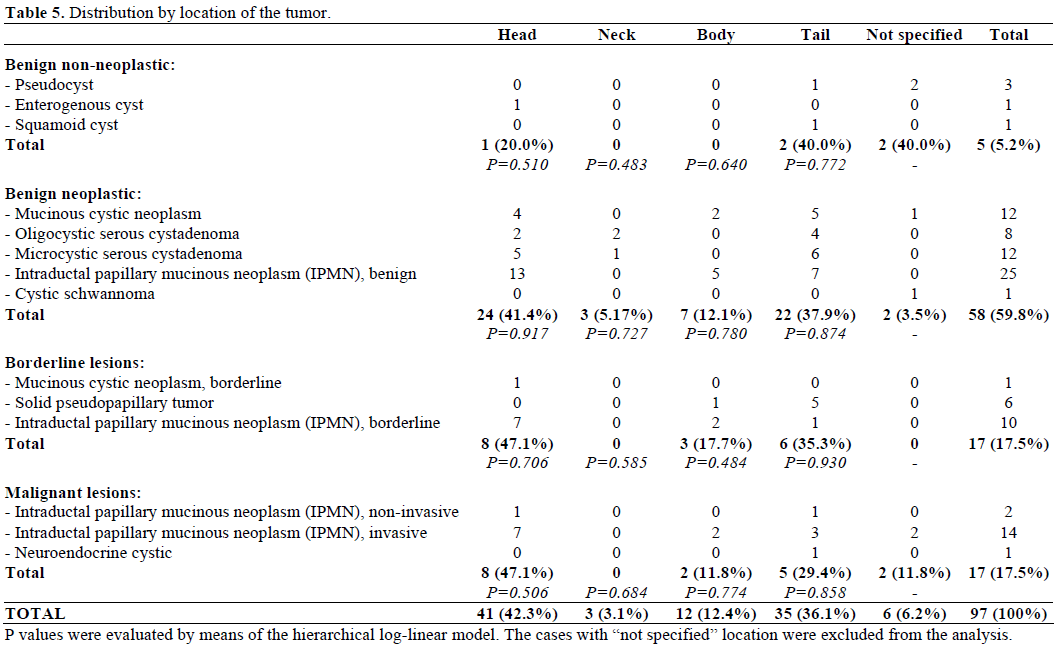
The distribution by location of the tumor is shown in Table 5. Non-neoplastic and neoplastic cystic lesions were found in all the anatomic parts of the pancreas, except for solid pseudopapillary tumor, which was found exclusively in the body or the tail. Overall, the most frequent locations in the pancreas were the head (42.3%) and tail (36.1%). There were no significant differences of the location among the four diagnostic categories.
Finally, two patients had two distinct lesions (one with two mucinous cystic neoplasms and one with two benign IPMNs). The lesions in these patients were grossly separated (1.0 and 9.0 cm in each case). Interestingly, none of our cases showed additional pathologic changes, such as pancreatitis.
DISCUSSION
In this retrospective study we analyzed 97 cystic lesions of the pancreas diagnosed in our institution in a five-year period. Our study is based on patients who underwent tumoral resection and did not include those cases where surgery was not performed. Therefore, our series may not be entirely representative of the whole population. Information about pre-operative work-up was not available for every case of the series, limiting the evaluation of clinical, radiologic and laboratory data. We observed, however, predominance of complex lesions in our series, and a possible association between weight loss or jaundice as the presenting symptom and diagnosis of a malignant neoplasm.
Approximately two-thirds of our cases were benign lesions, and only one-third was borderline or malignant, which suggest a high rate of unnecessary surgeries in our series that could have been avoided. This may reflect the limitations of the current diagnostic methods to accurately characterize pancreatic lesions pre-operatively. However, we observed that in the majority of the benign cases the diagnostic imaging revealed complex cysts and the clinical impression was that of neoplastic mucinous cyst with a risk of malignant transformation. In fact, the pathologic distribution corroborates this, since the majority of cases in the benign category were mucinous in nature. Mucinous lesions are considered to have a malignant potential and should be resected.
Among the heterogeneous group of non-neoplastic cystic lesions, inflammatory pseudocyst is the most frequent entity, accounting for approximately 75% of all pancreatic cysts [8, 9]. Previous references in the literature report a prevalence of 30% to 34% in surgical resection series [1, 2, 9]. Currently, however, the diagnosis of inflammatory pseudocyst is achieved clinically and its management is medical in most instances. This may explain the relatively low prevalence in our series (only 3% of the cases). Pseudocysts are more frequent in males and the age range is variable. Nonetheless, two of our three patients were female.
Other non-neoplastic lesions are even more infrequent. Othman et al. described six cases of pancreatic cysts with squamous lining surrounded by fibrous tissue lacking inflammation and ovarian-like stroma, and introduced the term “squamoid cyst of pancreatic ducts” [10]. One of our cases met the characteristics of a squamoid cyst (Figure 1 ab). This lesion appears to be reactive and corresponds to a cystic dilation of the pancreatic ducts with squamous metaplasia of the ductal epithelium.
Figure 1. Squamoid cyst of pancreatic ducts (H&E 200x: a). Immunohistochemistry for p63 (200x, b.). Intraductal papillary mucinous neoplasm,
benign (H&E: 100x, c.; 400x d.). Oligocystic serous cystic neoplasm (H&E: 400x, e.; 100x, f.). Periodic acid Schiff stain (100x, g.). Schwannoma
with cystic degeneration (H&E 100x: h. i.). Immunohistochemistry for S100 (100x, j.). Neuroendocrine carcinoma with cystic degeneration (H&E
100x: k.). Immunohistochemistry for chromogranin (100x, l.).
Enterogenous (congenital, duplication) cysts are very rare. They are seen mainly in infants and children as an uncommon cause of pancreatitis [9, 11]. It has been also reported in adults. We found one enterogenous cyst in our series (1%), measuring 5 cm, located in the head of the pancreas next to the ampulla in a 59-yearold man. Histologically, the cyst was lined by simple epithelium and surrounded by a double layer of smooth muscle.
Cysts with mucinous lining are particularly important due to their inherent malignant potential. Mucinous cystic neoplasms are common, representing 10% to 45% of all pancreatic cystic neoplasms [12]. Likewise, IPMN is reported to represent 21% to 33% of the cases [12]. In our study, the proportion of IPMN cases is higher, being the most frequent diagnosis (52.6%, Figure 1 cd) followed by mucinous cystic neoplasms (13.4%). Combined, mucinous cystic neoplasm and IPMN represent the majority of cases in our series (64 cases, 66.0%). Mucinous cystic neoplasms are almost exclusive of premenopausal women, with a mean age of 48 years and a male to female ratio less than 1:20; they are located predominantly in the tail of the pancreas [13, 14]. Women represented 100% of the cases in two of the largest series of mucinous cystic neoplasms reported [15, 16]. However, cases present in men have been recently described as case reports [17, 18] and in one single small series of 41 patients. In the latter, 8 of them (19.5%) were men [19]. In our series, 30.8% (4 of our 13 cases) occurred in men, and 5 were located in the pancreatic head.
Serous cystic neoplasms are lesions of variable size (up 25 cm) that represent 10% to 39% of all the cystic lesions in different series [12, 13]. The majority of serous cystic neoplasms are microcystic, and the macrocystic (oligocystic) variant is reported infrequently. Galanis et al. published the largest series of serous cystic neoplasms in a single institution; 75% of their patients were female and the mean age was 62.1 years [20]. In our study, serous cystic neoplasms account for 20.6% of the cases, affecting predominantly women (70%). The majority of them measured less than 5 cm in size. Interestingly, the proportion of oligocystic serous cystic neoplasms was higher than expected. We found 8 cases of oligocystic serous cystic neoplasm and 12 cases of microcystic serous cystic neoplasm (40% and 60%, respectively; Figure 1 efg). Kosmahl et al. reported 40 cases of serous cystic neoplasm with the same distribution, 24 cases (60%) of microcystic serous cystic neoplasm versus 16 cases (40%) of oligocystic serous cystic neoplasm [2].
Solid pseudopapillary tumor is included in the differential diagnosis of pancreatic cystic lesions because very commonly develops necrosis and cystic degeneration. This entity accounts for less than 10% of all cystic lesions of the pancreas and 1% to 3% of pancreatic neoplasms [1, 7, 12, 21]. However, Kosmahl et al. found a higher proportion of these cases, representing 21.2% of all cystic lesions [2]. In our study solid pseudopapillary tumor was seen in 6.1% of the cases. Solid pseudopapillary tumor is typically found in young female patients with a mean age of 25 to 28 years and a male to female ratio of 1:20 [1, 9]. Our findings correlate with these data, with all six cases being women (100%) and a mean age of 23 years. The size of the tumor is highly variable; being the mean size reported in the literature 9.3 cm [7]. In our study it was 8.1 cm. These lesions were larger than other neoplastic cysts. Solid pseudopapillary tumor is reported to be evenly distributed through the pancreas. However, all our cases were located in the body and tail of the gland (five of them in the tail, 83.3%). We included this entity in the borderline category because, despite the risk of recurrence and metastasis, most of the cases have an excellent prognosis after surgery.
More infrequent solid pancreatic tumors can have cystic degeneration. Pancreatic schwannoma is exceedingly rare with only 25 cases reported in the English literature [22]. These lesions occasionally undergo cystic degeneration. They have a size that ranges from 1.5 to 20 cm and [23]. We identified one case in our series. This tumor measured 7 cm and showed the typical histopathologic features, being positive for S100 and negative for keratin, CD34, cKit and calretinin by immunohistochemistry (Figure 1 hij). Neuroendocrine tumors of the pancreas represent only 1-2% of all tumors, and undergo cystic changes in only 10% of the cases [24]. Most of these lesions are nonfunctioning. The only case we observed was a 1.5 cm cystic lesion in the tail of the pancreas on a 73- year-old man (Figure 1 kl). Cystic neuroendocrine tumors are considered lesions with low malignant potential. However, our case represented a recurrence of a solid neuroendocrine tumor after a distal pancreatectomy where the tumor initially showed lymphovascular invasion, and therefore was classified as a malignant lesion.
Table 6 includes other cystic lesions of the pancreas not encountered in our series. These include duodenal diverticula, endometriotic cysts, lymphangiomas, lymphoepithelial cysts, cystic hamartomas and acinar cell carcinomas with cystic change, among others. Most of these entities are uncommon. Although frequent among pancreatic tumors, ductal adenocarcinomas rarely undergo cystic change [25]. In fact, we did not identify any in our series.
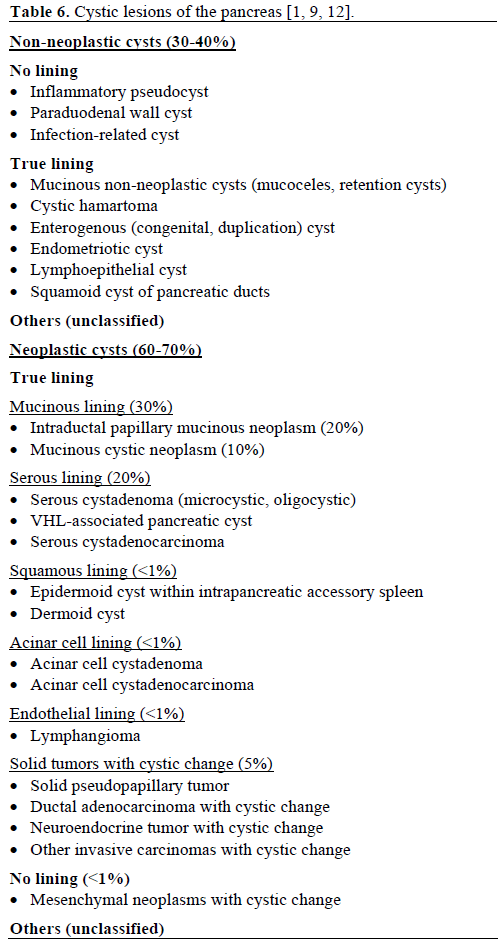
Table 6 also highlights the morphology-based diagnostic approach that we follow at our institution. The initial step is to determine if the cyst has a true lining or not. If it does the nature of the lining and features such as the underlying stroma, the cyst content and the relation with the pancreatic ducts will guide the pathologist to the specific diagnosis. Lesions with no true lining (pseudocysts, mesenchymal lesions) have also distinctive clinical and morphologic characteristics that are helpful in the diagnostic approach.
In conclusion, cystic lesions of the pancreas are diverse and may have a different presentation in different populations. We found a significant proportion of neoplastic lesions, especially mucinous cysts. We also found an association between clinical presentation and diagnosis, specially in cases diagnosed incidentally. Solid pseudopapillary tumor appears to be the only lesion with a consistent age at presentation, gender and tumor size. Other lesions showed significant variation of these characteristics, and their assessment may not be helpful in differentiating benign from malignant lesions. Clinical, radiologic and laboratory investigation should be consistently exercised in order to optimize the pre-operative diagnostic impression and determine the need of surgical intervention. This study reports interesting distributions and rare cases, and it may contribute to the further characterization of this complex group of entities.
Conflict of interest
The authors have no potential conflict of interest
References
- Adsay VN. Cystic lesions of the pancreas. Mod Pathol 2007; 20(Suppl 1):S71-93. [PMID 17486054]
- Kosmahl M, Pauser U, Peters K, Sipos B, Lüttges J, Kremer B,
Klöppel G. Cystic neoplasms of the pancreas and tumor-like lesions
with cystic features: a review of 418 cases and classification
proposal. Virchows Arch 2004; 445:168-8. [PMID 15185076]
- Garcea G, Ong SL, Rajesh A, Neal CP, Pollard CA, Berry DP, Dennison AR. Cystic lesions of the pancreas: a diagnostic and management dilemma. Pancreatology 2008; 8:236-51. [PMID 18497542]
- Klöppel G, Solcia E, Longnecker DS, Capella C, Sobin LH. Histological Typing of Tumours of the Exocrine Pancreas (WHO. World Health Organization. International Histological Classification of Tumours). Berlin, Heidelberg; Germany: Springer-Verlag; 2nd edition, 1996. [ISBN 978-3540602804]
- Van der Waaij LA, Van Dullemen HM, Porte RJ. Cyst fluid analysis in the differential diagnosis of pancreatic cystic lesions: a pooled analysis. Gastrointest Endosc 2005; 62:383-9. [PMID 16111956]
- Scheiman JM. Cystic lesion of the pancreas. Gastroenterology 2005; 128:463-9. [PMID 15685556]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology 2004; 126:1330-6. [PMID 15131794]
- Klöppel G. Pseudocysts and other non-neoplastic cysts of the pancreas. Semin Diagn Pathol 2000; 17:7-15. [PMID 10721803]
- Basturk O, Coban I, Adsay VN. Pancreatic cysts: pathologic classification, differential diagnosis, and clinical implications. Arch Pathol Lab Med 2009; 133:423-38. [PMID 19260748]
- Othman M, Basturk O, Groisman G, Krasinskas A, Adsay NV. Squamoid cyst of pancreatic ducts: a distinct type of cystic lesion in the pancreas. Am J Surg Pathol 2007; 3:291-7. [PMID 17255775]
- Hunter CJ, Connelly ME, Ghaffari N, Anselmo D, Gonzalez I, Shin C. Enteric duplication cysts of the pancreas: a report of two cases and review of the literature. Pediatr Surg Int 2008; 24:227-33. [PMID 18060413]
- Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C, Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med 2004; 351:1218-26. [PMID 15371579]
- Adsay VN. Cystic neoplasia of the pancreas: pathology and biology. J Gastrointest Surg 2008; 12:401-4. [PMID 17957438]
- Fernandez-Del Castillo C. Mucinous cystic neoplasms. J Gastrointest Surg 2008; 12:411-3. [PMID 17955316]
- Thompson LD, Becker RC, Przygodzki RM, Adair CF, Heffess CS. Mucinous cystic neoplasm (mucinous cystadenocarcinoma of low malignant potential) of the pancreas: a clinicopathologic study of 130 cases. Am J Surg Pathol 1999; 23:1-16. [PMID 9888699]
- Zamboni G, Scarpa A, Bogina G, Iacono C, Bassi C, Talamini G, et al. Mucinous cystic tumors of the pancreas: clinicopathological features, prognosis, and relationship to other mucinous cystic tumors. Am J Surg Pathol 1999; 23:410-22. [PMID 10199470]
- Kim JC, Kim MH, Lee TY, Kim JY, Han JH, Park SJ, et al. Clinicopathologic review of 41 cases of pancreatic mucinous cystic neoplasms. Korean J Gastroenterol 2008; 51:34-9. [PMID 18349560]
- Kobayashi T, Teruya M, Shimizu S, Miki K, Kobayashi K, Morita K. Mucinous cystic tumor of the pancreas in a man: a rare case. Pancreas 2006; 33:312-4. [PMID 17003656]
- Suzuki M, Fujita N, Onodera H, Kayaba Y, Suzuki S, Kagaya H, et al. Mucinous cystic neoplasm in a young male patient. J Gastroenterol 2005; 40:1070-4. [PMID 16322953]
- Galanis C, Zamani A, Cameron JL, Campbell KA, Lillemoe KD, Caparrelli D, et al. Resected serous cystic neoplasms of the pancreas: a review of 158 patients with recommendations for treatment. J Gastrointest Surg 2007; 11:820-6. [PMID 17440789]
- Papavramidis T, Papavramidis S. Solid pseudopapillary tumors of the pancreas: review of 718 patients reported in English literature. J Am Coll Surg 2005; 200:965-72. [PMID 15922212]
- Tafe LJ, Suriawinata AA. Cystic pancreatic schwannoma in a 46-year-old man. Ann Diagn Pathol 2008; 12:296-300. [PMID 18621000]
- Tan G, Vitellas K, Morrison C, Frankel WL. Cystic schwannoma of the pancreas. Ann Diagn Pathol 2003; 7:285-91. [PMID 14571430]
- Ballarin R, Masetti M, Losi L, Di Benedetto F, Di Sandro S, De Ruvo N, et al. Cystic pancreatic neuroendocrine neoplasms with uncertain malignant potential: report of two cases. Surg Today 2009; 39:162-7. [PMID 19198998]
- Adsay VN. Centrally necrotic invasive ductal carcinoma of the pancreas presenting clinically as macrocystic lesions. Mod Pathol 2001; 14:191A.


