Keywords
Vascular Resection; Whipple Procedure; Management; Pancreas; Malignancy; Adenocarcinoma
INTRODUCTION
Pancreatic cancer is the fourth leading cause of cancer death in the United States [1] with a 5-year overall survival (5-year-OS) of only 9-18 % [2]. Due to the late presentation of symptoms, only 10-20% of patients are candidates for curative resection (CR). Over 50% of patients have distant metastasis, and 35% have locally advanced disease at the time of diagnosis [3, 4]. Only 35% of patients who have locally advanced disease may benefit from a more radical surgery if an R-0 resection, where all post resection margins are tumor free, can be achieved. Complete surgical resection of a localized pancreatic cancer is the only curative treatment, and the 5-year-OS in this group of patients has been reported as high as 25% [5-8]. The initial enthusiasm for increasing resectability by regional pancreatectomy, in patients who have major vascular (arterial and venous) involvement, was proposed by Fortner in 1973 [9], but this technique has not resulted in a lower morbidity or improved patient survival since it is difficult to get R-0 resections in such patients. However, surgical management of patients with portal vein (PV) or superior mesenteric vein (SMV) tumor involvement has received more enthusiasm, and it has been claimed that it should no longer be considered as a contraindication for curative resections [10].
The Gastrointestinal Medical Oncology group of the University of Texas M. D. Anderson Cancer Center defined a group of locally advanced pancreatic tumors with major venous involvement as borderline resectable tumors [10]. There are several reports from larger centers with expertise in pancreatic surgery showing similar morbidity and long term survival rates between patients with locally advanced pancreatic cancer undergoing en bloc resection of PV/SMV in conjunction with pancreatoduodenectomy and patients who underwent a conventional pancreatoduodenectomy without vascular resections [2, 11-28]; however, others have questioned this approach [29-33]. The issue of major venous involvement due to tumor location, as opposed to biologic aggressiveness [34], was indirectly addressed by Illuminati et al. [3] when they resected venous involvement of < 2cm if they predicted an R-0 resection with good results. Others have shown similar results when limited vein resection and reconstruction have been performed [35, 36]. Experience with major arterial resection (celiac and/or superior mesenteric artery) and reconstruction is limited by poor outcomes [37]. Improvement in preoperative staging, surgical techniques and expertise, a multidisciplinary approach to patient selection, and perioperative care has led to a reduced morbidity and an improved 5-year-OS in high volume pancreatic centers [4, 13, 22, 32, 38, 39]. We are reporting our experience from a medium size center with extensive experience in hepatopancreato- biliary (HPB) surgery and transplantations of the liver and pancreas. In a group of patients with borderline to advanced pancreatic cancer, we compare the outcome of patients who underwent CR of the pancreas with venous resection and repair to patients who underwent CR but did not need vascular resection and reconstruction.
PATIENTS AND METHODS
Following IRB approval, we reviewed data from patients who underwent pancreatic surgery (n=274) by our team between February of 1998 and January of 2012. In 2003, expecting an improved overall survival, we began performing en bloc major venous resections in patients with borderline resectable pancreatic malignancies if we deemed an R-0 resection achievable. After initial work up, which included routine blood tests, tumor markers (CEA, CA19-9), and either positron emission tomography (PET) scan, pancreas protocol computed tomography (CT), magnetic resonance cholangio-pancreatography (MRCP), endoscopic retrograde cholangio-pancreatography (ERCP) and, more recently, endoscopic ultrasound scan (EUS), the patients were discussed by a multidisciplinary team of oncologists, oncology surgeons, gastroenterologists, interventional radiologists, and HPB surgeons. The presence of distant metastasis or involvements of celiac and superior mesenteric arteries by tumor infiltrate were considered as contraindications to curative resection. In the situation where CR was contraindicated, palliative procedures were performed in case it was necessary. Involvement of the SMV or PV, if tumor thrombi were not present inside these vessels and involvement of the tumor in less than 180 degrees of the vessel wall, were not considered as contraindications for CR. Malignant causes were present in 175 patients and 119 patients underwent CR for pancreatic adenocarcinoma (patients with neuroendocrine tumors, those who only had open biopsies and palliative surgeries or surgeries which did not include the curative resection (n=56) were not included in the study).
One hundred and two (102) patients who did not require venous resection / repair at the time of surgery (Group-I) were compared with 17 patients in which the tumor had infiltrated the SMV / PV and vascular resection / repair (Group-II) was performed during the CR. These patients (N=17) underwent partial (N=4) or complete resection (N=13) of the involved segment of the vein as well as primary repair / anastomosis (N=12), repair using autologous veins (N=4) or repair using a synthetic patch (N=1).
Demographic data, duration of operation, use of hemodilution technique, estimated blood loss (EBL), amount of blood transfusion (intra-operative and postoperative), length of hospital stay (LOS), rate and severity of complications (pancreatic leak, biliary leak, bleeding, gastroparesis, infection, etc), peri-operative mortality, and long-term outcome were studied. In this study, perioperative complication was defined as presence of intraor postoperative complications up to 30 days after surgery or at the time of patient’s discharge, whichever was longer. The severity of peri-operative complications were scored based on the revised Clavien-Dindo (CD) classification [40, 41]. When more than one complication occurred, the score of the most sever complication was considered as the complication score of the patient. Final pathology reports were re-reviewed by another pathologist blinded to patient information for evaluation of the number, size and location of lesions in the pancreas, type of tumor (cystic or solid), lymph node involvement, number of resected and involved lymph nodes, resection margin status, tumor grade, and tumor stage. Tumor staging was based on the American Joint Committee on Cancer (AJCC) 7th edition TNM staging system (AJCC Cancer Staging Manual. 7th ed. New York, NY: Springer, 2010) and tumor grades were coded as 1 (well differentiated), 2 (moderately differentiated), 3 (poorly differentiated), or 4 (undifferentiated).
If CA 19-9 was high before the procedure and decreased after surgery, levels were checked regularly for early detection of recurrence during follow up. In addition, regular imaging, including computed tomography (CT) and/or positron emission tomography (PET), was also used (every six months for two years and yearly up to five years thereafter) for detection of recurrence during the follow-ups. Patients were followed indefinitely.
STATISTICS
Descriptive statistics were used to summarize the data. Student’s t-test, chi-square test, Kaplan Meier method and log-rank test were used for statistical analysis. In a multivariate analysis using a Cox regression model, variables were assessed in search of independent risk factors predicting poor outcome in the patients. A p-value of less than 0.05 will be considered significant.
RESULTS
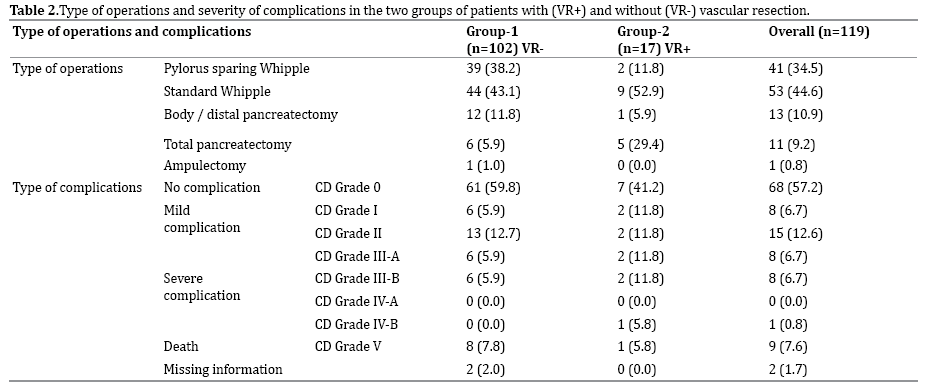
The mean age of the patients was 64.1 + 10.2 years. Sixty (50.4%) of patients were male and 89 (74.8%) were Caucasian. Age, gender and race were not significantly different between Group-I and Group-II patients (P > 0.05 for all). Ninety-six percent of lesions (N=114) were solid, and there were five cases where the tumor had cystic appearance. Patient and tumor characteristics of the two groups are depicted in Table 1. Types of operations performed in the 119 patients are summarized in Table 2.
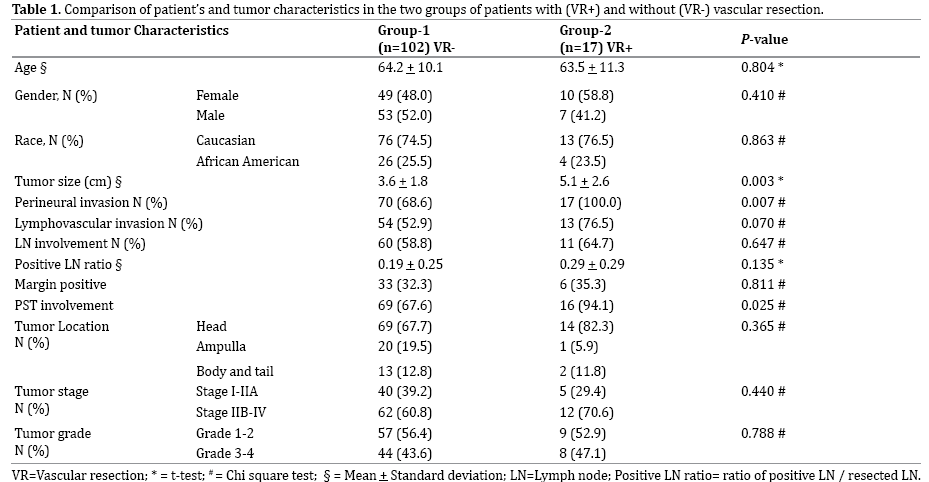
The tumor grades were: 1 (N=5, 4.3%), 2 (N=61, 51.7%), 3 (N=49, 41.5%), and 4 (N=3, 2.5%). The stages were: 1A (N=5, 4.2%), 1B (N=9, 7.6%), IIA (N=31, 26.0%), IIB (N=57, 47.9%), III (N=13, 10.9%), and IV (N=4, 3.4%). Mean tumor size was 3.8 + 1.9 cm. More than 59% (N=71) of the patients had lymph node involvement at the time of surgery, and 71.4% (N=85) had peripancreatic soft tissue (PST) involvement. A postoperative tumor free resection margin (R-0 resection) was achieved in 67.2% (N=80) of the patients. Perineural invasion and lympho-vascular invasion was seen in 73.1% (N=87) and 56.3% (N=67) of the tumors, respectively.
Mean OR time was 320 + 76 minutes for the patients in group-I and 400 + 82 minutes for the patients in Group-II (P=0.051). Sixty seven patients in group-I (67%) and 15 patients in group-II (88.2%) received a blood transfusion during their hospital stay (intra- and postoperative) (P=0.077), and the average amount of the inpatient blood transfusion for the patients (N=119) was 3.7 + 7.1 units (Range 0-57). Table 3 compares operative and inpatient data between the patients in Group-I and Group-II.
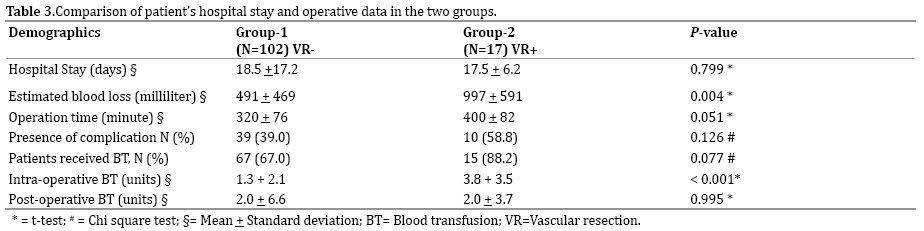
The intra-operative blood transfusion requirement was significantly higher in Group-II (3.8 + 3.5) compared with Group-I (1.3 + 2.1) patients (P < 0.001). Twelve patients in Group-I (11.8%) and six patients in Group-II (35.3%) received four or more units of blood intra-operatively (P=0.023). Postoperative blood transfusion requirements were not significantly different between the two groups (P= 0.995). In 30 patients (25.2%), one to two bottles of blood was taken pre-operatively from the patient and was transfused back after the operation (Hemodilution technique). These patients (N=30) required significantly less blood transfusion during their hospital stay (1.4 + 2.1) compared with the other patients (4.5 + 8.0) (P=0.001).
Pre-operation CA 19-9 serum levels > 200 U/mL were significantly associated with higher risk of vascular involvement (PV and SMV) in the patients (P=0.032). Final pathology reports showed tumor involvement of at least one of the resected margins (R-1) in 32.3% of the cases in Group-I and 35.3% in Group-II, and the rate was not significantly different between the two groups (P=0.811).
Peri-operative complications were seen in 39 % and 58.8% of the patients in Group-I and Group-II respectively (P=0.126). Severity of complications was not different between the two groups. While the majority of reported complications were minor, the frequency of severe complications (CD grade > IIIb) was not significantly different between the groups (p=0.295). No intra-operative death was encountered, and there were a total of nine peri-operative mortalities [8 cases in Group-I (7.8%) and 1 cases in Group-II (5.9%), P=0.777]. Table 2 summarizes the peri-operative complications in the patients based on their CD severity score.
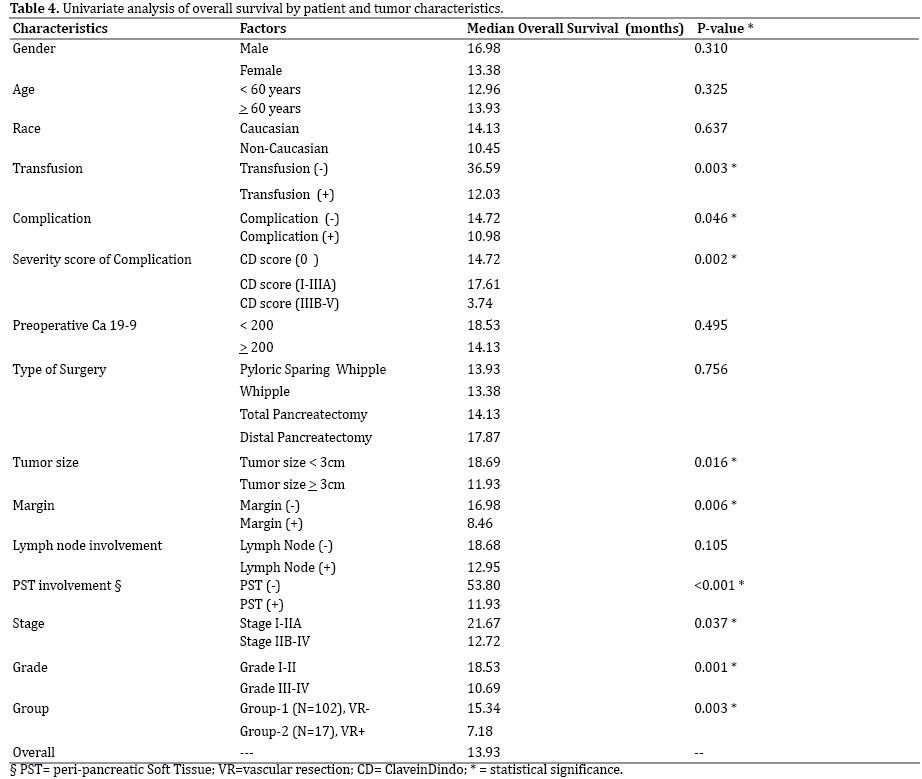
LOS in Group-I and Group-II patients was 18.5 + 17.2 and 17.5 + 6.2 days, respectively (P=0.799). While age, gender, race, pre-operative CA-19-9 level, type of surgery, and lymph node involvement were not predictors of survival in our patients, requirement for transfusion (P=0.003), presence of complication (P=0.046), severity of complications (P=0.002), larger tumor size (P=0.016), resection margin tumor involvement (R1) (P=0.006), presence of tumor in the peripancreatic soft tissue (PST involvement) (P<0.001), higher tumor stage (P=0.037), and higher tumor grade (P=0.001) were all predictors of a poor outcome in the patients. Patients in Group-II had a significantly lower median overall survival compared with Group-I patients (P=003). Figure 1 shows the overall survival of the patients in the groups of patients with and without vascular resection (Group-II and Group-I patients, respectively). A univariate analysis of different patient and tumor characteristics and their value in predicting survival is listed in Table 4.
Figure 1. This graph compares the overall survival of the patients in the groups with and without vascular resection (Group-II and Group-I patients
respectively).
The 5-year overall survival (5-year-OS) for N-0 and N (+) was 25.4% and 18.3% (p=0.05), respectively, and the 5-year-OS for R-0 and R1 was 25.7% and 10.1% (p=0.006) respectively. Tumor stages IIB-IV had significantly lower median overall survival than stages I-IIA (p=0.037). Figures 2A and 2B compare the overall survival of the patients based on the surgical resection margin status in Group-1 and Group-II patients respectively. Figures 2C and 2D compare the outcomes of patients with a negative resection margin (2C) or a positive (R1) resection margin (2D) between the two groups of patients who required vascular resection and those who did not require a vascular resection.
Figure 2. A: Compares the overall survival of the patients who did not require a venous resection / reconstruction based on the margin status in the final
pathology report. B: Compares the overall survival of the patients who required a venous resection /reconstruction based on the margin status in the final
pathology report. C: Compares the overall survival of the patients who had a negative margin in their final pathology report based on the requirement of
venous resection / reconstruction. D: Compares the overall survival of the patients who had a positive margin in their final pathology report based on the
requirement of venous resection / reconstruction.
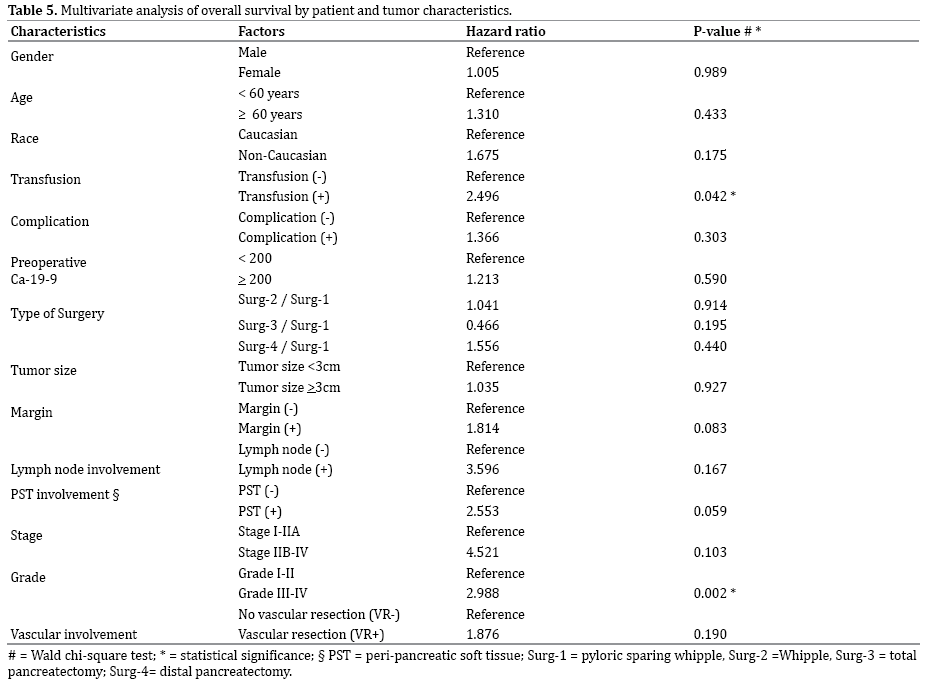
Multivariate analysis using a Cox regression model demonstrated that requirement of transfusion and tumor grade were the only independent predictors of outcome in the patients (P < 0.05 for both). Table 5 shows the multivariate analysis of the overall survival in the patients based on patient and tumor characteristics. The overall mean follow-up time (N=119) has been 18.1 months and 40 (33.6%) patients are currently alive. The mean followup time for Group-I and Group-II patients have been 19.6 months and 8.9 months, respectively. Three patients in Group-II (17.7%) and 37 patients in Group-I (36.3%) are currently alive (P=0.171).
DISCUSSION
Better patient selection and earlier diagnosis due to more accurate diagnostic modalities such as PET CT, EUS, and newer generations of CT or MRI/MRCP have been instrumental in increasing the curative resectability rate in patients suffering from a pancreatic malignancy [4, 5]. At the same time, more centralization of these patients in high volume centers with adequate expertise in this type of surgery, together with better intra- and perioperative care, has helped to decrease perioperative mortality significantly [6, 42]. All these factors have played a major role in improving long term patient survival worldwide. In spite of these advances, a majority of patients with pancreatic cancer are still diagnosed late. As high as 50% of these patients have metastasis at the time of diagnosis, and curative surgery will not be an option. It has been claimed that only those patients who have locally advanced disease, even in the form of large venous (SMV/PV) involvement (borderline resectable tumors), may benefit from a more aggressive surgery. Numerous reports have shown similar short and long term results when venous resection was performed in conjunction with conventional pancreato duodenectomy [2, 11-28, 43, 44]. Indirect evidence suggests that patients with extensive venous involvement (larger than 3 cm in length, complete circumferential involvement, tumor thrombi in the vessel or total occlusion of the vessel) may not get the benefit from en-bloc resection of the SMV/PV with the tumor [2, 3]. This may be due to the aggressive biology of the tumor versus location of the tumor, and, possibly, due to the hematogenous spread of the tumors.
This retrospective study, like others, has shown that the most important factor in achieving long term survival in patients with resectable pancreatic cancer is obtaining an R-0 resection [45]. At the same time, we have tried to increase the resectability rate in patients who had borderline resectable tumors. In terms of feasibility and safety, we have shown that morbidity and complication rates were not significantly different in patients who required resection and / or repair of their vascular involvement compared to patients who underwent conventional pancreatoduodenectomy or other CR. This is similar to the observation reported by Aktekin et al. [43]. However, Worni [46] and Castleberry [47] groups reported higher intraoperative and post operative complication rates in the patients undergoing vascular resection. On the other hand, the long term follow-up and survival analysis in our patients showed that venous resection and reconstruction in the patients with borderline resectable pancreatic tumors did not offer a comparable outcome to those who did not require venous resection even when R-0 resection was achieved. This is similar to the reported outcome by Ouassi and the multidisciplinary HPB Group of Center of Cancer [48].
A comparison between the tumor characteristics in the two groups of patients with and without venous involvement showed that patients with major venous involvement had significantly larger tumor size with more aggressive tumor characteristics (higher rate of perineural invasion and peripancreatic soft tissue involvement). This might explain the lower long term overall survival in these patients. This finding is also supported by the fact that vascular resection as a factor was not an independent predictor of outcome in our cohort when we performed a multivariate Cox regression analysis.
The percentage of major vascular resections in our study seems to be lower than in other studies (14.3 % vs. 25- 70%) [2, 41, 43]. In our series, all of the cases with vascular resection (Group-II) had pathological evidence of vessel (venous) involvement compared to other published studies in which up to only 40-70% of the resected vessels showed tumor involvement [21, 22, 43]. This may explain a better overall survival in the patients reported in the literature compared to our patients. In some of the reported studies, all patients who had venous resection did not have advanced disease as verified by up to 30-60% lack of vessel involvement confirmed by final pathology reports [22, 44]. This is in contradistinction to our patients who required venous resection, 100% of which showed venous involvement by the tumor. One may argue that we may have missed some cases with vascular involvement. Even though this is a possibility, we have been as aggressive as high volume centers in resecting the involved vessels. The other explanation could be that centers with high resection rates may have a large percentage of patients referred to them due to their special interest in treating only the locally advanced tumors.
Jane et al., reported on 48 patients in whom some type of vascular resection was performed during Whipple procedure, but failed to mention the center’s overall activity, so it is not known what percentage of their patients required major vascular resection [45]. Additionally, histopathological proof of venous invasion was not ascertained in their study, so the true incidence of vascular involvement in these 48 patients is not known.
We have not found it necessary either to bypass the SMV to PV beyond the resection line or to perform the resection and repair of these vessels under SMA occlusion, as practiced by Nakao et al. [25]. This originates from our extensive experience with liver and pancreas transplantation where we occlude the portal vein or SMV for up to 30 minutes without any complications.
In our study, transfusion requirement, presence of complication, severity of complications, tumor size, margin status, PST status, tumor stage, and tumor grade played a significant role in predicting the patient outcomes. This was in line with previous studies [6, 8, 13, 16, 20, 21, 24, 31]. In our experience the only independent predictors of lower survival were requirement of transfusion and tumor grade, which represent both the aggressiveness of a tumor and the subsequent requirement for a very extensive resection.
LIMITATIONS OF THE STUDY
This is a retrospective study from a medium size hepatopancreato- billiary and transplant center and our findings need to be verified by larger series and ideally prospective design studies. We also acknowledge that in the current study, there are relatively small number of study subjects (n=119) for the 14 predictors included in the final model. This limitation could be overcome by collaborating with other medical centers to acquire more study subjects in the future or limiting the study to include smaller number of predictors. We believe the currently included risk factors were important predictors of the survival of the patients and had to be included in the analysis.
CONCLUSION
In conclusion, better patient selection, intra- and perioperative care, center volume and surgeon experience have all contributed to recent improvements in the outcomes of major pancreatic surgeries. In patients with a locally advanced or borderline resectable pancreatic malignancy with major venous involvement, en block venous resection during Whipple operation or total or distal pancreatectomies is technically feasible without an immediate increase in morbidity, but overall survival was not affected but this approach. In our experience the most important and independent predictors of long term outcome were tumor grade and requirement for blood transfusion in the patients.
Acknowledgement
The authors would like to thank Mr. John Cyrus who provided us editorial assistance. This research is supported by the Donnie and Gail Juneau Endowed Chair in Transplantation.
Conflicts of Interest
Authors declare that they have no conflict of interest to disclose.
References
- Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2008. CA Cancer JClin. 2008; 58: 71-96. [PMID:18287387]
- Ramacciato G, Mercantini P, Petrucciani N, et al. Does portal-superiormesenteric vein invasion still indicateirresectability for pancreaticcarcinoma? Ann Surg Oncol. 2009; 16:817-825. [PMID:19156463]
- Illuminati G, Carboni F, Lorusso R, et al. Results of a pancreatectomywith a limited venous resection for pancreatic cancer. Surg Today. 2008;38:517-523. [PMID:18516531]
- Neoptolemos JP, Russell RC, Bramhall S, et al. Low mortality following resection for pancreatic and periampullarytumours in 1026 patients: UKsurvey of specialist pancreatic units. UK Pancreatic Cancer Group. Br JSurg. 1997; 84:1370-1376. [PMID:9361591]
- Wagner M, Redaelli C, Lietz M, et al. Curative resection is the single most important factor determining outcome in patients with pancreaticadenocarcinoma. Br J Surg. 2004; 91:586-594. [PMID:15122610]
- Winter JM, Cameron JL, Campbell KA, et al. 1423 pancreaticoduodenectomies for pancreatic cancer: A single-institution experience. J Gastrointest Surg. 2006; 10:1199-210. [PMID:17114007]
- Cameron JL, Riall TS, Coleman J, et al. One thousand consecutive pancreaticoduodenectomies. Ann Surg. 2006; 244:10-5. [PMID:16794383]
- Sommerville CA, Limongelli P, Pai M, et al. Survival analysis after pancreatic resection for ampullary and pancreatic head carcinoma: an analysis of clinicopathological factors. J Surg Oncol. 2009; 100:651-6.[PMID:19722229]
- Fortner JG. Regional resection of cancer of the pancreas: a new surgical approach. Surgery. 1973; 73:307-320. [PMID:4265314]
- Varadhachary GR, Tamm EP, Abbruzzese JL, et al. Border line resectablepancreatic cancer: definitions, management, and role of preoperativetherapy. Ann Surg Oncol. 2006; 13:1035-46. [PMID:16865597]
- Moore GE, Sako Y, Thomas B. Radical pancreatoduodenectomy with resection and reanastomosis of the superior mesenteric vein. Surgery.1951; 30:550-3.Asada D, Itaya H, Nakamura K, et al. Radical pancreatoduodenectomyand portal vein resection. Report of two successful cases with transplantation of portal vein. Arch Surg. 1963; 87:609-13.
- Asada D, Itaya H, Nakamura K, et al. Radical pancreatoduodenectomy and portal vein resection. Report of two successful cases with transplantation of portal vein. Arch Surg. 1963; 87:609-13.
- Howard TJ, Villamustre N, Moore SA, et al. Efficacy of venous reconstruction in patients with adenocarcinoma of the pancreatic head. J Gastrointest Surg. 2003; 7:1089-95. [PMID:14675720]
- Poon RT, Fan ST, Lo CM, et al. Pancreaticoduodenectomy with en bloc portal vein resection for pancreatic carcinoma with suspected portal vein involvement. World J Surg. 2004; 28:602-8. [PMID:15366753]
- Leach SD, Lee JE, Charnsangavej C, et al. Survival following pancreaticoduodenectomy with resection of the superior mesentericportalconfluence for adenocarcinoma of the pancreatic head. Br J Surg.1998; 85:611-7. [PMID:9635805]
- Tseng JF, Raut CP, Lee JE, et al. Pancreaticoduodenectomy with vascular resection: margin status and survival duration. J Gastrointest Surg. 2004; 8:935-49. [PMID:15585381]
- Tseng JF, Tamm EP, Lee JE, et al. Venous resection in pancreatic cancer surgery. Best Pract Res Clin Gastroenterol. 2006; 20:349-64. [PMID:16549332]
- Shibata C, Kobari M, Tsuchiya T, et al. Pancreatectomy combined with superior mesenteric-portal vein resection for adenocarcinoma in pancreas. World J Surg. 2001; 25:1002-5. [PMID:11571964]
- Martin RCG 2nd, Scoggins CR, Egnatashvili V, et al. Arterial and venous resection for pancreatic adenocarcinoma: operative and long-term outcomes. Arch Surg. 2009;144:154-9. [PMID:19221327]
- Toomey P, Hernandez J, Morton C, et al. Resection of Portovenousstructures to obtain microscopically negative margins during Pancreaticoduodenectomy for pancreatic adenocarcinoma is worthwhile.Am Surg. 2009; 75:804-9. [PMID:19774952]
- Bachellier P, Nakano H, Oussoultzoglou PD, et al. Is Pancreaticoduodenectomy with mesentericoportal venous resection safe and worthwhile? Am J Surg. 200l; 182:120-9. [PMID:11574081]
- Carrere N, Sauvanet A, Goera D, et al. Pancreaticoduodenectomy with mesentericoportal vein resection for adenocarcinoma of the pancreatic head. World J Surg. 2006; 30:1526-35. [PMID:16855797]
- Al-Haddad M, Martin JK, Nguyen J, et al. Vascular resection and reconstruction for pancreatic malignancy: a single center survival study. J Gastrointest Surg. 2007; 11:1168-74. [PMID:17632763]
- Yekebas EF, Bogoevski D, Cataldegirmen G, et al. En bloc Vascular resection for locally advanced pancreatic malignancy infiltrating major blood vessels: perioperative outcome and long-term survival in 136 patients. Ann Surg. 2008; 247:300-9. [PMID:18216537]
- Nakao A, Takeda S, Inoue S, et al. Indications and techniques of extended resection for pancreatic cancer. World J Surg. 2006; 30:976-82.[PMID:16736324]
- Müller SA, Hartel M, Mehrabi A, et al. Vascular resection in pancreatic cancer surgery: survival determinants. J Gastrointest Surg. 2009; 13:784- [PMID:19137380]
- Harrison LE, Klimstra DS, Brennan MF. Isolated portal vein involvement in pancreatic adenocarcinoma. A contraindication for resection? Ann Surg. 1996; 224: 342–349. [PMID:8813262]
- Misuta K, Shimada H, Miura Y, et al. The role of splenomesenteric vein anastomosis after division of the splenic vein in pancreatoduodenectomy. J Gastrointest Surg. 2005; 9:245-53. [PMID:15694821]
- Allema JH, Reinders ME, Van Gulik TM, et al. Portal vein resection in patients undergoing pancreatoduodenectomy for carcinoma of the pancreatic head. Br J Surg. 1994; 81:1642-6. [PMID:7827892]
- Roder JD, Stein HJ, Siewert JR. Carcinoma of the periampullary region: Who benefits from portal vein resection? Am J Surg. 1996; 171:170-4.[PMID:8554135]
- Kremer B, Vogel I, Lüttes J, et al. Surgical possibilities for pancreatic cancer: extended resection. AnnOncol. 1999; 10 Suppl 4:252-6.[PMID:10436834]
- Launois B, Stasik C, Bardaxoglou E, et al. Who benefits from portal vein resection during pancreaticoduodenectomy for pancreatic cancer? World J Surg. 1999; 23:926-9. [PMID:10449822]
- Van Geenen RC, Ten Kate FJ, De Wit LT, et al. Segmental resection and wedge excision of the portal or superior mesenteric vein during pancreatoduodenectomy. Surgery. 2001; 129:158-63. [PMID:11174708]
- Siriwardana HP, Siriwardena AK. Systematic review of outcome of synchronous portal-superior mesenteric vein resection during pancreatectomy for cancer. Br J Surg. 2006; 93:662-73. [PMID:16703621]
- Kaneoka Y, Yamaguchi A, Isogai M. Portal or superior mesenteric vein resection for pancreatic head adenocarcinoma: Prognostic value of thelength of venous resection. Surgery. 2009; 145:417-25. [PMID:19303991]
- Riediger H, Makowiec F, Fischer E, et al. Postoperative morbidity and long-term survival after pancreaticoduodenectomy with superior mesenterico-portal vein resection. J Gastrointest Surg. 2006; 10:1106-15. [PMID:16966029]
- Stitzenberg KB, Watson JC, Roberts A, et al. Survival afterpancreatectomy with major arterial resection and reconstruction. Ann Surg Oncol. 2008; 15:1399-406. [PMID:18320285]
- Weitz J, Koch M, Friess H, et al. Impact of volume and specialization for cancer surgery. Dig Surg. 2004; 21:253-61.
- Koniaris LG, Staveley-OCarroll KF, Zeh HJ, et al. Pancreaticoduodenectomy in the presence of superior mesenteric venous obstruction. J Gastrointest Surg. 2005; 9:915-21. [PMID:16137584]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications: a new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg. 2004; 240:205-13. [PMID:15273542]
- Clavien PA, Barkun J, de Oliveira ML, et al. The Clavien-Dindoclassification of surgical complications: five-year experience. Ann Surg. 2009; 250:187-96. [PMID:19638912]
- Tucker ON, Rela M. Controversies in the management of borderline resectable proximal pancreatic adenocarcinoma with vascular involvement. HPB Surg. 2008.
- Aktekin A, Küçük M, Odabasi M, et al. The importance of invasion and resection of superior mesenteric and portal veins in adenocarcinoma of the
- Kelly KJ, Winslow E, Kooby D, et al. Vein involvement during pancreaticoduodenectomy: is there a need for redefinition of "borderline resectable disease"? J Gastrointest Surg. 2013; 17:1209-17. [PMID:23620151]
- Jain S, Sacchi M, Vrachnos P, et al. Carcinoma of the pancreas with portal vein involvement--our experience with a modified technique of resection. Hepatogastroenterology. 2005; 52:1596-600. [PMID:16201124]
- Worni M, Castleberry AW, Clary BM, et al. Concomitant vascular reconstruction during pancreatectomy for malignant disease: a propensity score-adjusted, population-based trend analysis involving10,206 patients. JAMA Surg. 2013;148:331-8. [PMID:23715922]
- Castleberry AW, White RR, De La FuenteSG, et al. The impact of vascular resection on early postoperative outcomes after pancreaticoduodenectomy: an analysis of the American College of Surgeons National Surgical Quality Improvement Program database. Ann Surg Oncol. 2012; 19:4068-77. [PMID:22932857]
- Ouaissi M, Hubert C, Verhelst R, et al. Vascular reconstruction during pancreatoduodenectomy for ductal adenocarcinoma of the pancreas improves resectability but does not achieve cure. World J Surg. 2010;34:2648-61. [PMID:20607257]



