Keywords
Cell Differentiation; Pancreatic Neoplasms; Ultrasonography
INTRODUCTION
The most common pancreatic tumors are adenocarcinomas and pancreatitis-associated masses. Neuroendocrine lesions, cystic tumors and metastases to the pancreas occur less frequently. The differentiation of pancreatic tumors is important for therapeutic planning and for the evaluation of the prognosis but this difficult with current imaging techniques, even when a combination of various diagnostic procedures is employed. Although histology or cytology obtained from fine needle biopsy or surgery is the standard of reference, especially in the differential diagnosis between pancreatitis-associated lesions and adenocarcinomas, needle biopsy can produce false results due to sampling error. Endoscopic retrograde (ERCP) and magnetic cholangiopancreatography (MRCP) are the current imaging standards for the differential diagnosis of pancreatic lesions [1, 2, 3, 4, 5]. With conventional transabdominal ultrasound, there are no characteristic findings for the differentiation of pancreatic masses and its diagnostic accuracy is less than 70% [6, 7, 8, 9]. Echo-enhanced ultrasound has been proposed as a valuable technique for the differentiation of liver lesions [10, 11, 12, 13, 14, 15]. We and others have demonstrated that echo-enhanced ultrasound is a valuable imaging method to evaluate pancreatic tumors [16, 17, 18, 19, 20]. In this review, we present a practical approach for the use of echo-enhanced sonography in the differential diagnosis of pancreatic masses.
Technical Aspects of Echo-Enhanced Ultrasound
All patients are first investigated by conventional sonography using a dynamic sector scanner. Special patient preparation is not necessary. When using echo-enhanced sonography, the pulse inversion technique or the power-Doppler mode under the conditions of 2nd harmonic imaging are available. At present, the pulse inversion mode is used more frequently than 2nd harmonic imaging.
When performing echo-enhanced sonography with pulse inversion, 2.4 mL SonoVue® (Bracco Spa, Milan, Italy) are injected intravenously, and the mechanical index varies from 0.1 to 0.2 (low mechanical index procedure). The investigation can be done in real time and lasts approximately two minutes.
Echo-enhanced power Doppler sonography starts immediately after the injection of 4 g Levovist® (Schering AG, Berlin, Germany) at a 300 mg/mL concentration. Intermittent sweeps have to be carried out and the investigation lasts also approximately two minutes. One focus zone with depth adapted to the area of interest and a mechanical index of 0.8 to 1.3 (high mechanical index procedure) should be used.
Criteria for Pancreatic Tumor Differentiation
Criteria for the differentiation of pancreatic masses by conventional and echo-enhanced sonography have recently been published (Table 1) [9, 16].
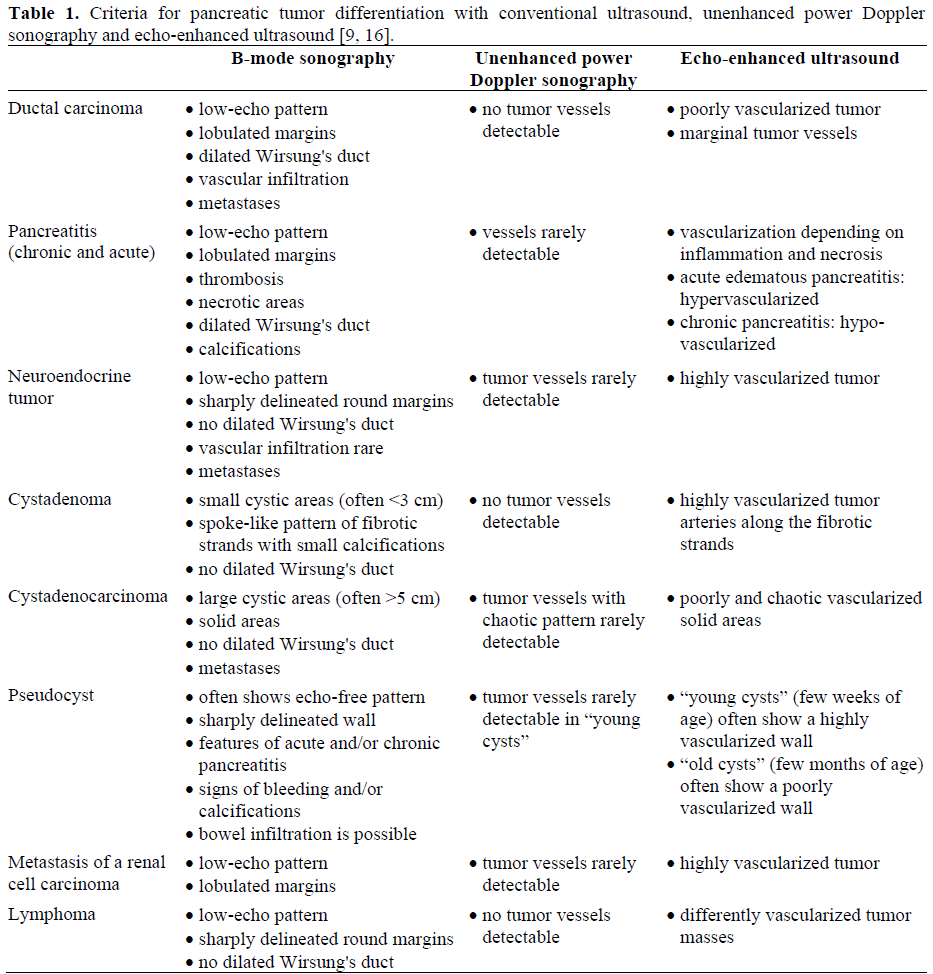
• An adenocarcinoma presents at B-mode ultrasound with a low-echo pattern and lobulated margins. The Wirsung's duct is dilated (Figure 1a). At echo-enhanced sonography, the lesion is, in most cases, poorly vascularized (Figure 1b).
Figure 1. Pancreatic adenocarcinoma at conventional(a.) and echo-enhanced sonography (b.). a. Low-echo tumor with lobulated margins and dilatation ofWirsung's duct. b. Poorly vascularized lesioncompared to the surrounding tissue.
• In contrast to adenocarcinomas, neuroendocrine tumors and metastases of renal cell carcinomas show sharply delineated margins, and the Wirsung's duct is usually not dilated (Figure 2a). Hypervascularization after the injection of an echo-enhancer is a characteristic sign of these masses (Figure 2b).
Figure 2. Pancreatic metastatis of a renal cell carcinoma at conventional (a.) and echo-enhanced sonography (b.) a. Low-echo with sharpy delineated margins without dilataion of Wirsung's duct. b. Highly viscularized lesion compared to the sorrounding tissue.
• In particular, the differential diagnosis of adenocarcinomas and pancreatitis-associated masses is notoriously problematic since both tumors can appear as low-echo and lobulated lesions with dilatation of Wirsung's duct. The vascularization of pancreatitis-associated tumors depends on the degree of inflammation and necrosis. Acute edematous lesions are generally hypervascularized (Figure 3). On the other hand, necroses or chronic pancreatitis-associated masses are mostly hypovascularized.
Figure 3. Pancreatitis-associated lesion at conventional(a.) and echo-enhanced sonography (b.). a. Lobulatedmass (arrows) with a small pseudocyst. b. Highly vascularized lesion compared to the surrounding tissue.
• Cystic pancreatic neoplasms are rare. While serous microcystic adenomas are characterized by small cystic areas and highly vascularized fibrotic strands (Figure 4), cystadenocarcinomas consist of large cysts and poorly vascularized solid areas. Pseudocysts show an echo-free pattern and a sharply delineated wall. In cases of chronic pancreatitis, the remaining pancreatic parenchyma may display features of chronic inflammation such as calcifications and a dilated Wirsung's duct. After the injection of an echo-enhancer, the wall of the pseudocysts is highly (“young cyst”) or poorly (“old cyst”) vascularized.
Figure 4. Serous cystadenoma at conventional (a.) and echo-enhanced sonography (b.). a. Tumor at the pancreatic tail with small cystic areas (small arrows) and thin fibrotic strands. b. Highly vascularized tumor arteries (large arrows) along the fibrotic strands.
Results of Echo-Enhanced Ultrasound in the Differentiation of Pancreatic Tumors
Several studies have demonstrated that echo-enhanced sonography is a valuable method for the evaluation of pancreatic lesions (Table 2) [16, 17, 18, 19, 20]. Similar to conventional ultrasound, operator depend-ency, flatulence, obesity, deep lesions, and tumors in the pancreatic tail are limitations of this procedure.
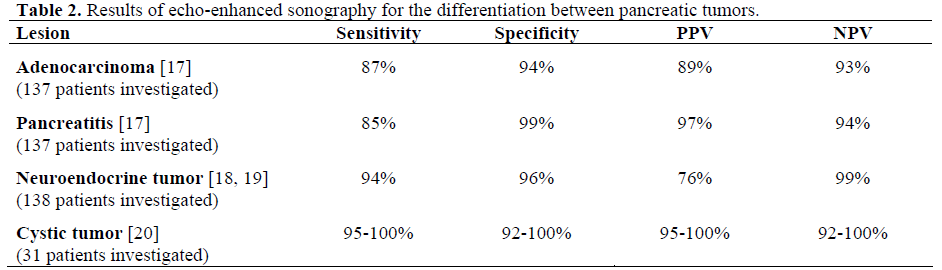
In a study published in 2002 [17], only 57% of the adenocarcinomas were correctly classified by conventional and unenhanced ultrasound. However, with echo-enhanced sonography, 87% of the masses could be differentiated (P=0.0001). Two out of 47 carcinomas were interpreted erroneously as pancreatitis-associated masses. Of the pancreatitis-associated tumors, 85% were diagnosed correctly by echo-enhanced sonography. Four out of 41 benign tumors were falsely classified as ductal carcinomas. All of them showed necrotic tissue at histology.
Another study showed good results of echo-enhanced ultrasound in the differentiation of neuroendocrine pancreatic tumors [18]. Table 2 demonstrates that, with this procedure, a sensitivity of 94% and a specificity of 96% was achieved. Other reports have confirmed these good results [19]. On the other hand, it was shown that the overall sensitivity of somatostatin receptor scintigraphy in the differential diagnosis of neuroendocrine pancreatic tumors is less than 55% [18].
Furthermore, a recently published study showed that echo-enhanced sonography can differentiate cystic neoplasms from pseudocysts [20]. However, one out of 10 cystadenomas was misdiagnosed as a cystadenocarcinoma and vice-versa. The morphological variability of these cystic lesions at conventional ultrasound and the difficulties in the evaluation of the vascularization of cystic masses seem to be responsible for the false results.
Discussion
There is no ideal diagnostic procedure to differentiate between pancreatic tumors. The gold standard is histology, obtained either through image-guided fine needle biopsy or surgery. However, especially when evaluating pancreatitis-associated lesions and adeno-carcinomas, needle biopsy can produce false negative results due to sampling error. ERCP is the standard for diagnostic imaging, but has an increased risk of complications, the most important being pancreatitis [21, 22]. MRCP (including magnetic resonance tomography) has a sensitivity (about 80%) and specificity (about 90%) similar to ERCP for detecting pancreatic cancer or chronic pancreatitis [1, 2, 3, 4, 5]. However, this procedure is expensive and available only in large medical centers. In some studies evaluating pancreatic tumor differentiation with computed tomography, endoscopic ultrasonography and positron emission tomography, sensitivities and specificities of more than 90% were observed [23, 24, 25, 26]. However, in these studies, only a small number of patients were investigated. In most cases, computed tomography and endoscopic ultrasonography are unable to differentiate between pancreatic tumors satisfactorily but may be the best methods to stage for resectability and to detect metastases [27, 28, 29].
There are no characteristic signs to differentiate between the various pancreatic lesions when using conventional trans-abdominal ultrasound. In particular, the differentiation of adenocarcinoma from chronic pancreatitis is notoriously problematic [9, 16].
Some years ago, the angiographic vascular-ization pattern was reported to be helpful to differentiate between pancreatic tumors [30, 31, 32]. Whereas ductal carcinomas are characterized by their hypovascularization, neuroendocrine tumors were found to be hypervascularized. However, the diagnostic accuracy of angiography is low because it is impossible to investigate the macroscopic tumor features.
Unenhanced power Doppler sonography also allows the investigation of the vascularization pattern of tumors by ultrasound. For instance, there are good results for diagnosing the degree of differentiation of hepatocellular carcinomas using this method [13, 33]. However, in the differential diagnosis of pancreatic masses, no diagnostic advantage of this method was observed in comparison to conventional ultrasound. This might be explained by the low sensitivity of unenhanced power Doppler sonography for detecting low blood flow velocity or small vessels and the existence of multiple tissue artifacts [9, 10].
The sensitivity of power Doppler sonography can be increased by echo-enhancers, such as Levovist®. This preparation consists of microbubbles of air which enhance the Doppler signal at 20-30 dB [10, 34, 35]. With echo-enhanced power Doppler sonography, however, the signal intensity from flowing blood is much lower as compared to that of moving solid structures, such as tissue movements. Thus, 2nd harmonic imaging was developed to overcome these difficulties. This method is based on the property of microbubbles to resonate and emit harmonic waves in an ultrasound field with a frequency of 1-5 MHz. If the harmonic frequency is to be detected at twice the transmitted frequency, the procedure is called 2nd harmonic imaging. Tissue particles have fewer 2nd harmonic waves than microbubbles; therefore, the signals of echo-enhancers become more distinguishable [10].
Recently, the new contrast agent SonoVue® has been used more frequently for echo-enhanced sonography. Furthermore, 2nd harmonic imaging has partially been replaced by the pulse inversion imaging technique. With this new procedure, more favorable results can be achieved than with 2nd harmonic imaging. With 2nd harmonic imaging, it is impossible to separate the transmitted and the received harmonic signal completely due to limited bandwidth. However, pulse inversion imaging avoids these bandwidth limitations by using characteristics specific to the microbubble vibrations to subtract rather than filtering out the fundamental vibrations. Because this imaging transmits two reciprocal pulses, leading to the subtraction of fundamental signals, it allows the use of broader transmission and receiving bandwidths for improved resolution and can provide increased sensitivity to contrast [36]. However, the comparative results of large prospective studies are lacking.
Characteristic signs of pancreatic tumors at echo-enhanced sonography have been published [9, 16]. Similar to their angiographic features, ductal carcinomas and the solid areas of cystadenocarcinomas were found to be hypovascularized. In contrast, neuroendocrine tumors and the solid parts of cystadenomas are mostly hypervascularized. Pancreatitis-associated masses show different patterns of vascularization depending on inflammation, fibrotic scars, and the extent of necrosis [9, 16].
The results of the studies of Table 2 demonstrate that, with the combination of echo-enhanced sonography and 2nd harmonic or pulse inversion imaging, a higher percentage of ductal carcinomas, pancreatitis-associated masses, and neuroendocrine and cystic tumors can be classified correctly.
However, conventional ultrasound, unenhanced and echo-enhanced sonography must not be used as separate imaging techniques. Conventional ultrasound is the basic sonographic method and tumor differentiation is hardly possible with echo-enhanced ultrasound alone. Echo-enhanced sonography offers more diagnostic criteria than conventional ultrasound alone. Therefore, all sonographic procedures should be combined.
Echo-enhanced sonography has a similar accuracy in diagnosing pancreatic carcinoma as compared to ERCP and MRCP [1]. With respect to the differentiation of pancreatitis-associated tumors, the sensitivity of echo-enhanced power Doppler sonography seems to be slightly lower while the specificity is somewhat higher as compared to ERCP and MRCP [1]. Necroses and fibroses are major problems for the differential diagnosis of ductal carcinomas and pancreatitis-associated masses. Since both tissues are not vascularized, necrotic pancreatitis may be falsely interpreted as ductal carcinoma. On the other hand, it is possible to find inflammation in the surrounding tissue of an adenocarcinoma leading to the suspicion of pancreatitis.
Echo-enhanced sonography displayed, above all, a high sensitivity and specificity in differentiating between neuroendocrine tumors. Whereas endoscopic ultrasonography is of great value for localizing neuroendocrine pancreatic tumors [37], echo-enhanced sonography could become the new standard of reference for their differentiation by using imaging procedures.
However, there are reports of false results involving echo-enhanced sonography due to hypervascularized metastases of a renal cell carcinoma. Hypervascularization of metastases from renal cell carcinomas has also been observed in angiographic studies [38, 39]. This phenomenon is based on a well-vascularized stroma.
Cystic pancreatic masses are often associated with multiple artifacts at sonography. Although it is difficult to investigate the vascularization pattern of the solid tumor parts, the present results demonstrate the higher diagnostic value of echo-enhanced sonography as compared to conventional or unenhanced ultrasound [40]. However, MRCP seems to be more useful in the differential diagnosis of cystic pancreatic tumors [41, 42].
Furthermore, a recently published study showed that echo-enhanced sonography also produces excellent results in the staging of acute pancreatitis severity [43]. This procedure is cheaper and has fewer contraindications than computed tomography.
The successful treatment of pancreatic tumors requires a highly sensitive and specific diagnostic procedure. Echo-enhanced sonography is a powerful tool which may satisfy this requirement. New ultrasound procedures such as pulse inversion and vascular recognition imaging offer higher imaging quality. However, histology is the standard of reference for the definitive diagnosis of pancreatic lesions.
References
- Hartmann D, Schilling D, Bassler B, Adamek HE, Layer G, Riemann JF. ERCP and MRCP in the differentiation of pancreatic tumors. Dig Dis 2004; 22:18-25. [PMID 15292691
- Sugiyama M, Atomi Y, Hachiya J. Intraductal papillary tumors of the pancreas. Evaluation with magnetic resonance cholangiopancreatography. Am J Gastroenterol 1998; 93:156-9. [PMID 9468232
- Hintze RE, Adler A, Veltzke W, Abou-Rebyeh H, Hammerstingl R, Vogl T, Felix R. Clinical significance of magnetic resonance cholangiopancreatography (MRCP) compared to endoscopic retrograde cholangiopancreatography (ERCP). Endoscopy 1997; 29:182-7. [PMID 9201467
- Adamek HE, Weitz M, Breer H, Jakobs R, Schilling D, Riemann JF. Value of magnetic-resonance cholangio-pancreatography (MRCP) after unsuccessful endoscopic-retrograde cholangio-pancreatography (ERCP). Endoscopy 1997; 29:741-4. [PMID 9427493
- Soto JA, Barish MA, Yucel EK, Siegenberg D, Ferrucci JT, Chuttani R. Magnetic resonance cholangiography: comparison with endoscopic retrograde cholangiopancreatography. Gastroenterology 1996; 110:589-97. [PMID 8566608
- Palazzo L, Roseau G, Gayet B, Vilgrain V, Belghiti J, Fekete F, Paolaggi JA. Endoscopic ultrasonography in the diagnosis and staging of pancreatic adenocarcinoma. Results of a prospective study with comparison to ultrasonography and CT scan. Endoscopy 1993; 25:143-50. [PMID 8491130
- Karlson BM, Ekbom A, Lindgren PG, Kallskog V, Rastad J. Abdominal US for diagnosis of pancreatic tumor: prospective cohort analysis. Radiology 1999; 213:107-11. [PMID 10540649
- RöschTh, Lorenz R, BraigCh, Feuerbach S, Siewert JR, Classen M. Endoscopic ultrasound in the diagnosis of pancreatic tumors. Dtsch Med Wschr 1990; 115:1339-47. [PMID 2204522
- Rickes S, Unkrodt K, Ocran K, Neye H, Lochs H, Wermke W. Evaluation of Doppler ultrasonography criteria for the differential diagnosis of pancreatic tumors. Ultraschall Med 2000; 20:253-8. [PMID 11209722
- Wermke W, Gassmann B. Tumour Diagnostics of the Liver with Echo Enhancers. Berlin, Heidelberg, New York: Springer Verlag, 1998.
- Rickes S, Schulze S, Neye H, Ocran KW, Wermke W. Improved diagnosing of small hepatocellular carcinomas by echo-enhanced power Doppler sonography in patients with cirrhosis. Eur J GastroenterolHepatol 2003; 15:893-900. [PMID 12867800
- Rickes S, Ocran K, Schulze S, Wermke W. Evaluation of Doppler sonographic criteria for the differentiation of hepatocellular carcinomas and regenerative nodules in patients with liver cirrhosis. Ultraschall Med 2002; 23:83-90. [PMID 11961720
- Strobel D, Hoefer A, Martus P, Hahn EG, Becker D. Dynamic contrast-enhanced power Doppler sonography improves the differential diagnosis of liver lesions. Int J Colorectal Dis 2001; 16:247-56. [PMID 11515685
- Rickes S, Ocran KW, Gerstenhauer G, Wermke W. Evaluation of diagnostic criteria for liver metastases of adenocarcinomas and neuroendocrine tumors at conventional ultrasound, unenhanced power Doppler sonography and echo-enhanced ultrasound. Dig Dis 2004; 22:81-6. [PMID 15292699
- Bleck JS. Application of vascular recognition imaging (VRI) in the clinical routine. Visions 2003; 3:55-8.
- Rickes S, Flath B, Unkrodt K, Ocran K, Neye H, Lochs H, Wermke W. Pancreatic metastases of renal cell carcinomas - evaluation of the contrast behaviour at echo-enhanced power Doppler sonography in comparison to primary pancreatic tumors. Z Gastroenterol 2001; 39:571-8. [PMID 11558060
- Rickes S, Unkrodt K, Neye H, Ocran KW, Wermke W. Differentiation of pancreatic tumors by conventional ultrasound, unenhanced and echo-enhanced power Doppler sonography. Scand J Gastroenterol 2002; 37:1313-20. [PMID 12465731
- Rickes S, Unkrodt K, Ocran K, Neye H, Wermke W. Differentiation of neuroendocrine tumors from other pancreatic lesions by echo-enhanced power Doppler sonography and somatostatin receptor scintigraphy. Pancreas 2003; 26:76-81. [PMID 12499921
- Ding H, Kudo M, Onda H, Nomura H, Haji S. Sonographic diagnosis of pancreatic islet cell tumor: value of intermittent harmonic imaging. J Clin Ultrasound 2001; 29:411-6. [PMID 11579405
- Rickes S, Wermke W. Differentiation of cystic pancreatic neoplasms and pseudocysts by conventional and echo-enhanced ultrasound. J GastroenterolHepatol 2004; 19:761-6. [PMID 15209622
- Loperfido S, Angelini G, Benedetti G, Chilovi F, Costan F, De Berardinis F, et al. Major early complications from diagnostic and therapeutic ERCP: a prospective multicenter study. Gastrointest Endosc 1998; 48:1-10. [PMID 9684657
- Bilbao MK, Dotter CT, Lee TG, Katon RM. Complications of endoscopic retrograde cholangiopancreatography (ERCP). Gastroenterology 1976; 70:314-320. [PMID 1248697
- Becker D, Strobel D, Bernatik T, Hahn EG. Echo-enhanced color- and power-Doppler EUS for the discrimination between focal pancreatitis and pancreatic carcinoma. Gastrointest Endosc 2001; 53:784-9. [PMID 11375592
- Hocke M, Gottschalk P, Dietrich CF. KontrastmittelverstärkteEndosonographiezurDifferentialdiagnostik der unklarenPankreasraumforderung. Ultraschall Med 2004; 25(S1):Abstract WS_23_02.
- Schima W, Fugger R, Schober E, Oettl C, Wamser P, Grabenwoger F, et al. Diagnosis and staging of pancreatic cancer: comparison of mangafodipirtrisodium-enhanced MR imaging and contrast-enhanced helical hydro-CT. AJR Am J Roentgenol 2002; 179:717-724. [PMID 12185052
- Papos M, Takacs T, Tron L, Farkas G, Ambrus E, Szakall S Jr, et al. The possible role of F-18 FDG positron emission tomography in the differential diagnosis of focal pancreatic lesions. ClinNucl Med 2002; 27:197-201. [PMID 11852308
- Diehl SJ, Lehmann KJ, Sadick M, Lachmann R, Georgi M. Pancreatic cancer: value of dual-phase helical CT in assessing resectability. Radiology 1998; 206:373-8. [PMID 9457188
- Legmann P, Vignaux O, Dousset B, Baraza AJ, Palazzo L, Dumontier I, et al. Pancreatic tumors; comparison of dual-phase helical CT and endoscopic sonography. AJR Am J Roentgenol 1998; 170:1315-22. [PMID 9574609
- Rosch T, Braig C, Gain T, Feuerbach S, Siewert JR, Schusdziarra V, Classen M. Staging of pancreatic and ampullary carcinoma by endoscopic ultrasound. Gastroenterology 1992; 102:188-199. [PMID 1727753
- Goldstein HM, Neiman HL, Bookstein JJ. Angiography evaluation of pancreatic disease. A further appraisal. Radiology 1974; 112:275-82. [PMID 4835020
- Reuter SR, Redman HC, Bookstein JJ. Differential problems in the angiographic diagnosis of carcinoma of the pancreas. Radiology 1970; 96:93-9. [PMID 5420420
- Appleton GV, Bathurst NC, Virjee J, Cooper MJ, Williamson RC. The value of angiography in the surgical management of pancreatic disease. Ann R CollSurgEngl 1989; 71:92-6. [PMID 2705733
- Koito K, Namieno T, Morita K. Differential diagnosis of small hepatocellular carcinoma and adenomatous hyperplasia with power Doppler sonography. AJR Am J Roentgenol 1998; 170:157-61. [PMID 9423624
- Calliada F, Campani R, Bottinelli O, Bozzini A, Sommaruga MG. Ultrasound contrast agents: basic principles. Eur J Radiol 1998; 27(Suppl):S157-60. [PMID 9652516
- Correas JM, Hélénon O, Pourcelot L, Moreau JF. Ultrasound contrast agents. Examples of blood pool agents. ActaRadiol 1997; 38:101-12. [PMID 9240088
- Kim AY, Choi BI, Kim TK, Kim KW, Lee JY, Han JK. Comparison of contrast-enhanced fundamental imaging, second-harmonic imaging, and pulse-inversion harmonic imaging. Invest Radiol 2001; 36:582-8. [PMID 11577268
- Rosch T, Lightdale CJ, Botet JF, Boyce GA, Sivak MV Jr, Yasuda K, et al. Localization of pancreatic endocrine tumors by endoscopic ultrasonography. N Engl J Med 1992; 326:1721-6. [PMID 1317506
- Hirota T, Tomida T, Iwasa M, Takahashi K, Kaneda M, Tamaki H. Solitary pancreatic metastasis occurring eight years after nephrectomy for renal cell carcinoma: a case report and review of the literature. Int J Pancreatol 1996; 19:145-53. [PMID 8723558
- Thompson LD, Heffess CS. Renal cell carcinoma to the pancreas in surgical pathology material. Cancer 2000; 89:1076-88. [PMID 10964338
- Rickes S, Unkrodt K, Neye H, Ocran K, Lochs H, Wermke W. Differential diagnosis of frequent pancreatic tumors with echo-enhanced power-Doppler sonography - presentation of case reports. Z Gastroenterol 2002; 40:235-40. [PMID 11961732
- Koito K, Namieno T, Ichimura T, Yama N, Hareyama M, Morita K, Nishi M. Mucin-producing tumor of the pancreas: comparison of MR cholangiopancreatography with ER cholangiopancreatography. Radiology 1998; 208:231-7. [PMID 9646818
- Ueno E, Takada Y, Yoshida I, Toda J, Sugiura T, Toki F. Pancreatic diseases: evaluation with MR cholangiopancreatography. Pancreas 1998; 16:418-26. [PMID 9548689
- Rickes S, Uhle C, Kahl S, Kolfenbach S, Mönkemüller K, Effenberger O, Malfertheiner P. Echo-enhanced ultrasound: a new valid initial imaging approach for severe acute pancreatitis. Gut 2006; 55:74-8. [PMID 16033880





