Keywords
Diagnosis, Differential; Endosonography; Pancreatic Neoplasms; Ultrasonography
Abbreviations
EFSUMB: European Federation of Societies for Ultrasound in Medicine and Biology
INTRODUCTION
Contrast enhanced ultrasound (CEUS) has been established for detection and characterisation of liver tumours [1, 2] and solid pancreatic lesions using the transabdominal [3] or endoscopic approach [4]. The previously published guidelines include the use for the differential diagnosis of solid pancreatic lesions. The role of CEUS in cystic pancreatic lesions has not been evaluated so far. The differentiation of pseudocyst from benign and malignant neoplasia remains an unsolved problem today despite improved technology, e.g., computed tomography and magnetic resonance imaging. The gold standard is still surgery with pathological examination of histological specimens. Therefore, a non-invasive method for reliable differentiation between pseudocysts and cystic neoplasia would be highly desirable since surgery could be avoided in some cases.
In the present study transabdominal CEUS using low mechanical index real-time techniques was used for the first time in a large group of patients for the differential diagnosis of the undetermined cystic pancreatic lesion (gold standard: surgery or biopsy yielding histology or cytology).
PATIENTS
Over a period of seven years we prospectively evaluated 127 patients with the definite histological diagnosis of cystic pancreatic lesions using CEUS. In 13/127 patients (10.2%) adequate visualisation of the pancreas was not achieved using CEUS and were, therefore, excluded from study analysis. The ultrasound visualisation rate is in accordance to published data for visualisation of the peripancreatic region and hepatoduodenal ligament [5]. Therefore, 114 patients with undetermined cystic pancreatic lesions were prospectively examined applying a standardised protocol [3, 4] using conventional B-mode and transabdominal CEUS.
Inclusion Criteria for Study Analysis
Inclusion criteria for study analysis were the primarily undetermined cystic pancreatic lesion of any size suspected by transabdominal ultrasound, computed tomography or magnetic resonance imaging. In patients with benign cytology or histology a follow-up examination of at least one year was documented as well. Patients with cystic pancreatic lesions and metastatic disease (e.g., liver, lung) were not included into study analysis since diagnosis was usually achieved by biopsy of the metastatic site. Possible other reasons for exclusion have been former allergic reactions to SonoVue® (Bracco, Milan, Italy) (no patients). Only patients older than 18 years were included into the study.
METHODS
Transabdominal ultrasound was performed using Siemens Acuson Sequoia® platform (Siemens, Erlangen, Germany) in all patients. The pancreas was examined as recently described in the decubitus position, slightly left lateral position and standing position if necessary also applying the trans-splenic approach in all patients [3]. Contrast enhancing agent (SonoVue®, Bracco, Milan, Italy; 2.4 mL) was applied in all patients. All examinations have been performed by one examiner (C.F.D.).
Conventional B-mode, Contrast Enhanced Ultrasound (CEUS)
Cystic tumour location (head, body, tail), size (mm), and echogenicity (echofree, hypoechoic, mixed echogenicity) were documented using conventional Bmode. Solid nodules with and without deriving septae out of the nodule were documented. The presence of identifiable mass lesions within a cyst or a cystic lesion with (peripherally) located solid nodules (with or without septae) were considered indicators for neoplasia. All patients were examined before and after intravenous bolus injection of 2.4 mL SonoVue® (Bracco, Milan, Italy) contrast pulse sequencing followed by a flush of 10 mL saline solution via a catheter of larger than, or equal to, 1.2 mm diameter into a cubital vein. CEUS was performed using the following imaging parameters: mechanical index 0.1- 0.25, power 1-3%, gain 50-80 dB, and frame rate 10-16 sec-1. The pancreas was scanned continuously for up to 5 minutes. Using this approach, contrast enhancing tumour characteristics were evaluated during the arterial phase (up to 40 seconds) identifying vascularity of suspected solid nodules. The reproducibility of the arterial phase in patients with pancreatic tumours was 100% in 20 consecutive patients whereas the delayed phases are difficult to standardize with respect to the mode of application, dosage used, time-point of analysis after the injection [3]. Therefore, the delayed phases (after 40 seconds post injection) were not part of the study.
Vascularisation of a mass lesions or cystic lesion with peripherally located nodules with or without septae (shown by B-mode) were analysed and afterwards assessed by CEUS analysing the contrast enhancement; it was differentiated if a macrovessel was transversing the nodule at the edge of a septum as a sign of preformed vessel transversing the pseudocyst (or necrosis) or microvascularity could be shown within the solid nodule as a sign of neoangiogenesis of neoplasia. Results were compared with histology assuming that pseudocysts (with the exception of individual macrovessels transversing the pseudocyst) in contrast to microvascularised neoplasia do not show contrast enhancement (Figure 1). In addition malignant lesions were assumed to be hypovascular in comparison to the surrounding pancreatic parenchyma according to the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) guidelines [1] and recently published studies [3, 4]. additionally in a few patients positron emission tomography were performed (sometimes using different techniques and, therefore, not comparable) as part of the clinical work-up of at least one procedure in all patients (in several cases outside our institution) and not for the purpose of this study.
Figure 1. B-mode imaging (a.) and contrast enhanced ultrasound
(CEUS) (b.) in a patient with histologically proven pseudocyst of the
pancreas. Small peripherally nodular structures are delineated
(arrow) analysing the arterial phase (b.) indicating neoplasia. Surgery
and consecutive histology revealed pseudocyst and no neoplasia.
Reference Imaging Methods
Reference imaging examinations (e.g. computed tomography, magnetic resonance imaging, and
Histology/Cytology
In all patients, a definite histological or cytological diagnosis was obtained by means of surgical pancreatic resection or fine needle aspiration guided by endoscopic ultrasound.
ETHICS
Institutional board approval according to the ethical guidelines from Helsinki was obtained. Oral informed consent was obtained.
STATISTICS
Dimensions were given as mean and standard deviation (SD) and range if appropriate. Sensitivity was calculated as the rate of true positive results to the sum of true positive and false negative results. Specificity was calculated as the rate of true negative results to the sum of true negative and false positive results. The positive predictive value was calculated as the rate of true positive results to the sum of true positive and false positive results. The negative predictive value was calculated as the rate of true negative results to the sum of true negative and false negative results. The frequency of cases correctly classified was calculated as the rate of the sum of true positive and true negative results to all results.
RESULTS
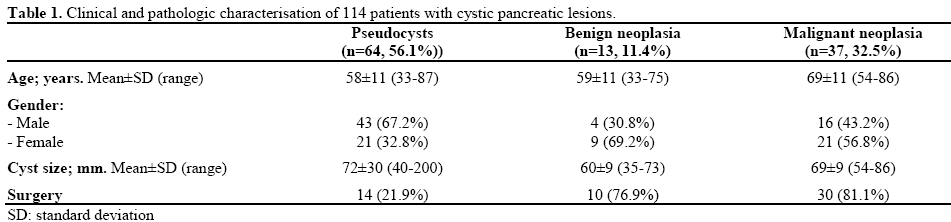
CEUS was performed in 114 patients with undetermined cystic pancreatic lesions (age: 62±12 years; range: 33-87 years). Sixty-four (56.1%) patients had the final diagnosis of pseudocysts (14 operated, 21.9%) and 50 neoplastic cystic lesions: 13 benign (11.4%) and 37 (32.5%) malignant neoplasia. Malignant neoplasia included: 7 patients with pseudocysts caused by chronic pancreatitis and concomitant ductal adenocarcinoma (all operated), and 9 mucinous cystadenocarcinoma (all operated), 13 malignant intraductal papillary mucinous neoplasia (IPMN) (all operated), 2 acinar cell carcinoma (both biopsy and histological confirmation), and 4 malignant neuroendocrine tumours (all 4 biopsy and histological confirmation). In one case a partially cystic solid papillary epithelial neoplasm was found (biopsy, operation). One patient had cystic metastases of a hypernephroma (confirmed by biopsy). The 13 benign neoplasia included: 2 mucinous cystadenoma (both operated), 7 benign IPMN (all operated), and 4 serous oligocystic pancreatic adenoma (one operation and three biopsy and histological confirmation). Patient characteristics are given in Table 1.
Pseudocysts
In all 64 (100%) patients with the final diagnosis of pseudocysts, puncture and drainage was performed using endoscopic ultrasound for diagnostic and therapeutic reasons. In 14 patients (21.9%) surgery was mandatory due to failure of endoscopic treatment. In 3 patients arterial pseudoaneurysms were detected using CEUS, thereof, 2 patients presented with hemosuccus pancreaticus (2 patients have been operated and in one patient radiological intervention was performed). The mean diameter of the pseudocysts was 72±30 mm (range: 40-200 mm).
Using conventional B-mode mostly peripherally located solid nodules (with or without septae formation) were displayed in 36/64 (56.3%) patients implying neoplastic disease. The results are shown in Table 2. In 2/36 (5%) of these patients with nodules at the edge of the cyst and the final diagnosis of pseudocyst contrast enhancement was found in the peripherally located solid nodules (Figure 1) which was the reason for the 2 false positive findings using CEUS in histologically/cytologically proven pseudocysts. The pseudocyst transversing arterial macrovessels could only be identified using CEUS and conventional ultrasound in combination in 13/35 (37.1%) patients.

Ductal Adenocarcinoma and Pseudocysts
Seven patients with a history of chronic pancreatitis and actual pseudocysts in patients with pancreatitis revealed finally ductal adenocarcinoma of the pancreatic head (5 patients), corpus (1 patient), and tail (1 patient). The mean diameter of the lesions was 62±24 mm (range: 40-120 mm). All lesions showed arterial enhancement but less pronounced compared to the surrounding pancreatic parenchyma (Figure 2). Isolated macrovessels transversing the cyst(s) could not be visualised.
Figure 2. B-mode imaging (a.) and contrast enhanced ultrasound
(CEUS) (b.) in a patient with a small partially cystic ductal
adenocarcinoma in a patient with chronic pancreatitis proven by
operation and histology.
Mucinous Cystadenoma
During the study period we examined 11 patients by CEUS with mucinous neoplasia (all except one lesion located in the corpus or tail of the pancreas; 2 benign, 9 malignant; all operated). The mean diameter of the lesions was 61±18 mm (range: 40-83 mm). Using conventional B-mode mostly peripherally located solid nodules were displayed in 9 out of 11 patients (81.8%). Contrast enhancement was found in all 9 nodules (Figure 3). Isolated macrovessels transversing the cyst(s) could not be visualised.
Figure 3. B-mode imaging (a.) and contrast enhanced ultrasound
(CEUS) (b.) in a patient with mucinous cystadenoma displaying the
mainly cystic but partially also solid tumour.
Intraductal Papillary Mucinous Neoplasia (IPMN)
Twenty patients with the final diagnosis IPMN were investigated using CEUS (7 benign, 13 malignant). All
cystic IPMN lesions were located in the head and/or corpus of the pancreas. The mean diameter of the IPMN was 62±18 mm (range: 35-86 mm). Using conventional B-mode solid nodules were displayed in 19/20 (95.0%) patients with the final diagnosis of IPMN. Contrast enhancement was found in all 19 nodules. Isolated macrovessels transversing cyst(s) could not be visualised.
Serous (Oligo) Macrocystic Pancreatic Adenoma
The incidental findings of a cystic pancreatic tumour in four asymptomatic patients turned out to be serous macrocystic adenoma (of the head and corpus of the pancreas in all), one proven by operation and the other three by transabdominal biopsy and histology. The mean tumour diameter was 58±6 mm (range: 50-65 mm). All four lesions revealed solid vascularised nodules and septae including transversing vessels.
Neuroendocrine Tumours
During the study period we examined 4 patients with histologically proven cystic neuroendocrine tumours of the head of the pancreas. The mean tumour diameter was 64±11 mm (range: 52-80 mm). Solid parts of the lesion (representing more than 50% of the whole diameter of the lesion) were identified by conventional B-mode and pronounced contrast enhancement could be displayed by CEUS. Isolated vessels transversing cyst(s) could not be visualised.
Acinar Cell Carcinoma
We investigated 2 patients with histologically proven acinar cell carcinoma of the body and tail of the pancreas. Tumour size was 85 mm and 65 mm. Solid parts of the lesion (representing more than 50% of the whole diameter of the lesion) were identified by conventional B-mode and pronounced contrast enhancement could be displayed by CEUS. Isolated vessels transversing cyst(s) could not be visualised.
Solid Pseudopapillary Tumour of the Pancreas
One patient with a history of chronic pancreatitis had a histologically proven solid pseudopapillary tumour of the pancreatic tail. The tumour size was 85 mm. Solid parts of the lesion (representing more than 50% of the whole diameter of the lesion) were identified by conventional B-mode and pronounced contrast enhancement could be displayed by CEUS. Isolated vessels transversing cyst(s) could not be visualised.
Cystic Metastasis of a Hypernephroma
One patient with no history of chronic pancreatitis had a histologically proven cystic metastasis of a hypernephroma of the pancreatic head and corpus. The tumour size was 40 mm. Solid parts of the lesion (representing more than 50% of the whole diameter of the lesion) were identified by conventional B-mode and pronounced contrast enhancement could be displayed by CEUS. Isolated vessels transversing cyst(s) could not be visualised.
Pancreatic Pseudocysts versus Neoplastic Pancreatic Disease
In total 114 patients were included into the study analysis: 64 patients with final diagnosis of pseudocysts and 50 patients with neoplastic disease. Bmode alone, defining solid nodules within the cystic lesion or at the border with or without septae had a sensitivity of 94.0%, a specificity of 43.8% and 65.8%
CEUS combining contrast enhancement and morphology reached a sensitivity of 94.0%, specificity of 96.9% and an overall correct classification rate of 96.6%. The results, including predictive values, are given in Table 2.
Differential Diagnosis of Benign versus Malignant Cystic Pancreatic Neoplasia
Malignant lesions were assumed to be hypovascular in comparison to the surrounding pancreatic parenchyma according to the EFSUMB guidelines [1] and recently published studies [3, 4]. It has to be taken into account that comparison of tumour enhancement and surrounding pancreatic parenchyma would be only possible in patients without changes of the normal parenchyma (which serves as reference standard). Since most patients (67/114, 58.8%) revealed not only a cystic lesion but also changes of the surrounding pancreatic parenchyma mainly explained by accompanying pancreatitis a differentiation of benign and malignant lesion was not possible using these criteria. In the remaining 47 patients there where no patients with ductal adenocarcinoma (since all patients with ductal adenocarcinoma representing a mixed cystic lesion showed signs of chronic pancreatitis). The 47 patients with solid inflammatory or neoplastic masses showed iso- or hyper-vascularity in comparison to the surrounding (normal) pancreatic parenchyma. For a better understanding of the matter, we added a flow chart with the value of the used criteria (Figure 4).
Figure 4. Flow chart of the value of different criteria to discriminate
pseudocysts from cystic neoplasia.
DISCUSSION
Before analyzing imaging features of cystic pancreatic lesions the clinical work up has to be assessed. In patients with symptomatic pseudocysts puncture and drainage is required mainly depending on the severity of the symptoms. In patients with suspected neoplasia dignity (benign versus malignant) has also to be evaluated to determine the indication and extent for surgery. The role of imaging methods in the differential diagnosis of cystic pancreatic lesions were reported to be disappointing [6] in contrast to promising sonographic results in tumour characterisation of “solid” lesions using the transabdominal and endoscopic approach [1, 3, 4, 7]. The present study focuses on the differential diagnosis of cystic lesions in patients with and without chronic pancreatitis to distinguish between pseudocysts and cystic pancreatic neoplasia. It could be shown that conventional B-mode ultrasound has a high sensitivity and low specificity in the correct diagnosis of cystic neoplasia due to the fact that mass lesions, nodules and septae are easy to recognise by conventional B-mode ultrasound but only analysis of the (micro-)perfusion pattern of the respective mass lesions, nodules and septae helps to raise specificity
In contrast to solid nodules of the pancreas, where CEUS helps to differentiate between ductal adenocarcinoma and other pancreatic neoplastic disease [3], CEUS, as known for other imaging modalities [8], is also not capable to differentiate between benign and malignant cystic neoplasia (without distant metastases) since malignant transformation is not easy to recognise even for pathologist. It has to be taken into account that malignant transformation might be multilocular. As a rule patients with malignant disease are slightly older and the size of the lesion is often larger than in benign cystic neoplasia.
Pseudocysts are the most common cystic lesions of the pancreas. Neoplastic lesions occur in up to 15% of patients with suspected pseudocysts. Detection of (pseudo-)cystic lesions is easy to be made by transabdominal ultrasound and magnetic resonance imaging, whereas computed tomography is less sensitive in identifying cystic lesions. Differentiation between inflammatory pseudocysts and neoplastic disease is difficult for all imaging modalities so far. We could demonstrate that analysing the microperfusion of solid nodules by CEUS can be helpful in discrimination of pseudocysts from neoplastic cystic lesions. The pseudocyst transversing arterial macrovessels are signs of pseudocysts (or necrosis) whereas the detection of microvessels is typical for neoplasia [9, 10] and might lead to false positive results not using sophisticated contrast techniques.
In our findings, cystic neoplasia may show iso- or hyper-vascularisation of the solid parts in comparison to the surrounding pancreatic parenchyma independently of being benign or malignant which is in accordance with the literature [11, 12, 13]. This is true for mucinous cystadenoma (with a high female preponderance with malignant potential at least in tumours with a size greater than 30-50 mm) and IPMN, which all should be resected if possible. In cystadenocarcinoma, operative strategies follow oncological strategies similar to the therapeutical approach of ductal adenocarcinoma. However, the preoperative diagnosis of benign and malignant cystic pancreatic lesions is still an unsolved problem. None of the current imaging methods allows the reliable prediction of malignant transformation. Most cystic neoplasia are hypervascular and hyperenhancing in comparison to the surrounding pancreatic parenchyma. In addition, in patients with cystic lesions chronic pancreatitis is often an accompanying feature which makes it almost impossible to compare the enhancement pattern to normal surrounding pancreatic parenchyma. Preoperative biopsy is helpful only if positive since biopsy can also produce false negative results if specimens obtained are not representative. Several other limitations for the sonographic approach have to be considered. In larger tumours heterogeneity is more prominent and typical tumour features might be overlayed by regressive changes. Transabdominal ultrasound penetration might be limited by meteorism or other causes.
It is of interest that ductal adenocarcinoma of the pancreas is rarely encountered as cystic lesion. It has to be taken into account that chronic pancreatitis displays often cystic parts and calcifications but those lesions were not part of pancreatic carcinoma or found in the direct neighbourhood. The role of endoscopic CEUS techniques in the differential diagnosis of chronic pancreatitis and ductal adenocarcinoma has been recently discussed with promising results depending on the equipment and technique used. In ductal adenocarcinomas only arterial vessels (with higher resistance index in ductal adenocarcinoma compared to chronic pancreatitis) could be displayed using contrast enhanced power Doppler ultrasound in contrast to chronic pancreatitis which displays both arterial and venous vessels using specific equipment [9, 14]. In patients with cystic ductal adenocarcinoma the inflammatory component might be predominant; therefore, the lesion often shows iso- or hypervascularity in comparison to the surrounding parenchyma.
The typical features of autoimmune pancreatitis are the absence of cysts and calcifications and in addition without enlargement of the pancreatic duct. Therefore, autoimmune pancreatitis is not primarily included into differential diagnosis of cystic pancreatic lesions [15, 16]. In addition, patients with pancreatic (non- Hodgkin) lymphoma to our knowledge rarely show cystic parts of the lesions but in all that cases lymphoma was disseminated. Cystic pancreatic metastases of tumours of other origin rarely pose a (differential) diagnostic problem and can be managed without specific knowledge of the additional pancreatic lesion. Cystic metastases of the pancreas have been observed but metastases to other organs causing the leading symptoms and the cystic pancreatic lesions were not of clinical importance. In other patients with pancreatic cysts (such as polycystic disease and adult patients with cystic fibrosis [17]) neoplasia is rarely encountered and is therefore no problem of differential diagnosis.
In conclusion, appropriate management and treatment of cystic pancreatic tumours require highly sensitive and specific imaging techniques. CEUS improves the differentiation between pseudocysts and pancreatic neoplasia in comparison to the conventional B-mode imaging. The microvascularisation visualised using CEUS even in small nodules (with or without septae) associated with cystic lesions is an indicator for cystic pancreatic neoplasia.
Note Drs. Beyer-Enke and Hocke shared first authorship
Conflict of interest
The authors have no potential conflict of interest
References
- Claudon M, Cosgrove D, Albrecht T, Bolondi L, Bosio M, Calliada F, et al. Guidelines and good clinical practice recommendations for contrast enhanced ultrasound (CEUS) - update 2008. Ultraschall Med 2008; 29:28-44. [PMID 18270887]
- Dietrich CF. Comments and illustrations regarding the guidelines and good clinical practice recommendations for contrastenhanced ultrasound (CEUS): update 2008. Ultraschall Med 2008; 29(Suppl 4):S188-202. [PMID 18833497]
- Dietrich CF, Braden B, Hocke M, Ott M, Ignee A. Improved characterisation of solitary solid pancreatic tumours using contrast enhanced transabdominal ultrasound. J Cancer Res Clin Oncol 2008; 134:635-43. [PMID 17952469]
- Dietrich CF, Ignee A, Braden B, Barreiros AP, Ott M, Hocke M. Improved differentiation of pancreatic tumors using contrastenhanced endoscopic ultrasound. Clin Gastroenterol Hepatol 2008; 6:590-7. [PMID 18455699]
- Dietrich CF, Lee JH, Herrmann G, Teuber G, Roth WK, Caspary WF, et al. Enlargement of perihepatic lymph nodes in relation to liver histology and viremia in patients with chronic hepatitis C. Hepatology 1997; 26:467-72. [PMID 9252160]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic neoplasms: a report of the cooperative pancreatic cyst study. Gastroenterology 2004; 126:1330-6. [PMID 15131794]
- D'Onofrio M, Martone E, Malago R, Faccioli N, Zamboni G, Comai A, et al. Contrast-enhanced ultrasonography of the pancreas. JOP. J Pancreas (Online) 2007; 8(1 Suppl):71-6. [PMID 17228138]
- D'Onofrio M, Megibow AJ, Faccioli N, Malago R, Capelli P, Falconi M, et al. Comparison of contrast-enhanced sonography and MRI in displaying anatomic features of cystic pancreatic masses. AJR Am J Roentgenol 2007; 189:1435-42. [PMID 18029882]
- Hocke M, Schulze E, Gottschalk P, Topalidis T, Dietrich CF. Contrast-enhanced endoscopic ultrasound in discrimination between focal pancreatitis and pancreatic cancer. World J Gastroenterol 2006; 12:246-50. [PMID 16482625]
- Dietrich CF, Jenssen C, Allescher HD, Hocke M, Barreiros AP, Ignee A. Differential diagnosis of pancreatic lesions using endoscopic ultrasound. Z Gastroenterol 2008; 46:601-17. [PMID 18537088]
- Rickes S, Monkemuller K, Malfertheiner P. Echo-enhanced ultrasound with pulse inversion imaging: A new imaging modality for the differentiation of cystic pancreatic tumours. World J Gastroenterol 2006; 12:2205-8. [PMID 16610022]
- Rickes S, Randhan W, Malfertheiner P. Differentiation of cystic pancreatic lesions by echo-enhanced sonography with pulse inversion imaging - presentation of case reports. Z Gastroenterol 2004; 42:317-21. [PMID 15095122]
- Rickes S, Malfertheiner P. Echo-enhanced sonography--an increasingly used procedure for the differentiation of pancreatic tumors. Dig Dis 2004; 22:32-8. [PMID 15292693]
- Hocke M, Ignee A, Topalidis T, Stallmach A, Dietrich CF. Contrast-enhanced endosonographic Doppler spectrum analysis is helpful in discrimination between focal chronic pancreatitis and pancreatic cancer. Pancreas 2007; 35:286-8. [PMID 17895854]
- Hirche TO, Ignee A, Barreiros AP, Schreiber-Dietrich D, Jungblut S, Ott M, et al. Indications and limitations of endoscopic ultrasound elastography for evaluation of focal pancreatic lesions. Endoscopy 2008; 40:910-7. [PMID 19009483]
- Dietrich CF, Hirche TO, Ott M, Ignee A. Real-time tissue elastography in the diagnosis of autoimmune pancreatitis. Endoscopy 2009; 41:718-20. [PMID 19618344]
- Dietrich CF, Chichakli M, Hirche TO, Bargon J, Leitzmann P, Wagner TO, Lembcke B. Sonographic findings of the hepatobiliary pancreatic system in adult patients with cystic fibrosis. J Ultrasound Med 2002; 21:409-16. [PMID 11934098]





