Keywords
Hyperinsulinemic hypoglycemia, KCNJ11 gene, homozygous
(p.E126K) mutation
INTRODUCTİON
Hyperinsulinism is the most frequent cause of both
transient and persistent hypoglycemia in the neonatal
period [1]. Biochemically, congenital hyperinsulinism is
the inappropriate release of insulin from pancreatic β-cells
despite hypoglycaemia. Its incidence is estimated to be 1:
40,000 to 50,000 in outbred populations [2]. However, it
has an incidence up to 1: 2,500 in some populations where
consanguinity is widely practiced [3]. Hyperinsulinism
due to mutations in the KCNJ11 and ABCC8 genes which
encode the pancreatic ATP-sensitive potassium [KATP]
channel are the most common cause of hyperinsulinism.
Histologically two different forms are recognised, diffuse
and focal, with the diffuse form commonly inherited in an
autosomal recessive manner. In contrast focal disease is
usually sporadic. Patients with KATP channel mutations
are often born macrosomic with severe hypoglycemia
usually presenting immediately after birth [4, 5].
The diagnosis of congenital hyperinsulinism is made
according to the following criteria: hyperinsulinemia (plasma insulin >2μU/mL), plasma free fatty acid level
<1.5 mmol/L, hypoketonemia (plasma ß-hydroxi butirate
level <2 mmol/L) in blood samples obtained during
hypoglycemia (glucose <50 mg/dL), and excessive
glycemic response to glucagon (delta glucose >30 mg/dL
by 1 mg intravenous glucagon). A lack of ketosis during
hypoglycemia can exclude many causes of hypoglycemia
including insufficient calorie intake, hypopituitarism,
adrenal insufficiency, congenital enzyme defects,
galactosemia, and fructosemia [6].
CASE REPORT
An eight-day old boy with a birth weight of 4,550
g born to a 32-year old female with diabetes mellitus
was admitted to our neonatal intensive care unit with
respiratory distress syndrome, congenital heart disease
and hypoglycemia (glucose 32 mg/dL). His parents were
second-degree cousins and there was no known history of
disease in the family. Physical examination revealed the
following findings: weight: 4,550 g (>97 percentile); height:
50 cm (25 to 50 percentile); and head circumference: 35
cm (25 to 50 percentile). Systemic examination showed
that the patient was tachypneic and dyspneic with a
respiratory rate of 80/bpm, and heart rate of 160/
bpm. There was no abnormal finding other than systolic
murmur. Patent ductus arteriosus, atrial septal defect, and
focal septal hypertrophy (non-obstructive) were detected
on an echocardiogram. Mechanical ventilation was then
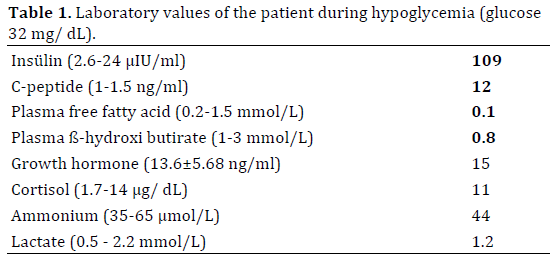
initiated. In the referral facility, glucose infusion (6 mg/kg/min) was initiated and was subsequently increased to
10 mg/kg/min due to the persistence of hypoglycemia . A
diagnosis of congenital hyperinsulinism was made based
on the presence of elevated serum insulin-c-peptide levels
(109 μIU/ml [2.6-24] and 12 ng/ml [1-1.5], respectively)
during hypoglycemia (Table 1). Levels of serum growth
hormone, cortisol, ammonium, and lactate were normal.
Metabolic screening tests for blood and urine ketones and
fatty acid oxidation defects were also found to be normal.
Glucose infusion (14 mg/kg/min), glucagon infusion, and
diazoxide (initially 5 mg/kg which increased up to 20 mg/
kg) were initiated but glycemic control was only achieved
when octreotide and nifedipine were intoduced to the
treatment regimen (final doses were 30 μg/kg and 1.5 mg/
kg/day, respectively). An 18F-DOPA-PET CT scan was not
performed as this is currently not available in our country.
Although nasogastric feeding was initiated, the
patient was unable to tolerate total enteral nutrition. He
was unable to be extubated and his neuorolgical status
deteriorated. There was diffuse edematous cerebral
hemispheres in cranial magnetic resonance imaging (MRI).
Glycemic control was provided but he was died because of
respiratory insufficiency.
Molecular Analysis
ABCC8 and KCNJ11 mutation analyses were performed
on genomic DNA extracted from the peripheral blood.
A novel homozygous missense mutation (p.E126K) was
detected in the KCNJ11 gene, confirming the diagnosis
of congenital hyperinsulinism (genetic analysis was
performed at the University of Exeter Medical School,
Molecular Genetics, Exeter, UK). His unaffected parents
were both heterozygous carriers of the same mutation.
DİSCUSSİON
Hyperinsulinism is the most common cause of
persistent hypoglycemia in the neonatal period and early
childhood. It is a heterogeneous disease in terms of the
genetic, clinical and histological findings.
Genes in which mutations are known to cause
congenital hyperinsulinism include ABCC8, KCNJ11, GLUD1,
GCK, HADH, SLC16A1 and HNF4A [7]. In one study ABCC8 gene mutations were reported in 45% of the affected
individuals, whilst mutations in KCNJ11 were found in 5%
of patients [8]. These two genes encode the sulfonylurea
receptor 1 (SUR-1) subunit and the inwardly rectifying
potassium channel subunit (Kir6.2) of the pancreatic KATP
channel respectively. Loss-of-function mutations in these
genes result in hyperinsulinism where insulin is secreted
regardless of the plasma glucose level.
In our case, a homozygous p.E126K mutation
was detected in KCNJ11, confirming congenital
hyperinsulinism. Although this mutation is present in the
database of the center where the genetic studies were
performed, having been identified in an unrelated patient
with congenital hyperinsulinism, it has not reported in the
literature to date.
Hyperinsulinism due to KCNJ11 and ABCC8 mutations
are the most common cause of hyperinsulinism and result
in the most clinically severe phenotype. Hyperinsulinism
due to K-ATP channel mutations can result in either diffuse or
focal histological disease. The identification of a homozygous KCNJ11 mutation is in keeping with diffuse disease in our
patient. Patients with K-ATP channel mutations are often
born macrosomic with severe hypoglycemia diagnosed
immediately after birth [4, 5]. Our case with KATP channel
hyperinsulinism was also a macrosomic infant with severe
hyperglycemia presenting early.
Diazoxide treatment is ineffective in the majority of
cases with K-ATP channel mutations as the drug exerts
its effects by binding to and opening the KATP channel.
However, of two cases reported by Shimomura et al. [9],
no response was achieved with diazoxide treatment in
one case who had a paternally inherited heterozygous T294M mutation in KCNJ11 whilst another case with the
same heterozygous mutation inherited by their unaffected
mother responded to treatment. Ilamaran et al. [10] also
reported a good response to diazoxide treatment in a case
with a KCNJ11 mutation suggesting that some cases with
these mutations are amenable to treatment with diazoxide.
For some patients with K-ATP channel mutations who
do not respond to diazoxide introduction of additional
therapies such a Octreotide and Nifedipine can result in
normoglycaemia [11]. In keeping with this our case who
was refractory to diazoxide treatment acheived good
glycemic control when treated with a combination of
octreotide and nifedipine.
CONCLUSİON
In conclusion, hyperinsulinism is the most common
cause of persistent hypoglycemia in the neonatal period.
A novel homozygous KCNJ11 missense mutation (p.E126K)
was detected in our case, which resulted in hyperinsulinism.
Statement of Human and Animal Rights
This manuscript does not contain any studies with
human or animal subjects performed by the any of the
authors.
Acknowledgments
SEF has a Sir Henry Dale Fellowship jointly funded
by the Wellcome Trust and the Royal Society (Grant
Number:105636/Z/14/Z).
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Stanley CA. Hyperinsulinism in infants and children. Pediatr Clin North Am 1997; 44:363-374. [PMID: 9130925]
- Fournet JC, Junien C. The genetics of neonatal hyperinsulinism. Horm Res 2003; 59:30-34. [PMID: 12566718]
- Flanagan SE, Clauin S, Bellanné-Chantelot C, de Lonlay P, Harries LW, Gloyn AL, Ellard S. Update of mutations in the genes encoding the pancreatic beta-cell KATP subunits Kir6.2 (KCNJ11) and sulfonylurea receptor (ABCC8) in diabetes mellitus and hyperinsulinism. Hum Mutat 2009; 30:170-180. [PMID: 18767144]
- Palladino AA, Bennett MJ, Stanley CA. Hyperinsulinism in infancy and childhood: when an insulin level is not always enough. Ann Biol Clin (Paris) 2009; 67:245-254. [PMID: 19411227]
- DeLeon DD, Stanley CA. Mechanisms of disease: advances in diagnosis and treatment of hyperinsulinism in neonates. Nat Clin Pract Endocrinol Metab 2007; 3:57-68. [PMID: 17179930]
- De Leon DD, Stanely CA, Sperling MA. Hypoglycemia in Neonates
and Infants. In: Sperling MA (ed). Pediatric Endocrinology, 3rd ed.
Philedelphia: Saunders Elsevier Co; 2008:166-193.
- James C, Kapoor RR, Ismail D, Hussain K. The genetic basis of congenital hyperinsulinism. J Med Genet 2009; 46:289-299. [PMID: 19254908]
- Glaser B. Familial Hyperinsulinism 2005. [PMID: 20301549]
- Shimomura K, Flanagan S, Zadek B, Lethby M, Zubcevic L, Girard
CA, Petz O, et al. Adjacent mutations in the gating loop of Kir6.2 produce
neonatal diabetes and hyperinsulinism. EMBO Mol Med 2009; 1:166-177.
[PMID: 20049716]
- Ilamaran V, Venkatesh C, Manish K, Adhisivam B. Persistent
hyperinsulinemic hypoglycemia of infancy due to homozygous KCNJ11
(T294M) mutation. Indian J Pediatr 2010; 77:803-804. [PMID: 20589481]
- Durmaz E, Flanagan SE, Parlak M, Ellard S, Akcurin S, Bircan
I. A combination of nifedipine and octreotide treatment in an
hyperinsulinemic hypoglycemic infant. J Clin Res Pediatr Endocrinol
2014; 6:119-121.

