Benjamin Kasenda1,6, Annatina Bass1, Dieter Koeberle2, Bernhard Pestalozzi3, Markus Borner4,
Richard Herrmann1, Lorenz Jost5, Andreas Lohri5, Viviane Hess1
1Department of Medical Oncology, University Hospital Basel, 4031 Basel, Switzerland
2Department of Medical Oncology, Cantonal Hospital of St. Gallen, 9007 St. Gallen, Switzerland
3Department of Medical Oncology, University Hospital of Zurich, 8091 Zurich, Switzerland
4Department of Medical Oncology, University Hospital of Berne, 3010 Berne, Switzerland
5Department of Medical Oncology, Cantonal Hospital Basel-Country, 4101 Basel-Country, Switzerland
6Royal Marsden Hospital, Department of Medicine, Royal Marsden NHS Foundation Trust, Sutton, UK
- *Corresponding Author:
- Benjamin Kasenda
Department of Medical Oncology
University Hospital Basel
Petersgraben 4
Basel CH-4031, Switzerland
Phone +41 (0)61 265 50 74
Fax +41 (0)61 265 53 16
E-mail :benjamin.kasenda@gmail.com/benjamin.kasenda@usb.ch
Received August 20th, 2015 – Accepted October 07th, 2015
Keywords
Pancreatic Neoplasms; Prognosis; Survival Analysis
Abbreviations
ECOG PS Eastern Cooperative Oncology Group performance status; CS conditional survival
INTRODUCTION
Advanced pancreatic adenocarcinoma is the fifth leading cause of cancer-related deaths and carries a devastating prognosis with 5-year survival rates of 6% [1, 2]. Incidence increases with age and most cases are diagnosed above the age of 50 at an unresectable stage [3]. Obesity, red meat consumption, and smoking are risk factors for the development of pancreatic cancer [4, 5]. Gemcitabine based therapies [6-8] are treatment options in the palliative setting; younger patients with a good performance status can benefit from more intense treatment [9].
Survival prognosis is usually estimated from a certain time point e.g. from diagnosis or from start of treatment until death. Such predictions are helpful for making informed treatment decisions, and also end-of life planning in advanced situations. However, these estimated prognoses might lose their validity once a patient has survived for a longer period than predicted. For example, if a patient’s 2 year-survival prognosis under a certain therapy was estimated to be 50% at the time of diagnosis, but she/he is still alive after 3 years, how should we counsel her/him regarding further prognosis? Conditional survival (CS) can provide guidance for such situations; it is defined as the probability of surviving an additional period of time given the patient has already survived a certain period of time. Therefore it provides a powerful tool to dynamically adjust prognosis during the course of disease. Conditional survival has been investigated in other malignancies such as breast cancer [10], colon cancer [11], gastric cancer [12], renal cell carcinoma [13] and also pancreatic cancer [14-17]. However, especially for pancreatic cancer, CS was either calculated based only on patients with resectable disease [15-17], or if patients with unresectable disease were included, data were obtained from registries [14].
To our best knowledge, CS has not been investigated in advanced pancreatic cancer based on clinical data including important baseline characteristics such as CA 19-9 and clinical performance status. We sought to close this knowledge gap based on patients from a national multicentre cohort.
PATIENTS AND METHODS
Eligibility Criteria and Study Design
All patients with stage III/IV pancreatic adenocarcinoma irrespective of age, clinical performance status or therapy modality, who were diagnosed and treated at four Swiss medical centres were included. Patients with stage III disease undergoing curative surgery were excluded. Routine clinical data were retrospectively collected using a pre-specified case report form that recorded anonymized data on patient and tumour characteristics at baseline, treatment, and follow-up. All identified eligible patients from the centres were included. Data were checked for consistency and queries re-checked with the corresponding centre before entering the data in our central database. The local ethics committees approved this study.
Statistical Considerations
The main outcome was 6-month CS, which was defined as the probability to survive another 6 months given that the patient has already survived a certain time after diagnosis – in other words, the probability of surviving at least 6 more months is a function of the number of months a patient has already survived since diagnosis. We analysed CS using a landmark analysis approach as previously reported [18, 19]; survival times were calculated from the landmark time points until death or censoring. In example, to calculate 6-month CS at the 6-month landmark, we set the time zero at 6 months after diagnosis and excluded all patients who i) had died before reaching the 6-month landmark and ii) who had been followed-up less than 6 months from diagnosis. We built four patient subsets according to landmark times at 0 (baseline, all patients), 6, 12, 18, and 24 months after diagnosis. For each set we separately calculated 6-month CS using the Kaplan-Meier method. The landmark time points were chosen arbitrarily, however, 6 months intervals represent a reasonable choice for counselling patients with unresectable pancreatic cancer. CA 19-9 and performance status have previously been identified as important independent prognostic baseline factors [20, 21]. In these two independent cohorts, the median CA 19-9 value showed strong and independent prognostic impact. Based on this evidence, we explored whether CA 19-9 (above median versus below median) and Eastern Cooperative Oncology Group performance status (ECOG PS) (<2 vs. ≥2) at diagnosis were of prognostic value in the 4 patient subsets at each landmark time point. Unadjusted survival rates (Kaplan-Meier estimator) were compared using the log-rank test; we calculated 95% confidence intervals (CI) and a p value of <0.05 (two-sided) was considered significant. For all analyses, missing data were imputed using multiple imputations [22, 23]; frequencies of missing values are presented with the patient characteristics. We used STATA (Texas, USA) to impute missing values; based on the imputed dataset we used the statistical program R version 2.15.3 (www.rproject. org) for all analyses and creating the graphs.
RESULTS
Patient Characteristics
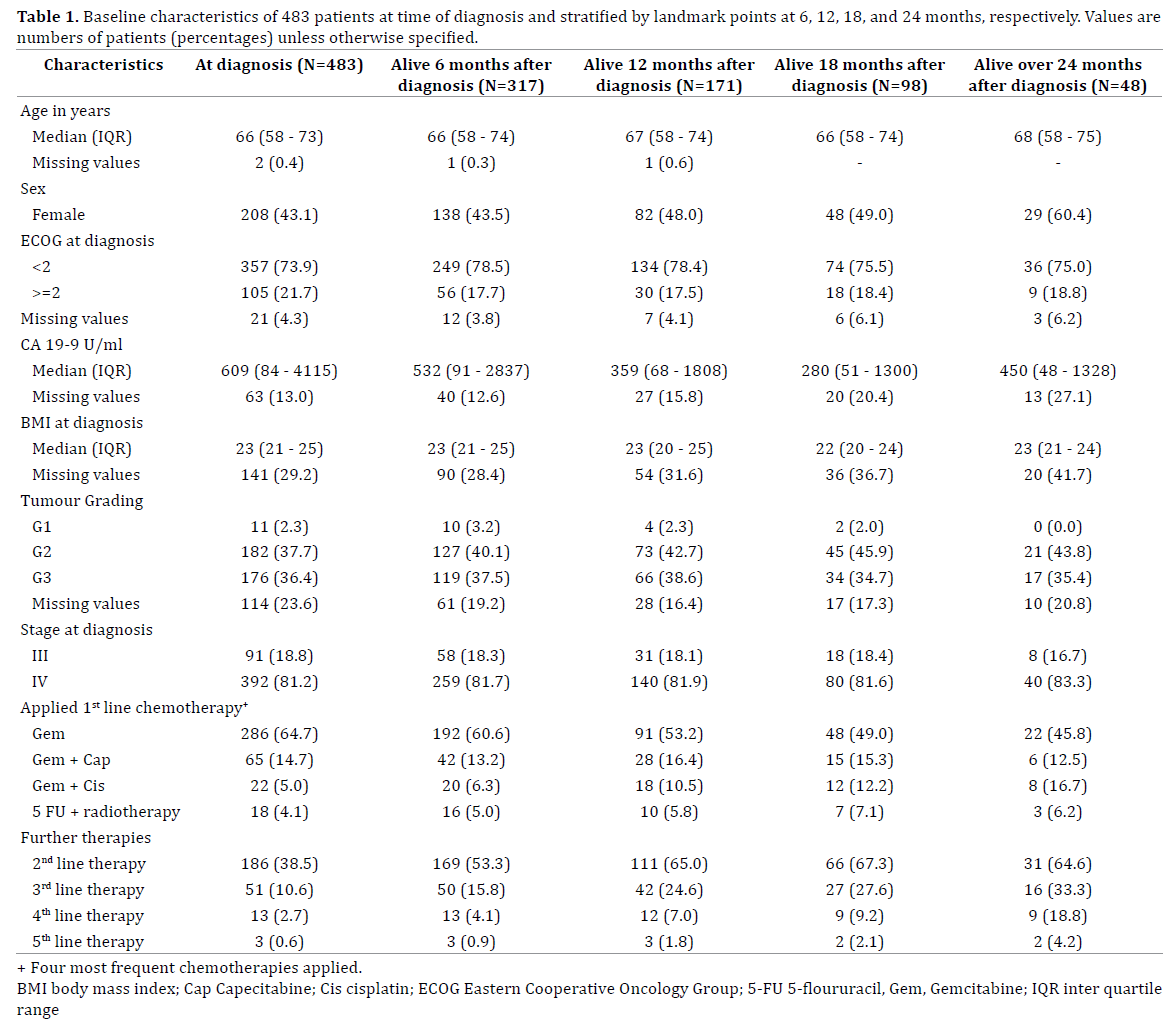
All 483 patients with advanced pancreatic cancer treated between 1994 and 2004 at 4 Swiss Oncology Centres were included in our analyses; characteristics are summarized in Table 1. The majority was diagnosed with stage IV disease; 14 patients (4%) were treated with best supportive care only. Most patients underwent first-line treatment with gemcitabine single agent (N = 286; 59%) or in combination with capecitabine (N = 65; 14%), or cisplatin (N = 22; 5%) (Table 1).
Overall Survival
Figure 1a illustrates the OS probability calculated from baseline. After a median follow-up of 8.5 months (interquartile range 2 – 15 months), 448 patients (93%) had died. Six and 12-month survival probabilities of the whole cohort were 67% (95% CI 63%-71%) and 37% (95% CI 33%-42%), respectively. As expected [20, 21], patients with a high CA 19-9 level or low clinical performance status at diagnosis had a significantly worse OS prognosis (Figure 1b and 1c).
Figure 1. (a.). Overall survival of the whole cohort. (b.). Overall survival
grouped by the Eastern Cooperative Oncology Group score (ECOG). (c.). Overall survival grouped by CA 19-9 baseline level.
Conditional Survival
Figure 2a illustrates the 6-month CS at the respective landmark points over time. At time of diagnosis (baseline), 6-month survival was 67% (95% CI, 63%-71%). For those patients being alive 6 months after diagnosis, 6-month CS was 56% (95% CI; 50%-62%). For those patients still being alive at 12, 18, and 24 months the respective 6-month CS was 58% (95% CI, 51%-66%), 52% (95% CI, 43%-63%), and 71% (95% CI, 58%-85%). The number of patients to calculate the 6-month CS continuously decreases over time, therefore the width of the 95% CIs steadily grows, which illustrates the growing uncertainty of the estimated 6-month CS over time. 6-month CS among patients with good performance status at diagnosis (ECOG PS<2, N=378) was similar to that of the overall population; patients with worse performance status (ECOG PS ≥2, N=105) revealed some improvement over time regarding their 6-month CS (Figure 2b). However, especially for the latter group, the uncertainty of 6-month CS estimates are much larger compared to patients with a better performance status, which is explained by the smaller number of patients with ECOG PS ≥2 at baseline (105/483, 22%). CA 19-9 levels (dichotomized by the median) were of prognostic value at diagnosis and the 6-month landmark, but over time, there was no difference between the groups as illustrated by the widely overlapping 95% CIs (Figure 2c).
Figure 2. The figure illustrates the 6-months conditional survival at the
landmarks 6, 12, 18, and 24 months after diagnosis. Patients being alive at
the respective landmark time points were included for calculation of the
6-months conditional survival thereafter. The horizontal lines depict the
95% confidence interval limits around the 6-months conditional survival
estimate. (a.). Whole cohort. (b.). Stratified by the Eastern Cooperative
Oncology Group score (ECOG). (c.). Stratified by CA 19-9 level at diagnosis.
Comparison to an Online Calculator
Table 2 summarizes 6-month CS provided by a registry-based online calculator compared to our data [14]. The developers of this calculator used registry data and calculated cancer-specific mortality; patients dying from other causes were censored [14]. Although we have specified baseline characteristics representative for our cohort for the online calculation, the provided CS clearly differed from our calculations. In example, the estimated CS at the landmark of 6 months is 38% based on the online calculator, whereas our calculations provide an estimate of 56%. At the 12-month landmark, the online calculator provides an estimate of 44%, which is still lower compared to 58% from our calculations (Table 2).

DISCUSSION
Summary of Findings
Six-month CS for patients with advanced pancreatic cancer remains stable and above 50% during the first two years after diagnosis. It may improve only for those very few patients who have survived 24 months after diagnosis. Our results are in contrast to a registry-based online calculator; particularly regarding CS estimates during the first 18 months. CA 19-9 serum levels and ECOG PS evaluated at diagnosis lose their prognostic relevance over time.
Strengths and Limitations
Our investigations are based on a large set of clinical data of patients with advanced pancreatic cancer. The availability of baseline prognostic factors such as ECOG PS and CA 19-9 serum levels allowed for assessing whether these markers keep their prognostic relevance during follow-up. These factors have not been included in previous CS analyses of patients with advanced pancreatic cancer. Because of the retrospective setting, however, some values of baseline prognostic factors including CA 19-9 serum levels and ECOG PS were missing. To circumvent any loss of power or risk of bias, and to use all available information in our dataset, we applied multiple imputations to impute missing values. This approach has been proposed as a remedy for such situations and its incorporation into routine practice has been recommended to avoid biased estimates [22, 24, 25]. Another limitation is that we were not able to investigate whether patients who received further lines of treatment had better CS, because time points of initiation of later line therapies were not available. Also, inherent to the natural course of this deadly disease, patients have died quickly; therefore, although the overall number of patients (N=483) was large, the uncertainty of our CS estimates at later landmarks grew steadily, because of the decreasing number of patients available to calculate CS. All these limitations need to be considered when applying our results in patient consultations.
Compared to Other Studies
Katz et al developed a registry-based online tool to calculate CS for all stages of pancreatic cancer. Data used for the development of this calculator were taken from the SEER database including 37’135 registered patients being diagnosed with pancreatic adenocarcinoma between 1988 and 2005 [14]. The strength of this study is the large number of patients, which allows for precise estimates. However, important clinical risk factors such as clinical performance status and CA 19-9 serum levels were not available, because such data are not collected in the SEER registry. Overall, the median survival in the patient group with unresectable pancreatic cancer (stage III and IV, N=24’520) was much lower compared to our cohort (below 6 months versus 9.1 months, 95% CI 8.1– 10.0). Possible explanations for this difference may be an improved pattern of care over the last decades, differences in access to health care providers or socio-economic status [26, 27]. 6-month CS estimates especially at the 6 and 12 months landmarks largely differed compared to our data. However, 6-month CS at 18 months after diagnosis was similar [14]. For patients still alive 24 months after diagnosis, the online calculator did not provide 6-month CS estimates.
Our finding that baseline prognostic factors can lose their validity over time is in line with studies investigating CS in lymphoma [28] and colon cancer [29] where survival prognosis based on baseline measures also converged in long-term survivors. In contrast to this, another recent study on renal cell carcinoma patients revealed that Heng risk group risk stratification retained its value over time from three to 18 months. However, there was also a trend towards convergence in the subset of patients with poor risk factors who remained on first-line targeted therapy for long periods of time [13]. In summary, all these findings support that survival prognosis should be regarded as a dynamic process over time.
Calculations of Conditional Survival
Conditional survival is derived from the concept of conditional probability in statistics. For example, to compute the 5-year CS for a patient who has already survived 2 years, the survival probability at 5 + 2 years, S(7), is divided by the survival probability at 2 years, S(2). This is the traditional definition of CS; it takes into account how long someone has survived. However, as outlined by Zamboni et al, this traditional approach does not take into account e.g. present disease status relative to recurrence or second primary cancer [29]. Therefore, in recent publications, investigators extended the CS concept using the landmark approach [13, 29, 30], which we have applied herein. This approach is more flexible compared to the traditional technique, because one can condition on a specific set of patients alive and e.g. free of recurrence or progression, or still on a certain treatment – thus much more detailed clinical information can be included to calculate CS. However, if one only conditions on survival status at a certain time point, CS estimates of the landmark approach or the traditional CS technique provide almost identical information.
CONCLUSION
Survival prognosis based on characteristics at diagnosis do not account for the dynamic development of survival prognosis over time and are therefore not very useful for counselling during follow-up. Clinicians know that the longer a patient lives, the longer she/he is expected to live; however, formally calculated CS estimates are often not at hand to be shared with patients. In contrast to previous reports, 6-month CS from our cohort of patients with advanced pancreatic cancer remains stable and above 50% for the first two years after diagnosis. Our results provide important information for counselling patients and families regarding survival prognosis during treatment and follow-up.
Funding
This work was supported by the Swiss Cancer League/ Oncosuisse (KLS-01881-04-2006 to V.H.) and by the Swiss National Science Foundation (PP00P3_139155/1 to V.H.).
Conflict of Interest
The authors have declared no conflicts of interest.
References
- Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Global cancer statistics. CA Cancer J Clin 2011; 61: 69-90 . [PMID: 21969133]
- Ferlay J, Parkin DM, Steliarova-Foucher E. Estimates of cancer incidence and mortality in Europe in 2008. Eur J Cancer 2010; 46: 765-781 . [PMID: 20116997]
- Hawes RH, Xiong Q, Waxman I, Chang KJ, Evans DB, Abbruzzese JL. A multispecialty approach to the diagnosis and management of pancreatic cancer. Am J Gastroenterol 2000; 95: 17-31. [PMID: 10638554]
- Li D, Morris JS, Liu J, Hassan MM, Day RS, Bondy ML et al. Body mass index and risk, age of onset, and survival in patients with pancreatic cancer. JAMA 2009; 301: 2553-2562. [PMID: 2760963]
- Larsson SC, Wolk A. Red and processed meat consumption and risk of pancreatic cancer: meta-analysis of prospective studies. Br J Cancer 2012; 106: 603-607. [PMID: 3273353]
- Sultana A, Smith CT, Cunningham D, Starling N, Neoptolemos JP, Ghaneh P. Meta-analyses of chemotherapy for locally advanced and metastatic pancreatic cancer. J Clin Oncol 2007; 25: 2607-2615 . [PMID: 18577990]
- Cunningham D, Chau I, Stocken DD, Valle JW, Smith D, Steward W et al. Phase III randomized comparison of gemcitabine versus gemcitabine plus capecitabine in patients with advanced pancreatic cancer. J Clin Oncol 2009; 27: 5513-5518 . [PMID: 19858379]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M et al. Increased survival in pancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl J Med 2013; 369: 1691-1703 . [PMID: 24131140]
- Conroy T, Desseigne F, Ychou M, Bouche O, Guimbaud R, Becouarn Y et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N Engl J Med 2011; 364: 1817-1825 . [PMID: 21561347]
- Christensen LH, Engholm G, Ceberg J, Hein S, Perfekt R, Tange UB et al. Can the survival difference between breast cancer patients in Denmark and Sweden 1989 and 1994 be explained by patho-anatomical variables?--a population-based study. Eur J Cancer 2004; 40: 1233-1243 . [PMID: 15110888]
- Merrill RM, Henson DE, Ries LA. Conditional survival estimates in 34,963 patients with invasive carcinoma of the colon. Dis Colon Rectum 1998; 41: 1097-1106 . [PMID: 9749492]
- Wang SJ, Emery R, Fuller CD, Kim JS, Sittig DF, Thomas CR. Conditional survival in gastric cancer: a SEER database analysis. Gastric Cancer 2007; 10: 153-158 . [PMID: 17922092]
- Harshman LC, Xie W, Bjarnason GA, Knox JJ, MacKenzie M, Wood L et al. Conditional survival of patients with metastatic renal-cell carcinoma treated with VEGF-targeted therapy: a population-based study. Lancet Oncol 2012; 13: 927-935 . [PMID: 3856362]
- Katz MH, Hu CY, Fleming JB, Pisters PW, Lee JE, Chang GJ. Clinical calculator of conditional survival estimates for resected and unresected survivors of pancreatic cancer. Arch Surg 2012; 147: 513-519 . [PMID: 22351874]
- Mayo SC, Nathan H, Cameron JL, Olino K, Edil BH, Herman JM et al. Conditional survival in patients with pancreatic ductal adenocarcinoma resected with curative intent. Cancer 2012; 118: 2674-2681 . [PMID: 3578343]>
- Mishra MV, Champ CE, Keith SW, Showalter TN, Anne PR, Lawrence YR et al. Conditional survival probabilities for patients with resected pancreatic adenocarcinoma. Am J Clin Oncol 2014; 37: 107-111 . [PMID: 23111364]
- Kent TS, Sachs TE, Sanchez N, Vollmer CM, Jr., Callery MP. Conditional survival in pancreatic cancer: better than expected. HPB (Oxford) 2011; 13: 876-880 . [PMID: 3244627]
- Dafni U. Landmark analysis at the 25-year landmark point. Circ Cardiovasc Qual Outcomes 2011; 4: 363-371 . [PMID: 21586725]
- Anderson JR, Cain KC, Gelber RD. Analysis of survival by tumor response and other comparisons of time-to-event by outcome variables. J Clin Oncol 2008; 26: 3913-3915 . [PMID: 18711176]
- Hess V, Glimelius B, Grawe P, Dietrich D, Bodoky G, Ruhstaller T et al. CA 19-9 tumour-marker response to chemotherapy in patients with advanced pancreatic cancer enrolled in a randomised controlled trial. Lancet Oncol 2008; 9: 132-138 . [PMID: 18249033]
- Maisey NR, Norman AR, Hill A, Massey A, Oates J, Cunningham D. CA19-9 as a prognostic factor in inoperable pancreatic cancer: the implication for clinical trials. Br J Cancer 2005; 93: 740-743 . [PMID: 2361637]
- Spratt M, Carpenter J, Sterne JA, Carlin JB, Heron J, Henderson J et al. Strategies for multiple imputation in longitudinal studies. Am J Epidemiol 2010; 172: 478-487 . [PMID: 20616200]
- Kenward MG, Carpenter J. Multiple imputation: current perspectives. Stat Methods Med Res 2007; 16: 199-218 . [PMID: 17621468]
- Klebanoff MA, Cole SR. Use of multiple imputation in the epidemiologic literature. Am J Epidemiol 2008; 168: 355-357 . [PMID: 2561989]>
- Sterne JA, White IR, Carlin JB, Spratt M, Royston P, Kenward MG et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ 2009; 338: b2393 . [PMID: 2714692]
- De Angelis R, Sant M, Coleman MP, Francisci S, Baili P, Pierannunzio D et al. Cancer survival in Europe 1999-2007 by country and age: results of EUROCARE--5-a population-based study. Lancet Oncol 2014; 15: 23-34 . [PMID: 24314615]
- Coleman MP, Quaresma M, Berrino F, Lutz JM, De Angelis R, Capocaccia R et al. Cancer survival in five continents: a worldwide population-based study (CONCORD). Lancet Oncol 2008; 9: 730-756 . [PMID: 18639491]
- Moller MB, Pedersen NT, Christensen BE. Conditional survival of patients with diffuse large B-cell lymphoma. Cancer 2006; 106: 2165-2170 . [PMID: 16586498]
- Zamboni BA, Yothers G, Choi M, Fuller CD, Dignam JJ, Raich PC et al. Conditional survival and the choice of conditioning set for patients with colon cancer: an analysis of NSABP trials C-03 through C-07. J Clin Oncol 2010; 28: 2544-2548 . [PMID: 2881729]
- van Houwelingen HC, Putter H. Dynamic predicting by landmarking as an alternative for multi-state modeling: an application to acute lymphoid leukemia data. Lifetime Data Anal 2008; 14: 447-463 . [PMID: 2798037]



