Keywords
Neuroendocrine Tumors; Pancreas
INTRODUCTION
Pancreatic neuroendocrine tumors (NETs) are
relatively rare tumors in the pancreas, accounting for 1-2%
of all pancreatic tumors. These tumors are characterized
by having cells containing cytoplasmic dense-core neurosecretory
granules [1].
The incidence of this tumor was reported as 1-2 per
100000 populations; however it seems that the incidence
of PNETs is being increased over the past two to three
decades, which is partly because of better diagnostic
imaging modalities [2]. Pancreatic NETs are heterogeneous
group of neoplasms with diverse clinical findings [3].
There have not been many studies about pancreatic
NETs from Asia and Iran; also there are individualized
epidemiologic studies from the Western countries [4, 5, 6]. Herein, we will report the clinical features of pancreatic
NETs in patients operated at a single institution. In this
report we will try to clarify the clinical characteristics,
pathologic findings, and outcome of the cases with the
diagnosis of pancreatic NETs. This is because most of the previous studies have been performed in Western
countries and do not account for possible differences
between pancreatic NETs in patients from North America/
Europe and those in other countries.
PATIENTS AND MEHODS
During 5 years (2012-2016), there have been 27 cases
of pancreatic NETs which have been operated in the
affiliated hospitals of Shiraz University of Medical Sciences.
There have been 14 males and 13 female patients, with
the age range between 23 to 73 years of age (47±2.8).
Clinical charts, operation notes and pathologic findings
were retrieved and recorded. The patients were followed
up between 1 to 5 years. All of the cases have been
operated and the excised tumor has been diagnosed by
pathologic examination. The pathologic diagnosis has
been confirmed by immunohistochemical markers i.e.
synaptophysin, chromogranin and ki-67 in all of the 27
tumors.
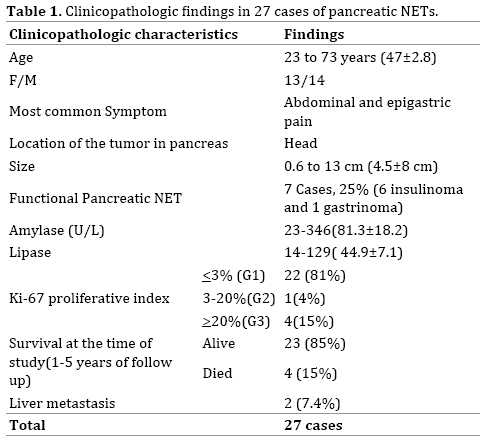
RESULTS
There have been 27 cases of pancreatic NETs during the
study period (2012-2016). The most common presenting
symptom has been abdominal and epigastric pain in 7 cases
(26%). Six cases have presented with decreased level of
consciousness and hypoglycemia (22%). Other symptoms
have been abdominal mass in 3 patients (11%), and
gastrointestinal bleeding in 2 patients (7.5%). Four cases
(15%) have incidentally been detected by imaging studies
as abdominal masses. Another 4 cases have presented with
jaundice and weight loss (15%). One of the patients has been known case of Zolinger-ellison syndrome which has
turned out to be serotonin-producing pancreatic NET.
Tumor sizes have been 0.6 to 13 cm (4.5±8 cm). The
most common location was head of the pancreas in 14
patients (52%). Ten cases were detected in the tail of
pancreas (37%). There have been 2 cases with pancreatic
NET involving body and tail and another case has shown
multiple tumors involving the whole length of the pancreas.
There have been no significant and specific paraclinical
abnormalities in the pancreatic NETs except for high insulin
levels in 6 cases (30-350 mIU/L) with the diagnosis of
insulinoma. Others had normal insulin levels below 25 mIU/L.
Gastrin level has been available only one case which
has been known case of Zolinger-ellison syndrome (250
pg/ml). Most cases (74%) showed normal amylase and
only 7 patients had high amylase levels. The amylase range
has been 23-346 U/L (81.3±18.2) with a normal range
of 23-85 U/L. All of our cases wit pancreatic NET had
normal lipase level i.e. below 160 U/L. The level of lipase
has been 14-129 U/L (44.9±7.1). All of the patients have
been operated for the excision of the pancreatic mass. Only
four cases have had preoperative tissue biopsies with the
diagnosis of NET (Table 1).
The selected procedure of surgery has been different
according to the location of the tumor in the pancreas and
the extension of the NET. Whipple’s operation has been
performed in 10 cases with the tumor in the head of pancreas (Figure 1). Simple excision has been done in the other 4
cases with the tumor located in the head of pancreas. Distal
pancreatectomy with and without splenectomy has been
performed in 10 cases with pancreatic NET in the tail of
pancreas. There have been 2 patients with pancreatic NET
metastatic to the liver, one of which has been undergone
pancreatectomy and liver transplantation and one distal
pancreatectomy and liver metastasectomy.
Figure 1: Sections from Whipple’s operation show a well-defined NET in the pancreas.
Pathologic examination and diagnosis of NET have
been confirmed by immunohistochemical positivity for
chromogranin and/or synaptophysin (Figures 2a, b,
3, 4). Proliferative index has been determined by the
number of mitosis in H&E staining and confirmed by Ki-67
immunostaining (Figure 5) [7, 8, 9, 10].
Figure 2: (a). Sections from pancreatic NET show mostly trabecular pattern with monomorphic cells and stippled chromatin with indistinct cytoplasmic border (H&EX250). (b). Sections from pancreatic NET show mostly nesting pattern (H&E X 100).
Figure 3: Sections from pancreatic NET shows positive chromogranin.
Figure 4: Sections from pancreatic NET show positive synaptophysin.
Figure 5: Sections from pancreatic NET shows Ki67 less than 3% (G1), 3-20% (G2) and more than 20% (G3).
Ki-67 has been below or equal to 3% in 22 cases (grade1
or G1) and only 5 cases had higher levels of ki-67. One case
had ki67 between 3-20% (Grade 2 or G2) and in four cases
ki-67 has been above or equal to 20% (grade 3 or G3). All
of the five G2 and G3 tumors had high mitotic activity as
well (above 10 mitosis /10 HPF).
Two patients have been known cases of ductal
carcinoma of breast. Also two cases had the preoperative
diagnosis of liver masses by imaging studies, but the
pathologic diagnosis was hemangioma.
At the end of study, twenty three patients (85%) with
pancreatic NET have been alive and free of symptoms.
Four patients have been dead, all of which had been
histologically neuroendocrine tumors with high Ki67
(above 20%).
One of the cases with liver metastasis had high Ki-67
and has been dead at the time of study. The other one with
liver metastasis who has been undergone metastasectomy
showed low Ki-67 and was alive with no symptom.
DISCUSSION
Pancreatic NETs are rare tumors with different
epidemiology and variable reported clinicopathologic
findings from all over the world. Only one study from Iran
[5] and also several individualized reports from different
Western and Asian countries (such as Japan and China)
have shown variable clinicopathologic findings [11, 12, 13, 14, 15, 16, 17, 18, 19, 20] There has been no consistent
findings from various geographic areas of the world.
In all of the previous reports, majority of the pancreatic
NETs presented with abdominal and epigastric pain,
however incidental finding of nonfunctioning small-sized
pancreatic NETs is also a common occurrence [21, 22, 23].
In both Western countries such as US [12], Sweden
[18], France [14] and Italy [17] ,and Asian countries such
as Korea [19], and Japan [21], the reported mean age have
been above 50 years (54-74), except for one study from
China with the mean age of 46 [22]. In our experience, the
mean age of pancreatic NETs was 47 years.
There have also been controversial reports about
the predominant gender which in some studies has been
more prevalent in females and in some studies has been
more common in male patients. However the difference of
female and male in all of the studies in pancreatic NET has not been significant and the female to male ratio has been
reported as 1.2/1 to 0.47/1. We had also exactly the same
experience [6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18, 19, 20].
The pathologic characteristics of the tumor has also
been the same in all of the previous studies, i.e. the mean
size has been reported from 1.5 to 4.5 cm. In our study the
mean size has been 4.5 cm as well. We had just two cases
with a size larger than 10 cm, both of which have been
histologically well differentiated and low grade (G1) and
are doing well and alive. One of them had liver metastasis at
the time of diagnosis, however despite of that, she is doing
well. This finding is compatible with previous finding have
shown that size and proliferative index are two of the main
prognostic factors in pancreatic NETs [20, 21].
In most of the previous report majority of the pancreatic
NETs (more than one third) have been detected in the
head of pancreas which is the same as our experience [11, 15]. However in some other studies the majority of the
pancreatic NETs have been in the body and tail [22].
Another important challenge in pancreatic NETs is
being functional vs. nonfunctional. In some of the previous
reports as our finding, most of the cases of pancreatic NETs
have been nonfunctioning (reported between 50-75%)
[12, 13, 14, 15]. However in some studies majority of the
pancreatic NETs have been hormone-producing, such as
report from Italy and china [17, 22] in which more than
70% of them have been functional. The most common
reported hormone has been insulin in 2-25% of cases in
the previous literature [1, 3, 15]. In our experience about
22% of the cases have been insulinoma and only one case
(4%) was gastrin-producing. The reported incidence of
gastrin-producing pancreatic NETs has been 3.1-13% [3, 11, 15].
Preoperative biopsy by endoscopic ultrasonography as
a routine procedure is a matter of controversy and there
are some reports about the increasing complication by this
modality and some studies have confirmed the changing
plan by knowing the type of pancreatic tumor before
surgery [23]. In our cases, 4 tumors have been biopsied
before excision with correct pathologic diagnosis.
Histopathologic diagnosis of pancreatic NETs is
based on the Hematoxylin and Eosin-stained sections
and confirmation by immunohistochemical staining for
chromogranin and synaptophysin. Well-differentiated
examples have characteristic nesting or organoid pattern
of cell arrangement and also trabecular, or gyriform
patterns. The nuclei show stippled chromatin and uniform
appearance with abundant neurosecretory granules,
strongly stained with neuroendocrine markers such as
chromogranin A and synaptophysin. High grade and
poorly differentiated pancreatic NETs have a more sheetlike
or diffuse pattern of cell arrangement with irregular
nuclei and less cytoplasmic granularity [7, 8].
Histologic and immunohistochemical studies in
previous reports as ours have shown that the majority of
pancreatic NETs are low grade with good prognosis and
high 5-year survival. It means that despite of the presence
of liver metastasis, a low grade pancreatic NET has a good
prognosis [7, 8, 23].
CONCLUSION
In conclusion, pancreatic Nets are heterogeneous
tumors with variable clinicopathologic characteristics. Our
findings have been very similar to other Asian countries
such as China.
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Shiba S, Morizane C, Hiraoka N, Sasaki M, Koga F, Sakamoto Y, et al. Pancreatic neuroendocrine tumors: A single-center 20-year experience with 100 patients. Pancreatology 2016;16:99-105. [PMID: 26718527]
- Estrozi B, Bacchi CE. Neuroendocrine tumors involving the gastroenteropancreatic tract: a clinicopathological evaluation of 773 cases. Clinics (Sao Paulo) 2011; 66:1671-1675. [PMID: 22012036]
- Han X, Xu X, Jin D, WangD, Ji Y, Lou W. Clinicopathological Characteristics and Prognosis-Related Factors of Resectable Pancreatic Neuroendocrine Tumors. A Retrospective Study of 104 Cases in a Single Chinese Center. Pancreas 2014;43:526-531. [PMID: 24658317]
- Nozari N, Nikfam S, Nikmanesh A, Mohammadnejad M, Sotoudehmanesh R, Zamani F, et al. Clinical and Pathological Features of Non-Functional Neuroendocrine Tumors of Pancreas: A Report from Iran. Middle East J Dig Dis 2014; 6:151-154. [PMID: 25093063]
- Haghighi S, Molaei M, Foroughi F, Foroutan M, Dabiri R, Habibi E, et al. Role of Endoscopic Ultrasound in Evaluation of Pancreatic Neuroendocrine Tumors - Report of 22 Cases from a Tertiary Center in Iran. Asian Pacific J Cancer Prev 2012; 13:4537-4540. [PMID: 23167375]
- Sotoudemanesh R, Hedayat A, Shirazian N, Shahraeeni S, Ainechi S, Zeinali F, et al. Endoscopic ultrasonography (EUS) in the localization of insulinoma. Endocr 2007; 31:238–241. [PMID: 17906369]
- Klimstra DS, Modlin IR, Coppola D,Lloyd RV, Suster S. The Pathologic Classification of Neuroendocrine Tumors. A review of Nomenclature, Grading and Staging Systems. Pancreas 2010;39:707-712. [PMID: 20664470]
- Ehehalt F, Saeger HD, Schmidt M, Grutzmann R. Neuroendocrine tumors of the pancreas. Oncologist 2009;14:456–467. [PMID: 19411317]
- Kim JY, Hong SM, Ro JY. Recent updates on grading and classification of neuroendocrine tumors. Ann Diagn Pathol 2017; 29:11–16. [PMID: 28807335]
- Ito T, Sasano H, Tanaka M, Osamura RY, Sasaki I, Kimura W, et al. Epidemiological study of gastroenteropancreatic neuroendocrine tumors in Japan. J Gastroenterol 2010; 45:234–243. [PMID: 20058030]
- Bilimoria KY, Tomlinson JS, Merkow RP, Stewart AK, Ko CY, Talamonti MS, et al. Clinicopathologic Features and Treatment Trends of Pancreatic Neuroendocrine Tumors: Analysis of 9,821 Patients. J Gastrointest Surg 2007;11:1460–1469. [PMID: 17846854]
- Dahdaleh FS, Calva-Cerquira D, Carr JC, Liao J,Mezhir JJ, O’Dorisio TM, et al. Comparison of Clinicopathologic Factors in 122 Patients with Resected Pancreatic and Ileal Neuroendocrine Tumors from a Single Institution. Ann Surg Oncol 2012; 19:966–972. [PMID: 21845496]
- Halfdanarson TR, Rubin J, Farnell MB, Grant CS, Petersen GM. Pancreatic endocrine neoplasms: epidemiology and prognosis of pancreatic endocrine tumors. Endocr Relat Cancer 2008; 15:409–427. [PMID: 18508996]
- Figueiredo FA, Giovannini M, Monges G, Charfi S, Bories E, Pesenti C, et al. Pancreatic Endocrine Tumors A Large Single-Center Experience. Pancreas 2009;38:936-940. [PMID: 19672207]
- Ekeblad S, Skogseid B, Dunder K, Berg K, Eriksson B. Prognostic Factors and Survival in 324 Patients with Pancreatic Endocrine Tumor Treated at a Single Institution. Clin Cancer Res 2008;14: 7798-7803. [PMID: 19047107]
- Geramizadeh B, Kashkooe A, Malkehosseini A. Liver Metastasis of Gastrointestinal Neuroendocrine Tumors: A Single Center Experience. Hepat Mon 2016; 16:e37293. [PMID: 27330538]
- Zerbi A, Falconi M, Rindi G, Fave GD, Tomassetti P, Pasquali C, et al. Clinicopathological Features of Pancreatic Endocrine Tumors: A Prospective Multicenter Study in Italy of 297 Sporadic Cases. Am J Gastroenterol 2010; 105:1421–1429. [PMID: 20087335]
- Jiao X, Li Y, Wang H, Liu S, Zhang D, Zhou Y. Clinicopathological features and survival analysis of gastroenteropancreatic neuroendocrine neoplasms: a retrospective study in a single center of China. Chin J Cancer Res 2015;27:258-266. [PMID: 26157322]
- Shin Y, Ha SY, Hyeon J, Lee B, Lee KT, Jang KT, et al. Gastroenteropancreatic Neuroendocrine Tumors with Liver Metastases in Korea: A Clinicopathological Analysis of 72 Cases in a Single Institute. Cancer Res Treat 2015;47:738-746. [PMID: 25687852]
- Hauso O, Gustafsson BI, Kidd M, Waldum HL, Waldum HL, Drozdov I, et al. Neuroendocrine Tumor Epidemiology. Contrasting Norway and North America. Cancer 2008;113:2655-2668. [PMID: 18853416]
- Yamamoto Y, Okamura Y, Uemura S, Sugiura T, Ito T, Ashida R, et al. Vascularity and Tumor Size are Significant Predictors for Recurrence after Resection of a Pancreatic Neuroendocrine Tumor. Ann Surg Oncol 2017; 24:2363–2370. [PMID: 28271173]
- Yang M, Zeng L, Zhang Y, Wang WG, Wang L, Ke NW. TNM Staging of Pancreatic Neuroendocrine Tumors. An Observational Analysis and Comparison by Both AJCC and ENETS Systems from 1 Single Institution. Medicine 94;12:e660. [PMID: 25816036]
- Bar-Moshe Y, Mazeh H, Gozinsky-Glasberg S. Non-functioning pancreatic neuroendocrine tumors:Surgery or observation?World J GastrointestEndosc 2017;9:149-203. [PMID: 28465781]






