Keywords
Nomograms; Pancreatic Neoplasms
INTRODUCTION
An estimated 337,800 people were diagnosed with
pancreatic cancer around the world in 2012; more than
330,000 patients succumbed due to this disease [1].
Furthermore, the incidence of pancreatic cancer tends to
increase. The disease is expected to take second place in
cancer mortality in the United States by 2030 [2].
FOLFIRINOX, gemcitabine in combination with nabpaclitaxel
or gemcitabine monotherapy are current
frontline regimens for the treatment of locally advanced
and metastatic pancreatic cancer [3, 4]. On the contrary
second-line chemotherapy regimens for this disease are
not standardized. Most patients do not receive secondline
chemotherapy, mainly due to the rapid deterioration
of performance status following cancer progression [5, 6].
Other relevant clinical factors, such as efficacy of previous
chemotherapy, lesions sites and sizes, weight loss and
laboratory parameters, are usually not taken into account.
All current second-line regimens have modest efficacy:
objective response rate is usually below 10% [7], median
progression-free survival is approximately 2 months [5]. Therefore patients should be carefully selected for
chemotherapy and there is an unmet medical need for a
predictive model which would facilitate patient selection
for second-line chemotherapy.
MATERIAL AND METHODS
Patients
Records of patients with pancreatic cancer who had
been treated at the department of clinical pharmacology
and chemotherapy of N.N. Blokhin Russian Cancer
Research Center since 2000 to 2015 were analyzed.
Eligibility criteria for this retrospective analysis were: 1)
morphologically confirmed locally advanced/metastatic or
recurrent pancreatic cancer, 2) disease progression within
6 months after the last cycle of first-line chemotherapy or
adjuvant chemotherapy.
Patient’s clinical and laboratory characteristics at the
time of progression after previous chemotherapy were
evaluated for prognostic and predictive significance. The
following clinical and laboratory factors were analyzed:
gender, age, family history/ supposed hereditary cancer
(yes vs. no), smoking status (current or former smokers vs. never smokers), body mass index, percentage of body
weight loss over the periodduring the course of the
disease, diabetes mellitus (yes vs. no), metformin , aspirin
or statins intake (yes vs. no), Karnofsky performance status
(100-80% vs. 70% vs. ≤60%), previous chemotherapy
setting (adjuvant vs. neoadjuvant ± adjuvant vs. first-line),
previous chemotherapy regimen (containing gemcitabine vs. not contain gemcitabine), objective response to previous
chemotherapy (yes vs. no), time to progression following
previous chemotherapy, site of the primary tumor (head vs. body or tail of the pancreas), maximum primary tumor
size, presence of regional lymph nodes involvement (yes vs.
no), presence (yes vs. no) and maximum size of metastases
in retroperitoneal lymph nodes, liver, lung, peritoneum,
presence of ascites (yes vs. no), tumor grade (G1 vs. G2 vs. G3), CEA and CA19-9 levels, albumin level (normal vs. below lower limit of normal), total bilirubin level
(normal vs. above upper limit of normal [ULN]), alkaline
phosphatase level, levels of hemoglobin, white blood cells,
platelets and neutrophil-to-lymphocyte ratio (NLR).
STATISTICAL ANALYSIS
Prognostic value of the all above mentioned factors
has been assessed by univariate Cox proportional hazards
model with overall survival (OS) as the endpoint. OS was
calculated from date of progression following previous
chemotherapy to death or last contact with a patient for
censored cases. Kaplan-Meier method was used to assess
OS. Cutoff levels of quantitative factors were chosen using
the ROC-curves analysis. Three months survival rate was
selected as the endpoint for ROC-curve analysis.
Factors, that demonstrated a statistically significant
impact on OS according to the results of univariate analyses,
were further analyzed in the multivariate Cox proportional
hazards model with stepwise exclusion of variables.
Factors that showed statistically significant impact on
OS were considered independent prognostic factors. The
prognostic model was constructed based on these factors
dichotomizing patients into groups with poor or favorable
prognosis. Hazard ratios for each independent prognostic factor were taken into consideration for prognostic score
calculation. Then an impact of second-line chemotherapy
on overall survival was evaluated with stratification into
two prognostic groups.
Statistical analysis of the data was conducted using
Microsoft Excel 2007 and IBM SPSS Statistics v. 20.
RESULTS
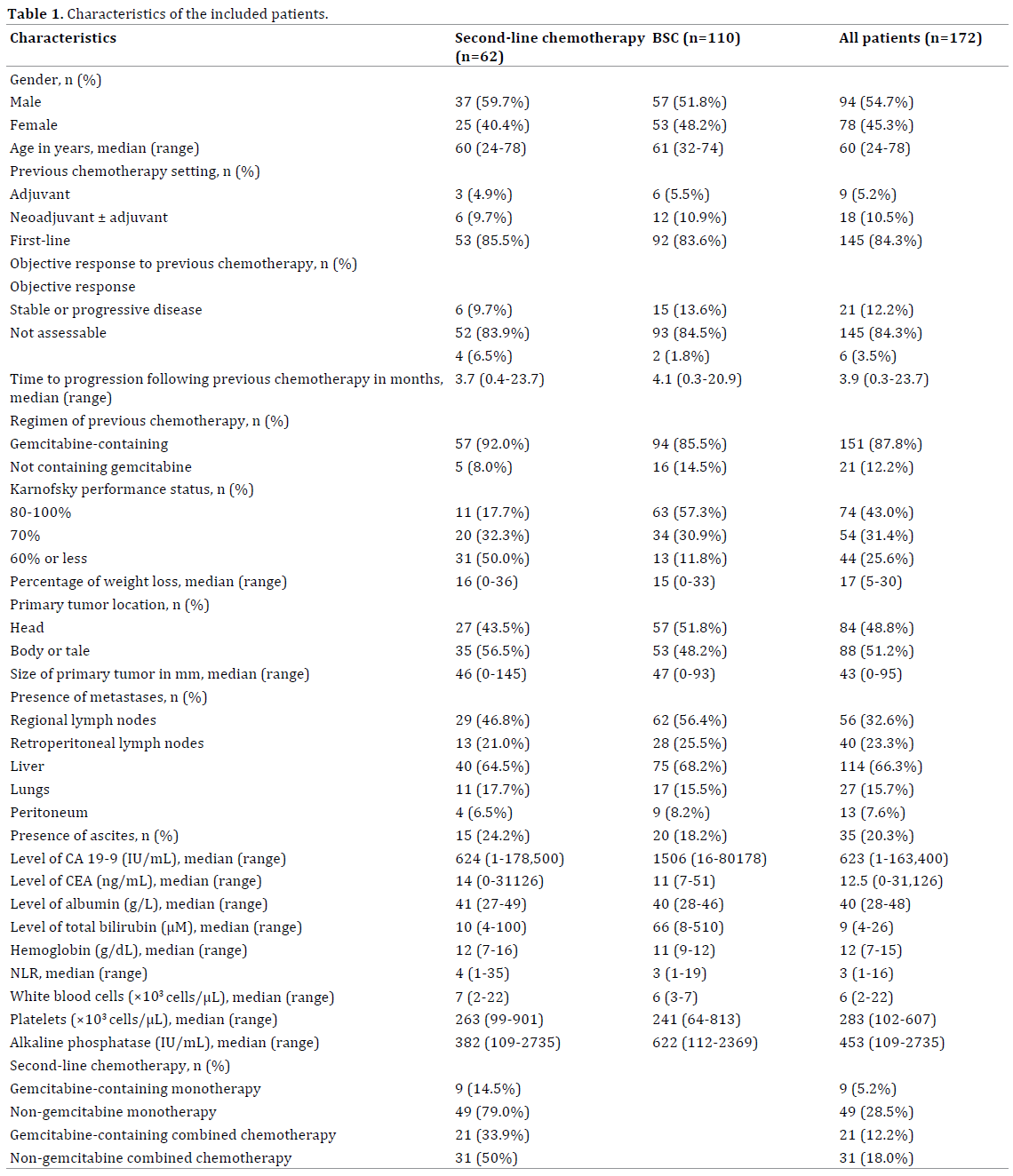
Patients Characteristics
A total of 347 patients received primary chemotherapy.
Of them 172 patients met the inclusion criteria for the
present analysis (Figure 1). Median OS in the whole cohort
of patients was 3.4 months (95% confidential interval (CI)
2.8-4.0 months). Characteristics of included patients are
presented in Table 1.
Figure 1. Patients flow chart.
Factors of Unfavorable Prognosis
Univariate Cox regression analyses showed that the
following variables had negative impact on OS: presence
of liver metastases greater than 20 mm in maximum
dimension [hazard ratio (HR) 1.513, 95% CI 1.090-2.101],
presence of ascites [HR 1.941, 95% CI 1.303-2.890],
Karnofsky performance status ≤70% [HR 1.818, 95%
CI 1.502-2.201], albumin level <35 g/L [HR 1.766, 95%
CI 1.069-2.917], total bilirubin >ULN [HR 1.656, 95% CI
1.122-2.445], hemoglobin ≤11 g/dL [HR 1.404, 95% CI
1.002-1.965], NLR> 5 [HR 1.845, 95% CI 1.236-2.755]
and alkaline phosphatase > 5 times higher ULN value [HR
2.424, 95% CI 1.374-4.277].
These factors were further analyzed in the multivariate
Cox regression analysis with stepwise variable exclusion.
Multivariate analysis results are presented in Table 2.

Two factors - Karnofsky status 70% or less and
NLR>5 – were shown to be independent poor prognostic
factors in pancreatic cancer progressing after first-line
chemotherapy. Groups of favorable (score 0-1) and poor
prognosis (score ≥2) were formed based on HR values of
these two factors.
Figure 2 shows Kaplan-Meier curves for OS in these
two risk groups. Median OS were 5.0 and 1.8 months
for groups of favorable and poor prognosis, respectively
(p<0.001).
Figure 2. Overall survival of patients with favorable (n=113) and poor (n=59) prognosis.
Efficacy of Second-line Chemotherapy
OS in patients who received second-line chemotherapy
or BSC only was compared with stratification by prognostic
groups (Figures 3 a,b). Median OS in the favorable
prognosis groups was 5.5 and 1.7 months for patients who
received chemotherapy and BSC only, respectively (HR
2.119, 95% CI 1.302-3.448, p=0.002). Median OS in the
poor prognosis group was 2.3 and 1.7 months for patients
who received chemotherapy and BSC only, respectively
(HR 1.392, 95% CI 0.798-2.428, p=0.233).
Figure 3. Overall survival of patients with pancreatic cancer who received second-line chemotherapy or only best supportive care stratified by prognostic
groups; a - cohort of patients with favorable prognosis, b - cohort of patients with poor prognosis.
DISCUSSION
Efficacy of second-line chemotherapy is usually
low in most patients with pancreatic cancer. However,
there are limited data suggesting that selected patients
receiving second-line chemotherapy can benefit from its
administration compared to BSC.
A small randomized trial comparing efficacy of OFF
regimen (oxaliplatin / folinic acid / 5-fluorouracil)
versus BSC in patients who had tumor progression
following gemcitabine-containing front line chemotherapy
demonstrated increased median OS in the OFF group [8].
A systematic analysis of published trials of secondline
chemotherapy in pancreatic cancer demonstrated a
consistent increase in the proportion of patients receiving
second-line chemotherapy during the recent years.
The authors found that the increase in the second-line
chemotherapy utilization had a positive impact on OS [5].
Less than half of the patients receive second-line
chemotherapy, mostly due to a rapid deterioration of
general condition [9, 10]. Good performance status is a
major factor supporting the decision to start second-line
chemotherapy [11].
There are few studies evaluating the prognostic role
of clinical and laboratory factors other than performance
status in pancreatic cancer progressing after first-line
chemotherapy. Nakachi K et al. evaluated the impact of
several clinical and laboratory factors on OS of 74 patients
with pancreatic cancer progression following gemcitabinecontaining
chemotherapy. The multivariate Cox proportional
hazards model showed that three factors - C-reactive protein
≥5 mg/dL, ECOG status ≥2 and presence of peritoneal
metastases were independent poor prognostic factors [12].
Marechal et al. demonstrated that CA19-9 level ≥400 IU/
mL and albumin ≤3.5 mg/dL were independent negative
prognostic factors for OS [13]. Herrmann et al. showed that
time to progression on first-line chemotherapy correlated
with OS of patients on second-line chemotherapy [14].
Kim ST et al. showed that ECOG status ≥2, lack of response
to first-line chemotherapy and albumin level <3.5 mg/dL
were independent factors of poor prognosis [15].
Limitations of the most above mentioned studies were
small number of patients and patient selection bias. Only
those patients who received second-line chemotherapy
were included so it is impossible to evaluate whether
identified prognostic factors can also be predictors of
second-line chemotherapy failure.
In the recent retrospective study authors evaluated
an impact of 50 clinical factors on OS of pancreatic
cancer patients who received first-line chemotherapy in
Besancon hospital in France. Elderly age, smoking, liver
metastases, poor performance status, pain, jaundice,
ascites and short duration of gemcitabine-based first-line
chemotherapy were found to be independent negative
prognostic factors [16]. Based on these prognostic factors
patients were divided into three groups. However, secondline
chemotherapy improved OS in each of these groups
although the HR in the high risk group was lower than in
the low risk group [16]. Uncertain correlation between
death risk and chemotherapy benefit limits the use of such
a model for prediction of chemotherapy benefit.
The present analysis is consistent with previous reports
demonstrating that patient performance status estimated
by Karnofsky scale as 70% or below is an independent
factor of poor prognosis. Another independent factor of
poor prognosis is NLR> 5. NLR is a marker of inflammation.
A number of studies demonstrated significant influence
of inflammation on tumor progression, invasion and
metastasis [17-19]. A metaanalysis of nine studies with
2035 participants demonstrated prognostic value of NLR
in primary pancreatic cancer [20]. Cut-off values of NLR
varied from 2 to 5 in these nine studies.
Results of the present analysis support the prognostic
significance of NLR in patients with disease progression
following first-line chemotherapy. These findings are
consistent with reported by Nakachi K et al. who demonstrated
an independent prognostic value of another inflammation
marker, C-reactive protein, in patients with progression after
gemcitabine-containing chemotherapy [12].
Patients treated with second-line chemotherapy and
patients who received BSC only were included in the
present analysis (Table 1). The presence of the latter
group allowed us to analyze the impact of chemotherapy
on OS with stratification into two prognostic
groups and compare it to OS of patients received no
chemotherapy.
Our results have shown that second-line chemotherapy
can improve outcomes only in the favorable prognostic
group of patients. In the poor prognosis group secondline
chemotherapy failed to demonstrate a statistically
significant impact on the outcome.
It should be noted that due to limited number of
patients the benefit of second-line therapy cannot be
excluded in the poor prognostic group. However, this
minimal benefit can be easily ruined by the toxicity of
the treatment. Thus, despite the fact that second-line
chemotherapy improves OS compared to BSC, it seems
rationale to limit the use of second-line chemotherapy
to selected patients.
CONCLUSION
New prognostic model for pancreatic cancer patients
with progression following first-line chemotherapy
has been developed. Retrospective nature and a small
number of patients should be considered as limitation
of this analysis. Advantages of this model are the use
of widespread parameters, available in routine clinical
practiceand its ability to serve as a predictive model of
second-line chemotherapy failure.
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- IARC: Section of Cancer Surveillance (CANCERMondial). https://
www-dep.iarc.fr
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM,
Matrisian LM. Projecting cancer incidence and deaths to 2030: the
unexpected burden of thyroid, liver, and pancreas cancers in the United
States. Cancer Res 2014; 74:2913-2921. [PMID: 24840647]
- Khorana AA, Mangu PB, Berlin J, Engebretson A, Hong TS, Maitra
A, et al. Potentially curable pancreatic cancer: American society
of clinical oncology clinical practice guideline. J Clin Oncol 2017;
11:JCO2017724948. [PMID: 28398845]
- Ducreux M, Cuhna AS, Caramella C, Hollebecque A, Burtin P, Goéré
D, et al. Cancer of the pancreas: ESMO clinical practice guidelines for
diagnosis, treatment and follow-up. Ann Oncol 2015; 26(Supplement 5):
v56–v68. [PMID: 26314780]
- Nagrial AM, Chin VT, Sjoquist KM, Pajic M, Horvath LG, Biankin AV, et al. Second-line treatment in inoperable pancreatic adenocarcinoma:
A systematic review and synthesis of all clinical trials. Crit Rev Oncol
Hematol 2015; 96:483-497. [PMID: 26481952]
- Sohal DP, Mangu PB, Khorana AA, Shah MA, Philip PA, O'Reilly EM, et al. Metastatic pancreatic cancer: American society of clinical oncology
clinical practice guideline. J Clin Oncol 2016; 34:2784-96. [PMID:
27247222]
- Onesti C, Romiti A, Roberto M, Falcone R, Marchetti P. Recent
advances for the treatment of pancreatic and biliary tract cancer after
first -line treatment failure. Expert Rev Anticancer Ther 2015; 15:1183-
1198. [PMID: 26325474]
- Oettle H, Pelzer U, Stieler J, Hilbig A, Roll L, Schwaner I, et al. Oxaliplatin/
folinic acid/5-fluorouracil [24h] (OFF) plus best supportive care versus best
supportive care alone (BSC) in second-line therapy of gemcitabine-refractory
advanced pancreatic cancer (CONKO 003). J Clin Oncol 2005; 23:4031.
- Conroy T, Desseigne F, Ychou M, Bouché O, Guimbaud R, Bécouarn Y, et al. FOLFIRINOX versus gemcitabine for metastatic pancreatic cancer. N
Engl J Med 2011; 364:1817-25. [PMID: 21561347]
- Von Hoff DD, Ervin T, Arena FP, Chiorean EG, Infante J, Moore M, et al. Increased survival in pancreatic cancer with nab-paclitaxel plus
gemcitabine. N Engl J Med 2013; 369:1691-703. [PMID: 24131140]
- Sohal DP, Mangu PB, Khorana AA, Shah MA, Philip PA, O'Reilly EM, et al.
Metastatic pancreatic cancer: American society of clinical oncology clinical
practice guideline. J Clin Oncol 2016; 34:2784-96. [PMID: 27247222]
- Nakachi K, Furuse J, Ishii H, Suzuki E, Yoshino M. Prognostic factors in
patients with gemcitabine-refractory pancreatic cancer. Jpn J Clin Oncol
2007; 37:114-120. [PMID: 17272317]
- Maréchal R, Demols A, Gay F, De Maertelaere V, Arvanitaki M,
Hendlisz A, et al. Prognostic factors and prognostic index for chemonaive
and gemcitabine-refractory patients with advanced pancreatic cancer.
Oncology 2007; 73:41e51. [PMID: 18334830]
- Herrmann C, Abel U, StremmelW, Jaeger D, Herrmann T. Short time
to progression under first-line chemotherapy is a negative prognostic
factor for time to progression and residual survival under secondline
chemotherapy in advanced pancreatic cancer. Oncology 2007; 73:
335e339. [PMID: 18497506]
- Kim ST, Choi YJ, Park KH, Oh SC, Seo JH, Shin SW, et al. A prognostic
model to identify patients with advanced pancreas adenocarcinoma who
could benefit from second-line chemotherapy. Clin Oncol (R Coll Radiol)
2012; 24:105-11. [PMID: 21382702]
- Vienot A, Beinse G, Louvet C, de Mestier L, Meurisse A, Fein F, et al.
Development and validation of a prognostic nomogram and score to
predict overall survival and usefulness of second-line chemotherapy
in advanced pancreatic adenocarcinoma. J Clin Oncol 2017. [PMID:
28383673]
- Balkwill F, Mantovani A. Inflammation and cancer: back to Virchow?
Lancet 2001; 357:539-45. [PMID: 11229684]
- Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related
inflammation. Nature 2008; 454:436-444. [PMID: 18650914]
- Grivennikov SI, Greten FR, Karin M. Immunity, inflammation, and
cancer. Cell 2010; 140:883-899. [PMID: 20303878]
- Cheng H, Long F, Jaiswar M, Yang L, Wang C, Zhou Z. Prognostic role of
the neutrophilto-lymphocyte ratio in pancreatic cancer: a meta-analysis.
Sci Rep 2015; 5:11026. [PMID: 26226887]




