INTRODUCTION
The human pancreas develops embryologically from the fusion of the ventral and dorsal buds. Under normal conditions, the superior branch of the ventral pancreatic duct fuses with the dorsal pancreatic duct and participates in the formation of the main pancreatic duct [1, 2]. In the embryo, the accessory pancreatic duct is the main drainage duct of the dorsal pancreas and enters the duodenum at the minor duodenal papilla. As development progresses, the duct of the dorsal bud undergoes varying degrees of atrophy at the duodenal end, finally forming the adult configuration of the duct [1, 2, 3].
Pancreas divisum (PD) is a common congenital anomaly of the pancreas, which results from an abnormal fusion between the ventral and dorsal pancreatic ducts during fetal development. It is divided into complete and incomplete PD. Complete PD is defined as a common separate pancreatic duct system. Incomplete PD is an anatomic variation that has an inadequate communication, usually an extremely small branch, between the ventral and dorsal pancreatic ducts [4, 5]. In Japan, an embryological and radiological concept of branch fusion between the ventral and dorsal pancreatic ducts was proposed [6].
In complete PD, the dorsal pancreatic duct leaves as the principal conduit of exocrine secretion from the pancreas and enters into the duodenum through the minor duodenal papilla. It has been suggested that complete PD may cause acute pancreatitis, chronic pancreatitis, or pancreatic-type pain [4, 7], but the clinical implications of incomplete PD have not yet been well established. We investigated the clinical significance of incomplete PD compared to complete PD.
Methods
Patients
During the past 23 years, we have documented the anatomy of the pancreatic duct system in 3,210 cases using endoscopic retrograde pancreatography via the minor duodenal papilla, as well as the major duodenal papilla. To achieve optimal visualization, several pancreatograms of the head of the pancreas were taken in prone or slightly oblique position.
Complete PD was diagnosed when, on cannulation of the minor duodenal papilla, the entire dorsal pancreatic duct from the tail to the anterior part of the head was filled with medium, and there was no communication with the ventral pancreatic duct. Incomplete PD was diagnosed when the ventral and dorsal pancreatic ducts ran parallel to each other, and there was an inadequate communication between them, usually consisting of an extremely small branch or a branch from the dorsal pancreatic duct that ran towards the ventral pancreatic duct in a roundabout manner.
Clinical Analysis
The clinical data of all cases were gathered by chart review. Patients with complete PD were compared with patients with incomplete PD with respect to history of alcohol abuse and presence of pancreatic diseases (acute or chronic pancreatitis, and pancreatic-type pain). The diagnosis of acute pancreatitis was based on episodes of abdominal pain accompanied by serum amylase or lipase levels that were twice the normal level, typical changes on ultrasonography or computed tomography (CT), and the absence of ductal changes characteristic of chronic pancreatitis. The diagnosis of chronic pancreatitis was based on either the existence of pancreatic stones visible on plain films of the abdomen or CT, or characteristic ductal changes on endoscopic retrograde cholangiopancreatography (ERCP) [8]. The clear-cut symptomatology of pancreatic-type pain is difficult to define. However, pancreatic-type pain usually presents as pain that is localized to the epigastrium, the left hypogastrium, or the right hypogastrium, often radiating directly to the back, which is alleviated by bending forward [9]. Pancreatic-like disease was defined by pooling together patients having pancreatitis and/or pancreatic-like pain. A history of alcohol abuse was diagnosed when alcohol intake exceeded 80 g/day for at least 10 years. The prevalence of chronic and acute pancreatitis associated with complete or incomplete PD was compared with that of cases with neither complete nor incomplete PD (controls).
ETHICS
This is a retrospective study and data were collected in the usual clinical practice.
STATISTICS
Means, ranges, and frequencies are reported as descriptive statistics. Data were statistically compared with those in controls using the Fisher’s exact and the Mann-Whitney U-test tests. Two-tailed P values less than 0.05 were considered statistically significant. The StatView software was used for data analysis.
RESULTS
In the 3,220 cases that had successful pancreatography (1,703 men and 1,517 women; mean age, 59.7 years, range 17-96), complete PD was identified in 44 patients (1.4%; 22 men and 22 women; mean age, 58.4 years, range 22-85 years). Via the major duodenal papilla, a short ventral pancreatic duct was detected in 32 patients (72.7%), and small ventral pancreas acinarization was detected in three patients (6.8%). Magnetic resonance cholangiopancreatography (MRCP) was performed in 15 patients, and dorsal and ventral pancreatography of the autopsied pancreas was performed in three patients. Incomplete PD was diagnosed in 41 patients (1.3%; 21 men and 20 women; mean age, 59.3 years, range 26-83 years). Incomplete PD was diagnosed by cannulating the major duodenal papilla in 29 patients, and by cannulating both the major duodenal papilla and the minor duodenal papilla in 12 patients. No significant difference in sex (P=0.741) and age (P=0.327) was observed between the 3,135 cases without complete or incomplete PD and the 85 patients with PD. In the 3,135 cases without complete or incomplete PD ERCP was done due to clinical suspicion of biliary diseases (n=1,421, 45.3%), pancreatic diseases (n=764, 24.4%: acute pancreatitis, n=181, 5.8%; chronic pancreatitis, n=161, 5.1%; pancreatic carcinoma, n=255, 8.1%; intraductal papillary mucinous neoplasm, n=89, 2.8%; pancreatic cyst, n=78, 2.5%), or other diseases (n=950, 30.3%). ERCP was done more frequently due to clinical suspicion of pancreatic diseases in patients with complete (n=26, 59.1%) than in incomplete (n=21, 51.2%) PD but the difference was not statistically significant (P=0.517).
Chronic pancreatitis occurred more frequently in patients with complete PD (25.0%: 11/44) and patients with incomplete PD (19.5%: 8/41) than in controls (4.5%: 142/3,135) (P<0.001 and P=0.001, respectively). Acute pancreatitis occurred more frequently in patients with complete PD (15.9%: 7/44) than in controls (5.5%: 171/3,135) (P=0.010). However, the prevalence of acute pancreatitis in patients with incomplete PD (7.3%, 3/41) was not significantly different from controls (Table 1).

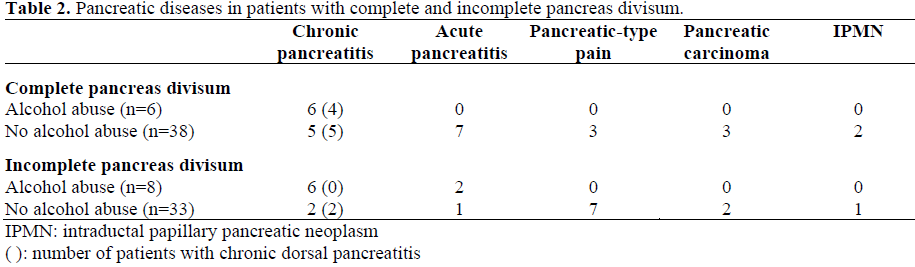
Of the 44 patients with complete PD, the six patients who abused alcohol had chronic pancreatitis: in two patients, the chronic pancreatitis involved the entire organ with pathological changes in both the ventral and dorsal pancreatic ducts; the other four patients had chronic dorsal pancreatitis with pathological changes seen only in the dorsal pancreatic duct (isolated chronic dorsal pancreatitis). Of the remaining 38 patients who did not abuse alcohol, five had chronic dorsal pancreatitis; seven had acute pancreatitis, including acute relapsing pancreatitis (n=2); three had pancreatic-type pain; three had pancreatic carcinoma in the dorsal pancreas; and two had intraductal papillary mucinous neoplasm in the dorsal pancreas. Complete PD was suspected as the cause of associated pancreatitis-like disease, including pancreatic-type pain, in 15 (39.5%) of these 38 patients.
In the eight patients with incomplete PD who abused alcohol, six patients had chronic pancreatitis of the entire organ and two had acute relapsing pancreatitis. Of the remaining 33 incomplete PD patients who did not abuse alcohol, two had chronic dorsal pancreatitis; one had acute relapsing pancreatitis; seven had pancreatic-type pain; two had pancreatic carcinoma in the dorsal pancreas; and one had intraductal papillary mucinous neoplasm in the dorsal pancreas. Incomplete PD was suspected as the cause of associated pancreatitis-like disease in 10 (30.3%) of these 33 patients (Table 2).
DISCUSSION
Pancreas divisum is a common congenital pancreatic ductal anomaly variant. It has a reported prevalence of 5-6% in ERCP series [10, 11] and 9.3-10.8% in MRCP series [12, 13]. However, the condition reportedly occurs less frequently in Japan (about 1%). Incomplete PD is uncommon, with a reported prevalence of 0.13-0.9% [14, 15] in Western series. However, in the present study, 41 (48%) of the 85 PD cases had incomplete PD, which was similar to the 52% reported from Korea [16]. Incomplete PD in Western countries may be underestimated partly due to under-reporting or failure to identify the anatomical abnormality.
In patients with complete PD, the dorsal pancreatic duct becomes the main pancreatic duct and drains most of the pancreas through the minor duodenal papilla. As the minor duodenal papilla is substantially smaller than the major duodenal papilla, a larger volume of secretions could place a significant load on the minor duodenal papilla [3, 4]. Most cases with complete PD may be asymptomatic, and the relationship between complete PD and pancreatitis is contentious. However, it has been suggested that, in some cases, complete PD may cause acute pancreatitis, chronic pancreatitis, or pancreatic-type pain, due to the presence of relative obstruction to the drainage of pancreatic juices at the minor duodenal papilla [4, 7]. Although a relationship between abnormalities of the cystic fibrosis gene product and recurrent acute pancreatitis in patients with PD was recently reported [17], further studies have not yet been done. Incomplete PD is a pancreatic anomaly in which there is an inadequate communication between the ventral and dorsal pancreatic ducts; often the two ducts communicate through an extremely small branch. However, the clinical significance of incomplete PD has not yet been well established.
In the present study, all of the patients with complete or incomplete PD who abused alcohol had chronic or acute pancreatitis. Of the patients with complete PD, four patients who abused alcohol and five patients who did not abuse alcohol had irregular dilatation of the entire dorsal pancreatic duct alone (isolated chronic dorsal pancreatitis). It is not completely clear how PD causes pancreatitis in some alcoholic patients; it could be that, in patients with complete PD, an interaction between a poorly functioning minor duodenal papilla and the increased flow of pancreatic juice caused by alcohol or food intake could increase dorsal duct pressure and lead to pathology confined to the dorsal pancreatic duct. The six patients with incomplete PD who abused alcohol had pathological changes in both the ventral and dorsal pancreatic ducts, but in four patients, the changes in the dorsal pancreatic duct were more severe than those in the ventral pancreatic duct. As well, chronic pancreatitis occurred more frequently in patients with complete PD and incomplete PD than in controls. The prevalence of pancreatitis-like disease, including pancreatictype pain, associated with complete and incomplete PD was similar.
Although we have not yet endoscopically treated PD patients, two reports have been published dealing with endoscopic treatment of patients with incomplete PD. In the Jacob’s paper [18], 18 (56%) of 32 patients with incomplete PD had clinical manifestations related to the anomaly and underwent endoscopic treatment, including minor duodenal papilla sphincterotomy or dorsal duct stent placement, to improve the flow rate at the minor duodenal papilla and decompress the dorsal pancreatic duct. Six (60%) of 10 patients with acute recurrent pancreatitis and four (80%) of five patients with chronic pancreatitis improved after endoscopic therapy. Kim et al. [16] reported that in 12 (44%) of 27 patients with complete PD and in 14 (48%) of 29 patients with incomplete PD, it was suspected that the anomaly was causing pancreatic diseases; after endoscopic treatment, clinical improvement was seen in seven (70%) of 10 symptomatic patients with complete PD and in eight (62%) of 13 symptomatic patients with incomplete PD. In many cases of incomplete PD, the communication between the ventral and dorsal pancreatic ducts is circular or involves a filamentous branch; therefore, drainage of most of the pancreatic juice in the dorsal pancreatic duct may occur via the minor duodenal papilla. Thus, some cases of incomplete PD have a dorsal pancreatic ductdominant physiological status that is similar to that in patients with complete PD, which sometimes induces functional overflow obstruction and complications can develop. However, although acute pancreatitis occurred more frequently in patients with complete PD than in controls, the prevalence of acute pancreatitis in patients with incomplete PD was not different from that in controls. Given this fact, the precise pathophysiology of incomplete PD may be different from that of complete PD.
An association between PD and pancreatic tumors has been reported by some researchers [19, 20]; seven (5%) of 137 patients with PD were found to have pancreatic tumors [8]. Since most pancreatic tumors in association with PD developed in the dorsal pancreas, it is possible that long-standing dorsal duct obstruction caused by the relative stenosis of the minor duodenal papilla might be a factor that promotes pancreatic carcinoma [19, 20]. It is also interesting to note that all three pancreatic tumors in patients with incomplete PD in our series developed in the dorsal pancreas.
In conclusion, although the precise pathophysiology may differ, patients with complete PD and patients with incomplete PD may have similar presentations and a similar prevalence. Thus, the clinical implications of incomplete PD may be similar to those of complete PD.
References
- Adda G, Hannoun L, Loygue J. Development of the human pancreas: variations and pathology. A tentative classification. Anat Clin 1984; 5:275-83. [PMID 6372837]
- Kamisawa T, Koike M, Okamoto A. Embryology of the pancreatic duct system. Digestion 1999; 60:161- 5. [PMID 10095158]
- Kamisawa T, Tabata I, Tajima T, Tsushima K, Yoshida Y. Patency of the human accessory pancreatic duct determined by dye-injection endoscopic retrograde pancreatography. Digestion 1997; 58:78-82. [PMID 9018014]
- Kamisawa T. Clinical significance of the minor duodenal papilla and accessory pancreatic duct. J Gastroenterol 2004; 39:605-15. [PMID 15293129]
- Warshaw AL, Simeone JF, Schapiro RH, Flavin- Warshaw B. Evaluation and treatment of the dorsal duct syndrome (pancreas divisum redefined). Am J Surg 1990; 159:59-66. [PMID 2403764]
- Hirooka T, Kataoka S, Ohchi H, Maruo T, Toyonaga T, Dozaiku T, et al. Branch fusion between the ventral and dorsal pancreatic duct. Dig Endosc 1994; 6:87-93.
- Lehman GA, Sherman S, Nisi R, Hawes RH. Pancreas divisum: results of minor papilla sphincterotomy. Gastrointest Endosc 1993; 39:1-8. [PMID 8454127]
- Bernard JP, Sahel J, Giovannini M, Sahels H. Pancreas divisum is a probable cause of acute pancreatitis: a report of 137 cases. Pancreas 1990; 5:248-54. [PMID 2343039]
- Funch-Jensen P. The clinical value of sphincter of Oddi manometry. Gast Gastrointest Endosc Clin North Am 1993; 3:119-131.
- Cotton PB. Congenital anomaly of pancreas divisum as cause of obstructive pain and pancreatitis. Gut 1980; 21:105-14. [PMID 7380331]
- Delhaye M, Engelholm L, Cremer M. Pancreas divisum: congenital anatomic variant or anatomy? Contribution of endoscopic retrograde dorsal pancreatography. Gastroenterology 1985; 89:951-8. [PMID 4043675]
- Bret PM, Reinhold C, Taourel P, Guiband L, Atri M, Barkun AN. Pancreas divisum: evaluation with MR cholangiopancreatography. Radiology 1996; 199:99- 103. [PMID 8633179]
- Matos C, Metens T, Deviere J, Delhaye M, LeMoine O, Cremer M. Pancreas divisum: evaluation with secretin-enhanced magnetic resonance cholangiopancreatography. Gastrointest Endosc 2001; 53:726-33. [PMID 11375579]
- Tulassay Z, Papp J, Farkas IE. Diagnostic aspects of incomplete pancreas divisum. Gastrointest Endosc 1986; 32:428. [PMID 3803848]
- Sugawa C, Walt AJ, Nunez DC, Masuyama H. Pancreas divisum: is it a normal anatomic variant? Am J Surg 1987; 153:62-7. [PMID 3799894]
- Kim MH, Lee SS, Kim CD, Lee SK, Kim HJ, Park HJ, et al. Incomplete pancreas divisum: Is it merely a normal anatomic variant without clinical implications? Endoscopy 2001; 33:778-85. [PMID 11558032]
- Gelrud A, Sheth S, Banerjee S, Weed D, Shea J, Chuttani R, et al. Analysis of cystic fibrosis gener product (CFTR) function in patients with pancreas divisum and recurrent acute pancreatitis. Am J Gastroenterol 2004; 99:1557-62. [PMID 15307877]
- Jacob L, Geenen JE, Catalano MF, Johnson GK, Geenen DJ, Hogan WJ. Clinical presentation and sortterm outcome of endoscopic therapy of patients with symptomatic incomplete pancreas divisum. Gastrointest Endosc 1999; 49:53-7. [PMID 9869723]
- Traverso LW, Kozarek RA, Simpson T, Galagan KA. Pancreatic duct obstruction as a potential etiology of pancreatic adenocarcinoma: a clue from pancreas divisum. Am J Gastroenterol 1993; 88:117-9. [PMID 8420250]
- Kamisawa T, Yoshiike M, Egawa N, Tsuruta K, Okamoto A, Funata N. Pancreatic tumor associated with pancreas divisum. J Gastroenterol Hepatol 2005; 20:915-8. [PMID 15946141]

