Keywords
Pancreas; Pancreatic Diseases; Pancreatic Ducts; Pancreatitis, Chronic; Secretin; Smoking
INTRODUCTION
Chronic pancreatitis is characterized by progressive inflammation and scarring, leading to irreversible damage to the pancreas resulting in loss of exocrine and endocrine function [1, 2]. Clinical manifestations include severe and often debilitating abdominal pain, steatorrhea, and diabetes [3]. Current treatments can only provide temporary pain relief and manage complications but are unable to arrest this devastating illness. Both basic science and clinical researchers are actively investigating the pathogenic mechanisms of injury that result in chronic pancreatitis [4, 5, 6, 7]. Cigarette smoking has been established as an important risk factor for chronic pancreatitis [8, 9, 10, 11, 12, 13, 14]. An estimated 45.3 million adults in the United States are active cigarette smokers [15], and tobacco use still remains the single largest preventable cause of death and disease in the United States.
Direct testing of pancreatic fluid for hormonestimulated electrolyte or enzyme concentrations is considered the most sensitive test for pancreatic secretory dysfunction in diagnosing chronic pancreatitis [16, 17]. Specifically, measurement of secretin-stimulated pancreatic fluid total bicarbonate and peak bicarbonate concentration have been shown to be reliable predictors or “biomarkers” of early chronic pancreatic disease [18, 19]. Our clinical research group believes that evaluation of pancreas fluid from direct endoscopic pancreas function testing can provide insights into the pathogenic mechanisms of chronic pancreatitis [5, 20].
The aim of this study was to compare pancreatic duct cell secretory function in cigarette smokers [past and current] and never smokers by measuring peak bicarbonate concentration ([HCO3 -]) in endoscopic collected pancreatic fluid (PF).
METHODS
Study Subjects
Subjects were identified from the ePFT database at the Center for Pancreatic Disease, Brigham and Women’s Hospital, Boston, MA, USA. This study cohort was comprised of patients referred for evaluation for pancreatic disease, who underwent secretin-stimulated endoscopic pancreatic function testing (ePFT) between November 2007 and May 2011. Indications for ePFT included: diagnostic evaluation for suspected chronic pancreatitis and evaluation of pancreatic function in patients with established chronic pancreatitis. All ePFT patients were included in the sample cohort irrespective of age, gender, race, or etiology of chronic pancreatitis. Patients who had undergone any pancreatic surgery, for any reason, prior to imaging and ePFT were excluded from this analysis.
Data Collection
A data collection form was developed (V Kadiyala, DL Conwell) to record demographic information (age, gender, race), smoking status (former, current, never), alcohol intake (<20 g/day or >20 g/day), symptoms (pain, nausea, vomiting), imaging study findings (MRCP/sMRCP, CT, EUS), and laboratory results (peak pancreatic fluid [HCO3 -] and stool pancreatic elastase-1).
Endoscopic Pancreatic Function Test
Pancreatic function was assessed by measurement of peak PF [HCO3 -], collected by a 45-minute secretinstimulated endoscopic pancreatic function test (ePFT). The ePFT procedure was performed as previously described [21, 22]. Briefly, the patient was placed in left lateral decubitus position with the head slightly elevated and administered 0.2 μg/kg intravenous secretin (ChiRhoStim™, Human Secretin for injection, Burtonsville, MD, USA) over one minute. Esophagogastroduodenoscopy (EGD) was performed using a standard (10 mm) or thin (6 mm) upper endoscope for visualization of the esophagus, stomach, and duodenum. All gastric fluid was aspirated through the endoscope and discarded. Following secretin injection, pancreatic fluid (20-30 mL) was then aspirated from the duodenum at 15, 30, and 45 minutes into separate specimen traps. Fluid samples were placed on ice and sent to the laboratory for analysis. Bicarbonate concentration measurements were conducted in the CLIA-certified Brigham and Women's Hospital Clinical Chemistry Laboratory under the standard operating procedures on an AU640 (Olympus America, Center Valley, PA, USA) automated chemistry analyzer. Total bicarbonate was measured by the two-step phosphoenolpyruvate carboxylase-malate dehydrogenase enzymatic-photometric method [23]. Samples with results greater than the upper assay limit were diluted into the linear range. A peak PF [HCO3 -] less than 75 mEq/L was considered abnormal, indicating duct cell dysfunction [24].
Definition of Chronic Pancreatitis
Subjects were categorized based on the presence or absence of pancreatic disease, according to the MANNHEIM (multiple risk factor classification: alcohol consumption, nicotine consumption, hereditary factors, efferent pancreatic duct factors, immunologic factors, and rare miscellaneous and metabolic factors) criteria for chronic pancreatitis [25]. All radiologic studies were reviewed by two abdominal imaging radiologists (K Mortele, NI Sainani).
ETHICS
This study protocol was approved by the Institutional Review Board at the Brigham and Women’s Hospital. This study conforms to the ethical guidelines of the World Medical Association Declaration of Helsinki- Ethical Principles for Medical Research Involving Human Subjects. Data were collected retrospectively and patient informed consent was waived by the Institutional Review Board.
STATISTICS
Statistical analysis was performed using SAS Version 9.2 (SAS Institute Inc., Cary, NC, USA) by a PhD biostatistician (W Wang). Predictor variables included: age (discrete), gender (nominal: male, female), smoking status (nominal: past, current, never), alcohol intake ≥20 g/day (nominal: no, yes), definite chronic pancreatitis (nominal: no, yes). Outcomes included: peak PF [HCO3 -] (discrete), ePFT test result (nominal: normal, abnormal), stool pancreatic elastase-1 test result (nominal: normal, abnormal).
The Spearman rank test was used to determine the correlation of peak pancreatic fluid bicarbonate concentration to stage of chronic pancreatitis.
A. Comparison of Past and Current Smokers
Univariate analysis using the Fisher exact test and the Wilcoxon two-sample test was performed comparing the past smokers to the current smokers to determine if the two groups could be pooled to form a single smoking cohort.
B. Comparison of “Smokers” Cohort versus Never Smokers
Univariate analysis using the Fisher exact test and the Wilcoxon two-sample test was performed to compare the smoking cohorts to the never-smokers cohort for significant differences in predictor variables and outcomes. A contingency table was used to assess the risk magnitude of duct cell dysfunction in smokers and never smokers.
C. Determination of Independent Predictors of Duct Cell Function
Multivariate logistic regression was performed to determine if smoking status is an independent predictor of duct cell dysfunction (by abnormal peak PF [HCO3 -]), when controlling for age, gender, and associated covariates including chronic pancreatitis.
RESULTS
Study Cohort
Table 1 displays the demographic data of the 131 subjects who underwent function testing that were included in the data analysis. The mean age of the study sample was 48 years; 54 (41.2%) subjects were male; and 108 (82.4%) were white race. At the time of function testing, 33/131 (25.2%) subjects were past smokers; 41/131 (31.3%) were current smokers; and 57/131 (43.5%) subjects were never smokers.
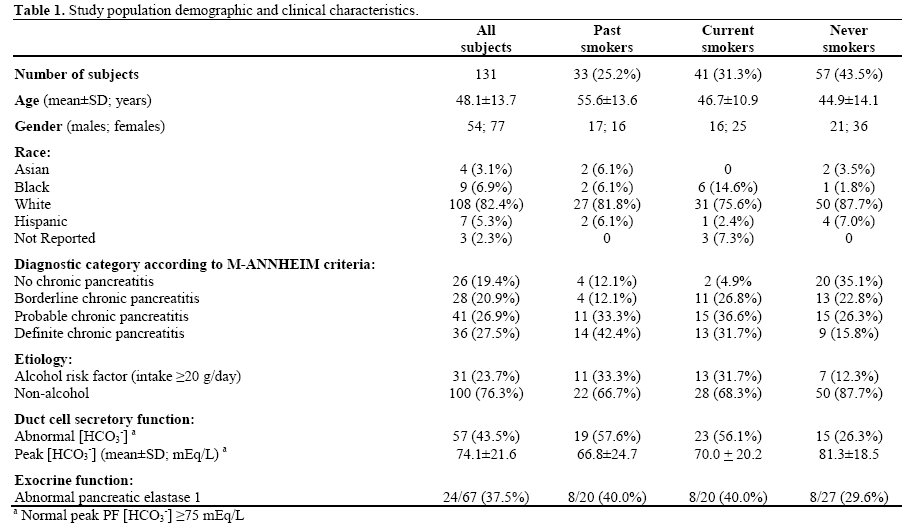
Clinical diagnosis for chronic pancreatitis was defined according to the M-ANNHEIM criteria [25]. Twenty six of the 131 subjects (19.4%) had no evidence of chronic pancreatitis; 28 (20.9%) had borderline chronic pancreatitis; 41 (26.9%) had probable chronic pancreatitis; and 36 (27.5%) had definite chronic pancreatitis. As expected, the mean peak [HCO3 -] was negatively correlated to the stage of chronic pancreatic disease according to the M-ANNHEIM diagnostic criteria and decreased from the no chronic pancreatitis group (88.3 mEq/L) to the definite chronic pancreatitis group (57.2 mEq/L) (rs=-0.579; P<0.001) (Table 2). Figure 1 shows the distribution of peak [HCO3 -] in male (Figure 1a) and female (Figure 1b) patients across all diagnostic categories in past, current and never smokers.
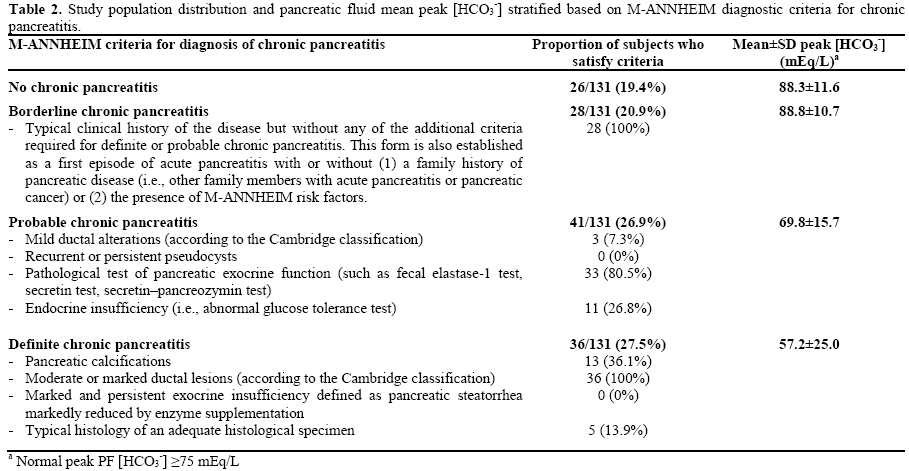
Figure 1. Box plots showing the distribution of mean peak
pancreatic fluid [HCO3-] in male (a.) and female (b.) never-smokers,
past smokers and current smokers, across M-ANNEHIM diagnostic
categories for chronic pancreatitis. (* Suspected outliers; ∘ Strongly
suspected outliers)
Effect of Smoking
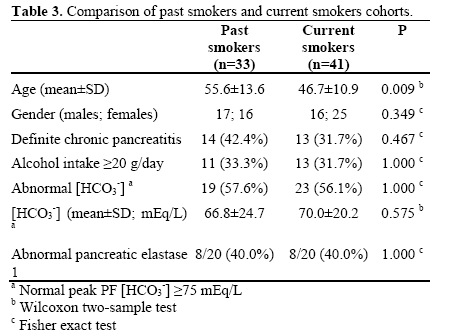
Current and past smokers were combined to form a “Smokers” cohort. As shown in Figure 2, when compared to never smokers, the mean peak PF [HCO3 -] was significantly lower in both current smokers (P=0.005) and past smokers (P=0.005). Table 3 shows that of those 74 subjects with a history of smoking, 33 (44.6%) were past smokers, and 41 (55.4%) were current smokers at the time of function testing. Past smokers were found to be significantly older than current smokers (P=0.002). There was no statistical difference in peak [HCO3 -] between past smokers (66.8±24.7 mEq/L) and current smokers (70.0±20.2 mEq/L) (P=0.575). There was no statistical difference between the two groups with regard to gender composition and proportion of subjects with definite chronic pancreatitis, daily alcohol intake ≥20 g, abnormal peak PF [HCO3 -], and abnormal stool pancreatic elastase-1. Based on these similar characteristics, past and current smokers were combined into one “smokers cohort” for data analysis. Also shown in Figure 2, when compared to never smokers, the mean peak PF [HCO3 -] was significantly lower in the “smokers cohort” (P<0.001).
Figure 2. Comparison of mean peak pancreatic fluid [HCO3-] and
95% CI among all cohorts, using the Wilcoxon two-sample test.
(Normal peak PF [HCO3-] ≥75 mEq/L).
Demographic Characteristics
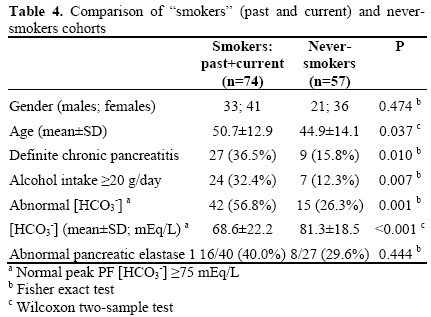
Demographic characteristics of the smokers cohort (past and current) compared to the never-smokers cohort are shown in Table 4. There were 74 subjects in the smokers cohort and 57 subjects in the neversmokers cohort. There was no difference in gender composition. However, the smokers cohort was significantly older (P=0.037) and as expected, had a greater proportion of subjects with definite chronic pancreatitis (P=0.010), daily alcohol intake ≥20 g (P=0.012), and abnormal peak PF [HCO3 -] (P<0.001). The mean peak PF [HCO3 -] in the smokers cohort (68.6±22.2 mEq/L) was significantly lower than that in never smokers (81.3±18.5 mEq/L) (P<0.001). There was no observed difference in the proportion of patients with abnormal stool pancreatic elastase-1 when smokers and never smokers were compared.
Risk of Pancreatic Duct Cell Dysfunction
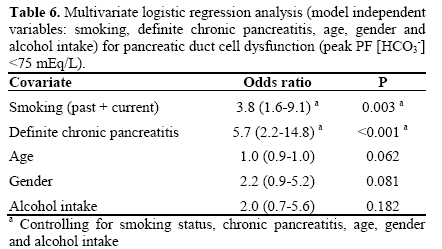
Smoking (past and current), definite chronic pancreatitis, and increased alcohol intake ≥20 g/day are associated with increased risk of pancreatic duct cell dysfunction. Table 5 shows the risk ratios (RR) and their corresponding 95% confidence intervals. Cigarette smoking (RR: 2.2, 95% CI: 1.3-3.5; P<0.001), diagnosis of definite chronic pancreatitis (RR: 2.2, 95% CI: 1.6-3.2; P<0.001), and alcohol consumption ≥20 g/day (RR: 1.6, 95% CI: 1.1-2.4; P=0.033) were all associated with an increased risk of duct cell secretory dysfunction. These three factors, including age and gender were entered as covariates in a multiple logistic regression model to determine the individual contributions of each factor in predicting duct cell dysfunction. As seen in Table 6, smoking (odds ratio, OR: 3.8, 95% CI: 1.6-9.1; P=0.003) and definite chronic pancreatitis were independent predictors of duct cell dysfunction when controlling for smoking status, chronic pancreatitis, age, gender, and increased alcohol intake. Furthermore, there was no interaction between smoking plus increased alcohol intake (P=0.571) or smoking plus gender (P=0.543) in predicting duct cell dysfunction.

DISCUSSION
We have shown that cigarette smoking is associated with impaired pancreatic duct cell function. Specifically, the mean peak pancreatic fluid [HCO3 -] was significantly lower in both past and current smokers when compared to never smokers, and the risk of duct cell secretory dysfunction in subjects who smoked was approximately twice (RR: 2.2) the risk in never smokers. Furthermore, smoking was found to be independently associated with duct cell dysfunction (i.e., peak PF [HCO3 -] <75 mEq/L), when controlling for age, gender, increased alcohol intake, and diagnosis of chronic pancreatitis. A diagnosis of chronic pancreatitis was also independently associated with abnormal duct cell function. Often associated with chronic pancreatitis and common among cigarette smokers, increased alcohol intake was also found to be associated with elevated risk of low peak PF [HCO3 -]. However, the logistic regression model demonstrated that cigarette smoking impaired duct cell function independent of any effect of increased alcohol consumption and chronic pancreatitis. These findings add to the growing body of evidence that cigarette smoking is harmful to the human pancreas. Our results show that pancreas duct cell secretion/function is impaired in cigarette smokers.
Animal models as well as human epidemiologic and pathology studies confirm that smoking is deleterious to the pancreas in both acute and chronic pancreatitis [26, 27, 28, 29]. Continued smoking exposure has also been associated with worsening disease severity, development of parenchymal calcifications, and pancreatic carcinoma [26, 30, 31, 32, 33]. Recent elucidation of the role of inflammatory mediators (i.e. growth factors, chemokines, and cytokines) in pancreatic stellate cell physiology has improved our understanding of mechanisms leading to pancreas fibrosis and adenocarcinoma [34, 35, 36, 37]. Cigarette smoke exposure has been shown to induce expression of pro-fibrotic inflammatory mediators in animal models [28]. There is also evidence to suggest that cigarette smoking may impair pancreatic secretory function even in the absence of overt pancreatic disease [26, 38, 39, 40]. Further studies in smokers and nonsmokers are warranted. We have previously shown that our current endoscopic pancreas fluid collection method can be used to collect pancreas fluid for in depth cytokine and chemokine analyses [41]. These molecular analyses of pancreas fluid may provide insight into the mechanisms of smoking-induced injury.
There have been a limited number of human studies examining the effects of long-term cigarette smoking on pancreatic secretory function. Our findings agree with those of previous investigators that habitual smokers had significantly lower peak PF [HCO3 -] [39, 40]. A recent study also found that current cigarette smoking was independently associated with secretory dysfunction (defined as [HCO3 -] <80 mEq/L) and calcifications [26]. Human studies generally agree that smoking appears to acutely impair duct cell secretory function [38, 39, 40, 42]. Canine studies have shown that intravenous nicotine generally appeared to suppress duct cell function; however, these experiments did note variable responses in pancreatic fluid volume, secreted bicarbonate, and bicarbonate concentration [43, 44, 45].
The aforementioned physiological effects are supported by human autopsy studies and animal models demonstrating smoking-induced pancreatic inflammation and injury. Examination of human pancreata at autopsy shows that smokers are more likely to have moderate-severe pancreatic fibrosis and specifically more intralobular fibrosis [29]. In response to cigarette smoke exposure, rat models have exhibited pancreatic inflammation, focal fibrosis, acinar cell stress, and disruption of normal enzyme secretion [46, 47].
There are limitations in our study. Specifically, we were unable to quantify the duration and extent of smoking (pack-year history) and alcohol intake due to inconsistent reporting in the medical record. This is especially relevant as there is evidence to suggest that smoking increases the risk of chronic pancreatitis in a dose-dependent manner [13, 27]. We were also not able to determine precisely when former smokers ceased smoking relative to onset of symptoms, diagnosis of chronic pancreatitis, and stage of disease process. In chronic pancreatitis patients, it has been demonstrated that smoking cessation soon after onset of symptoms actually reduces the risk of developing calcifications [48]; however, secretory function before and after smoking cessation has not been compared. Contrary to our findings, previous investigators have found that former smoking was not a predictor of chronic pancreatitis [26]. However, it should be noted that in addition to limited information about smoking intensity and timing of smoking cessation, we were unable to confirm patients’ reports of continuous abstinence from cigarette smoking. A significant number of false reports regarding smoking status would certainly confound any comparisons between the groups. Lastly, the generalizability of our study was limited by a referral bias inherent to the study sample. This patient sample was drawn from subjects referred to the Brigham and Women’s Hospital Center for Pancreatic Disease and does not represent the overall general population. For example, the prevalence of definite chronic pancreatitis (16%) and abnormally low peak bicarbonate concentrations (26%) in our neversmoker cohort was greater than would be expected in the general population [49].
In conclusion, cigarette smoking is independently associated with impaired pancreatic duct cell secretory function, regardless of age, gender, alcohol intake, and the presence of chronic pancreatitis. Further investigation is needed to determine the impact of both smoking dose exposure and smoking cessation on duct cell function. Our findings join a growing body of evidence that suggests smoking cessation is likely vital to the prevention and management of chronic pancreatitis. Smoking cessation should be encouraged early in disease management in hopes of retarding deleterious effects on the pancreas. But more importantly, endoscopic collection and in depth analysis of pancreas fluid may open new areas of research for better understanding the mechanisms of smoking induce pancreatic injury [50].
Acknowledgements
American College of Gastroenterology Clinical Research Grant (2007 DL Conwell). Center for Pancreatic Disease, Brigham and Women’s Hospital (PA Banks)
Financial support
American College of Gastroenterology Clinical Research Grant (2007, DL Conwell). Center for Pancreatic Disease Research Fund, Brigham and Women’s Hospital (PA Banks). Translational Research Fund in Pancreatic Disease, Brigham and Women’s Hospital (DL Conwell, PA Banks).
Potential competing interests
None
References
- Conwell DL, Banks PA. Chronic pancreatitis. Curr Opin Gastroenterol 2008;24:586-90.
- Stevens T, Conwell DL, Zuccaro G. Pathogenesis of chronic pancreatitis: an evidence-based review of past theories and recent developments. Am J Gastroenterol 2004;99:2256-70.
- Warshaw AL, Banks PA, Fernandez-Del Castillo C. AGA technical review: treatment of pain in chronic pancreatitis. Gastroenterology 1998;115:765-76.
- Whitcomb DC, Yadav D, Adam S, et al. Multicenter approach to recurrent acute and chronic pancreatitis in the United States: the North American Pancreatitis Study 2 (NAPS2). Pancreatology 2008;8:520-31.
- Paulo JA, Kadiyala V, Lee LS, Banks PA, Conwell DL, Steen H. Proteomic Analysis (GeLC-MS/MS) of ePFT-Collected Pancreatic Fluid in Chronic Pancreatitis. J Proteome Res.
- Paulo JA, Lee LS, Banks PA, Steen H, Conwell DL. Proteomic Analysis of Formalin-Fixed Paraffin-Embedded Pancreatic Tissue Using Liquid Chromatography Tandem Mass Spectrometry. Pancreas.
- Pandol SJ, Gorelick FS, Lugea A. Environmental and genetic stressors and the unfolded protein response in exocrine pancreatic function - a hypothesis. Front Physiol;2:8.
- Yadav D, Slivka A, Sherman S, et al. Smoking is underrecognizedas a risk factor for chronic pancreatitis. Pancreatology;10:713-9.
- Cote GA, Yadav D, Slivka A, et al. Alcohol and smoking as risk factors in an epidemiology study of patients with chronic pancreatitis. Clin Gastroenterol Hepatol;9:266-73; quiz e27.
- Yadav D, Whitcomb DC. The role of alcohol and smoking in pancreatitis. Nat Rev Gastroenterol Hepatol;7:131-45.
- Yadav D, Hawes RH, Brand RE, et al. Alcohol consumption, cigarette smoking, and the risk of recurrent acute and chronic pancreatitis. Arch Intern Med 2009;169:1035-45.
- Yadav D, Eigenbrodt ML, Briggs MJ, Williams DK, Wiseman EJ. Pancreatitis: prevalence and risk factors among male veterans in a detoxification program. Pancreas 2007;34:390-8.
- Andriulli A, Botteri E,Almasio PL, Vantini I, Uomo G, Maisonneuve P. Smoking as a cofactor for causation of chronic pancreatitis: a meta-analysis. Pancreas 2010;39:1205-10.
- Lin Y, Tamakoshi A, Hayakawa T, Ogawa M, Ohno Y. Cigarette smoking as a risk factor for chronic pancreatitis: a case-control study in Japan. Research Committee on Intractable Pancreatic Diseases. Pancreas 2000;21:109-14.
- Anju TR, Korah PK, Jayanarayanan S, Paulose CS. Enhancedbrain stem 5HTA receptor function under neonatal hypoxic insult:role of glucose, oxygen, and epinephrine resuscitation. Mol Cell Biochem 2011;354:151-60.
- Stevens T, Conwell DL, Zuccaro G, et al. Electrolyte composition of endoscopically collected duodenal drainage fluid after synthetic porcine secretin stimulation in healthy subjects. Gastrointest Endosc 2004;60:351-5.
- Somogyi L, Ross SO, Cintron M, Toskes PP. Comparison of biologic porcine secretin, synthetic porcine secretin, and synthetic human secretin in pancreatic function testing. Pancreas 2003;27:230-4.
- Chowdhury RS, Forsmark CE. Review article: Pancreatic function testing. Aliment Pharmacol Ther 2003;17:733-50.
- Stevens T, Dumot JA, Zuccaro G, Jr., et al. Evaluation of ductcelland acinar-cell function and endosonographic abnormalities in patients with suspected chronic pancreatitis. Clin Gastroenterol Hepatol 2009;7:114-9.
- Paulo JA, Lee LS, Wu B, et al. Identification of pancreas-specific proteins in endoscopically (endoscopic pancreatic function test) collected pancreatic fluid with liquid chromatography--tandem mass spectrometry. Pancreas;39:889-96.
- Conwell DL, Zuccaro G, Jr.,Vargo JJ, et al. An endoscopic pancreatic function test with synthetic porcine secretin for the evaluation of chronic abdominal pain and suspected chronic pancreatitis. Gastrointest Endosc 2003;57:37-40.
- Wu B, Conwell DL. The endoscopic pancreatic function test. Am J Gastroenterol 2009;104:2381-3.
- Forrester RL, Wataji LJ, Silverman DA, Pierre KJ. Enzymatic method for determination of CO2 in serum. Clin Chem 1976;22:243-5.
- Stevens T, Conwell DL, Zuccaro G, Jr., Lewis SA, Love TE. The efficiency of endoscopic pancreatic function testing is optimized using duodenal aspirates at 30 and 45 minutes after intravenous secretin. Am J Gastroenterol 2007;102:297-301.
- Schneider A, Lohr JM, Singer MV. The M-ANNHEIM classification of chronic pancreatitis: introduction of a unifying classification system based on a review of previous classifications of the disease. J Gastroenterol 2007;42:101-19.
- Law R, Parsi M, Lopez R, Zuccaro G, Stevens T. Cigarette smoking is independently associated with chronic pancreatitis. Pancreatology 2010;10:54-9.
- Yadav D, Whitcomb DC. The role of alcohol and smoking in pancreatitis. Nat Rev Gastroenterol Hepatol 2010;7:131-45.
- Wittel UA, Hopt UT, Batra SK. Cigarette smoke-inducedpancreatic damage: experimental data. Langenbecks Arch Surg 2008;393:581-8.
- vanGeenen EJ, Smits MM,Schreuder TC, van der Peet DL, Bloemena E, Mulder CJ. Smoking is related to pancreatic fibrosis in humans. Am J Gastroenterol; 106:1161-6; quiz 7.
- Brand RE, Greer JB, Zolotarevsky E, et al. Pancreatic cancer patients who smoke and drink are diagnosed at younger ages. Clin Gastroenterol Hepatol 2009;7:1007-12.
- Lowenfels AB, Maisonneuve P. Epidemiology and risk factorsfor pancreatic cancer. Best Pract Res Clin Gastroenterol 2006;20:197-209.
- Maisonneuve P, Lowenfels AB, Mullhaupt B, et al. Cigarettesmoking accelerates progression of alcoholic chronic pancreatitis.Gut 2005;54:510-4.
- Cavallini G, Talamini G, Vaona B, et al. Effect of alcohol andsmoking on pancreatic lithogenesis in the course of chronic pancreatitis. Pancreas 1994;9:42-6.
- Apte M, Pirola R, Wilson J. The fibrosis of chronic pancreatitis: new insights into the role of pancreatic stellate cells. Antioxid Redox Signal;15:2711-22.
- Apte M, Pirola R, Wilson J. New insights into alcoholic pancreatitis and pancreatic cancer. J Gastroenterol Hepatol 2009;24Suppl 3:S51-6.
- Apte MV, Pirola RC, Wilson JS. Pancreas: alcoholic pancreatitis- -it's the alcohol, stupid. Nat Rev Gastroenterol Hepatol 2009;6:321-2.
- Apte MV, Pirola RC, Wilson JS. Molecular mechanisms of alcoholic pancreatitis. Dig Dis 2005;23:23240.
- Murthy SN, Dinoso VP, Jr., Clearfield HR, Chey WY. Simultaneous measurement of basal pancreatic, gastric acidsecretion, plasma gastrin, and secretin during smoking. Gastroenterology 1977;73:758-61.
- Bynum TE, Solomon TE, Johnson LR, Jacobson ED. Inhibition of pancreatic secretion in man by cigarette smoking. Gut 1972;13:361-5.
- Brown P. The influence of smoking on pancreatic function in man. Med J Aust 1976;2:290-3.
- Paulo JA, Lee LS, Wu B, Banks PA, Steen H, Conwell DL. Cytokine profiling of pancreatic fluid using the ePFT collection method in tandem with a multiplexed microarray assay. J Immunol Methods 2011;369:98-107.
- Bochenek WJ, Koronczewski R. Effects of cigarette smoking on bicarbonate and volume of duodenal contents. Am J Dig Dis 1973;18:729-33.
- Konturek SJ, Solomon TE, McCreight WG, Johnson LR,Jacobson ED. Effects of nicotine on gastrointestinal secretions.Gastroenterology 1971;60:1098-105.
- Boden G, Shore LS, Essa-Koumar N, Landor JH. Effect of nicotine on serum secretin and exocrine pancreatic secretion. Am J Dig Dis 1976;21:974-7.
- Konturek SJ, Dale J, Jacobson ED, Johnson LR. Mechanisms of nicotine-induced inhibition of pancreatic secretion of bicarbonate in the dog. Gastroenterology 1972;62:425-9.
- Wittel UA, Pandey KK, Andrianifahanana M, et al. Chronic pancreatic inflammation induced by environmental tobacco smoke inhalation in rats. Am J Gastroenterol 2006;101:148-59.
- Wittel UA, Singh AP, Henley BJ, et al. Cigarette smoke-induced differential expression of the genes involved in exocrine function of the rat pancreas. Pancreas 2006;33:364-70.
- Talamini G, Bassi C, Falconi M, et al. Smoking cessation at the clinical onset of chronic pancreatitis and risk of pancreatic calcifications. Pancreas 2007;35:320-6.
- Yadav D, Timmons L, Benson JT, Dierkhising RA, Chari ST. Incidence, prevalence, and survival of chronic pancreatitis: a population-based study. Am J Gastroenterol 2011;106:2192-9.
- Paulo JA, Lee LS, Wu B, et al. Identification of pancreas-specific proteins in endoscopically (endoscopic pancreatic function test) collected pancreatic fluid with liquid chromatography-tandem mass spectrometry. Pancreas 2010;39:889-96.



