Vallath Balakrishnan1, Ambika Gopalakrishnan Unnikrishnan1, Varghese Thomas2 , Gourdas Choudhuri3, Peda Veeraraju4, Shivram Prasad Singh5, Pramod Garg6, Cannore Ganesh Pai7, Raveendranathan Nair Sobhana Devi8, Deepak Bhasin9, Venkataraman Jayanthi10, Narayanan Premalatha11, Ashok Chacko12, Premashish Kar13, Ramesh Roop Rai14, Ramesh Rajan15, Narayanan Subhalal15, Rajiv Mehta16, Sri Prakash Mishra17, Manisha Dwivedi17, Kattoor Ramakrishnan Nair Vinayakumar18, Ashok Kumar Jain19, Kalidas Biswas20, Sunil Mathai21, Jaison Varghese22, Hariharan Ramesh23, Thomas Alexander24, Jacob Philip25, Vigna Venugopal Raj26, Ankarath Vinodkumar27, Srikanth Mukevar28, Prabha Sawant29, Prem Nair1, Harish Kumar1, Surendran Sudhindran1, Puneet Dhar1, Othayil Vayoth Sudheer1, Karimassery Ramaiyer Sundaram1, Bailuru Vishwanath Tantri30, Devinder Singh31, Thekkayil Rajindra Nath32
1Amrita Institute of Medical Sciences, Cochin, India
2Medical College, Calicuto, India
3Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India
4AMC Hospital, Vishakapatnam, India
5SCB Medical College, Cuttack, India
6All India Institute of Medical Sciences, New Delhi, India
7Kasturba Medical College, Manipal, India
8Medical College, Kottayam, India
9Postgraduate Institute of Medical Education and Research, Chandigarh, India
10Stanley Medical College, Chennai, India
11Medical College, Thrissur, India
12Christian Medical College, Vellore, India
13Maulana Azad Medical College, New Delhi, India
14SMS Medical College, Jaipur, India
15Medical College, Trivandrum, India
16Shri Mahavir General Hospital, Surat, India
17Motilal Nehru Medical College, Allahabad, India
18Medical College, Thiruvananthapuram, India
19Institute of Medical Sciences, BHU, Varanasi, India
20Consultant Gastroenterologist, Kolkata, India
21Medical Trust Hospital, Cochin
22Devamatha Hospital, Koothatukulam, India
23Lakeshore Hospital, Cochin, India
24Holy Cross Hospital, Kottiyam, India
25Cosmopolitan Hospital, Trivandrum, India
26Manipal Hospital, Bangalore, India
27Ernakulam Medical Center, Cochin, India
28Consultant Gastroenterologist, Nagpur, India
29Lokmanya Tilak Medical College, Mumbai, India
30Consultant Gastroenterologist, Mangalore, India
31Apollo Hospital, Bilaspur, India
32Baby Memorial Hospital, Calicut. India
- *Corresponding Author:
- Vallath Balakrishnan
Indian Pancreatitis Study Group
Coordinating Office
Amrita Institute of Medical Sciences
Cochin, Kerala
India,682026
Phone: +91-484.400.1225
Fax: +91-484.280.2020
E-mail: vbalakrishnan@aims.amrita.edu; ipans@aims.amrita.edu
Received June 20th, 2008 - Accepted June 30th, 2008
Keywords
Calculi; Diabetes Mellitus; Epidemiology; India; Islets of Langerhans; Manihot; Pancreas; Pancreas, Exocrine; Pancreatitis, Alcoholic; Pancreatitis, Chronic; Prevalence
Acknowledgements
The authors of the study are all collaborators of the Indian Pancreatitis Study Group (IPANS). National Coordinator: V Balakrishnan; Assistant Coordinator: AG Unnikrishnan; Institutional IPANS Committee: P Nair, P Dhar, H Kumar, S Sudhindran, OV Sudheer. IPANS Writing Committee: V Balakrishnan, AG Unnikrishnan, P Dhar, SP Singh, and G Pai. IPANS Secretaries: Mr. N Sudhakaran, Ms. V Vidya, Ms. R Lakshmi, and Ms. AS Nair
INTRODUCTION
Chronic pancreatitis is a heterogeneous disease. Worldwide, alcoholism is the most common cause of chronic pancreatitis. However, in many tropical countries like India, the etiology frequently includes socalled ‘tropical chronic pancreatitis’ [1, 2, 3]. Genetic mutations are responsible for a proportion of subjects with tropical chronic pancreatitis, although the majority of such patients do not have mutations [4]. Clearly, any understanding of the complexity of chronic pancreatitis in India necessitates a study of the association between clinical patterns and risk factors of the disease as a first step.
There has been no systematic nationwide study on the clinical profile of subjects with chronic pancreatitis from the Indian subcontinent, although many sporadic reports from some regions exist in the medical literature. [5, 6, 7, 8, 9, 10, 11, 12]. In this study, we sought to ascertain the clinical profile of subjects with chronic pancreatitis in India, especially with regard to risk factors, clinical features and therapeutic modalities. To our knowledge, this is the first report of a prospective, nationwide study of chronic pancreatitis carried out in India.
METHODS
The Indian Pancreatitis Study Group was conceived at a National Consensus Meeting on Tropical Chronic Pancreatitis and Pancreatic Diabetes in India. The first meeting was held at the Amrita Institute of Medical Sciences, Cochin, comprising a core group of pancreatologists, endocrinologists and pancreatic surgeons. A common proforma, and subsequently, an online data entry website were created (www.ipans.org). The emphasis was on simplicity of the proforma to maximize compliance. Investigators wishing to participate in the study joined the study online, and entered clinical information on patients with chronic pancreatitis into an online database [13]. Major centers in the country were subsequently invited to enroll patients in order to ensure that the registry would be representative nationwide. The only requirement requested was that the data be entered prospectively, consecutively and completely. A copy of every patient’s information sheet was asked to be kept at the local site. Centers expressing unwillingness to enter data due to paucity of dedicated research or resident manpower were encouraged to fill out the paper printout of the proforma and the data was entered by the coordinating center. After the website had been put up, the information was circulated to all with at least two telephone or e-mail reminders to each center.
A national network of thirty-two centers contributed data (Figure 1). Clinical data were entered prospectively. The details of the proforma are available at www.ipans.org; briefly, information on the following parameters was collected: age, gender, mode of presentation of illness, family history, history of diabetes and its complications, history of alcohol as well as cassava (tapioca) intake, details of clinical examination, results of investigations, imaging study results, mode of treatment of diabetes, analgesics, the use of pancreatic enzyme supplements, frequency of endotherapy and surgery.
Figure 1. Map of India showing the various centers
participating in the study.
The data were analyzed at the coordinating center and presented at the first follow up registry meeting in Cochin (February, 2007). The coordinating center prepared the initial draft which was circulated to all members of the steering committee. Suggested modifications were included in the final version.
Definitions and Diagnostic Criteria
Chronic pancreatitis was defined by features consistent with irreversible pancreatic inflammation, i.e., clinical, structural or functional abnormality of the pancreas [14]. The presence of pancreatic calculi or ductal irregularity/parenchymal atrophy was determined at imaging using ultrasonography, CT scan, MRI, magnetic resonance cholangiopancreatography (MRCP), cholangiopancreatography (ERCP) or endoscopic ultrasound (EUS). Ultrasound and CT were the usual initial investigations. Other imaging modalities were carried out when indicated. Diabetes mellitus was diagnosed if the fasting plasma glucose value was equal to, or greater than, 126 mg/dL confirmed on two occasions and/or a plasma glucose value equal to, or greater than, 200 mg/dL after a two-hour glucose load confirmed on two occasions, and/or requirements for insulin or oral hypoglycemic drugs. Alcohol intake was considered significant in chronic pancreatitis patients who had been taking the equivalent of 80 g or more of ethanol/day for at least five years. Cassava intake was considered significant if cassava dishes formed the main portion of the meal on at least three occasions per week [15].
Since there are no clearly defined criteria for “tropical pancreatitis”, we defined it based on three most distinctive features of the disease: i) onset at less than 30 years of age; ii) a BMI less than 18 kg/m2; iii) subjects with chronic pancreatitis who also did not consume alcohol and who did not have any other specific cause for the pancreatitis [16, 17]. We then sought to determine how many among the current cohort would fit these criteria.
STATISTICS
Data are reported as means±SD, ranges and frequencies. SPSS for Windows (Version 11) was used for data management and statistical analysis. Association between two categorical variables was tested using the chi-square test or the Fisher’s exact test wherever appropriate. The Mann-Whitney test was also used for continuous variables. Stepwise logistic regression analysis was performed in order to determine the odds ratio (OR) of independent factors in chronic pancreatitis. Age, gender, presence of diabetes and duration of illness were all included as covariates. A two-tailed P value of less than 0.05 was considered statistically significant.
RESULTS
Although data is still being entered, we decided to include all patient data entered prior to a cut-off date, coinciding with the first follow-up meeting of the group. Thus, by the cut-off date, a total of 1,086 patients had been studied for over a period of 18 months. Complete information on risk factors was available on 1,033 subjects and all subsequent analyses were carried out on these subjects. The mean age was 39.7±14.1 years. The mean duration of the disease was 6.95±8.16 years. The mean BMI was 19.8±3.3 kg/m2. Among the subjects studied, 733 (71.0%) were male and 300 (29.0%) were female. The socioeconomic distribution of the subjects was: upper class 84 (8.1%), middle class 600 (58.1%) and lower class 349 (33.8%).
Factors Related to the Disease
Of the 1,033 subjects, 622 (60.2%) did not have any of the risk factors generally described in the literature while 400 (38.7%) were chronic consumers of alcohol and the rest (n=11; 1.1%) had rare risk factors. Other risk factors included pancreas divisum (n=4; 0.4%) and hyperparathyroidism (n=2; 0.2%); in addition, one patient each (0.1%) had agenesis of the pancreas, autoimmune pancreatitis, hypertriglyceridemia-related pancreatitis, trauma and microlithiasis. Table 1 shows the distribution of chronic alcohol consumers and smokers according to gender. Among the 400 subjects who were chronic alcoholics, detailed alcohol intake data was available in 199 (49.8%) subjects; mean daily intake was 148.9±78.1 g/day (range: 80-400 g/day). The mean duration of alcohol intake was 17.8±7.8 years (range: 10-50 years). The mean cumulative intake was 565±651 (kg of alcohol). Of the 733 males with chronic pancreatitis, 394 (53.8%) had alcoholic pancreatitis.
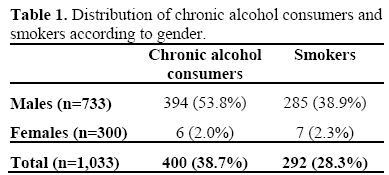
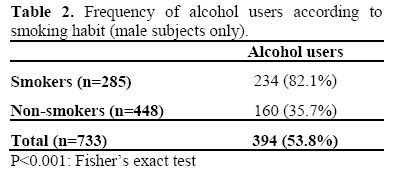
Two hundred and ninety-two (28.3%) of the 1,033 subjects were smokers and, in particular, of the 733 male subjects 285 (38.9%) were smokers (Table 2). Fifty-nine percent (234/394) of the male alcoholics were smokers and, conversely, 82.1% (234/285) of the male smokers were alcoholics. One hundred and eighty-nine subjects (18.3%) reported significant cassava intake.
Alcoholic vs. Non-alcoholic Pancreatitis
Subjects with chronic pancreatitis who consumed alcohol had a mean age of 45.5±10.4 years as compared with a mean age of 36.6±14.9 years in the non-alcoholic group (P<0.001).
Tropical Pancreatitis
Thirty-nine of the 1,033 subjects (3.8%) fulfilled the set of classical criteria for tropical pancreatitis.
Family History
In their family history, twenty-two (2.1%) subjects listed pancreatitis in at least one additional family member. One hundred and forty-one subjects (13.6%) gave a family history of diabetes. Four patients (0.4%) gave a family history of pancreatic cancer
Diabetes-Related Profile
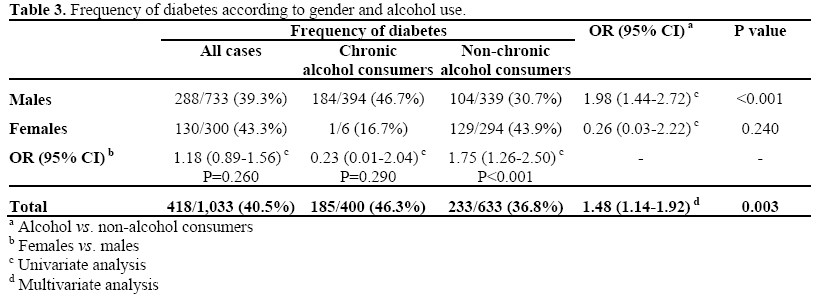
Of the 1,033 subjects with chronic pancreatitis who were studied, 418 (40.5%) had diabetes mellitus. Data regarding diabetes therapy was available in 399 subjects (95.5%): 67 (16.8%) were controlled by diet, 134 subjects (33.6%) were on oral hypoglycemic agents and 198 subjects (49.6%) were on insulin.
Table 3 shows the frequency of diabetes according to gender and alcohol consumption. One hundred and eighty-four (46.7%) of the 394 alcoholic males versus 104 (30.7%) of the 339 non-alcoholic males had diabetes (OR=1.98; 95%CI: 1.44-2.72; P<0.001). Multivariate analysis of frequency of diabetes versus alcohol and gender was carried out. A significantly higher frequency of diabetes was found in alcoholics when compared to nonalcoholics (OR: 1.48; 95%CI: 1.14-1.92; P=0.003). The odds ratio of having diabetes for non-alcoholic females (129/294; 43.9%) compared to non-alcoholic males was 1.75 (95%CI: 1.26-2.50; P<0.001). The most common presentation of diabetes was asymptomatic hyperglycemia (n=100; 23.9% of 418 diabetic subjects).
Treatment Modalities for Chronic Pancreatitis
Eight hundred and forty-nine subjects (82.2%) were on medical therapy. Surgery had been performed in 85 (8.2%) and endotherapy had been carried out in 99 (9.6%).
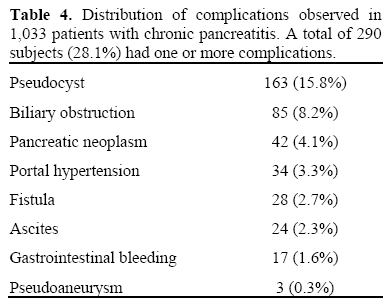
Complications of Chronic Pancreatitis
One or more complications occurred in 290 (28.1%) patients. The complications of chronic pancreatitis in these 290 patients are listed in Table 4.
Pain and Therapeutic Outcome
Pain was present in 971 subjects (94.0%). Of the 85 subjects who were reported to have undergone surgery, relief of pain was reported in 31 subjects (36.5%)
Imaging Modalities
Ultrasound data was available in 831 patients (80.4%) and the most common findings were: calculi (n=579; 69.7%), dilated duct (n=527; 63.4%), atrophy (n=227; 27.3%), mass (n=64; 7.7%), and common bile duct dilatation (n=73; 8.8%).
CT scan findings were available in 489 patients (47.3%) and the most frequent findings included: pancreatic calculi (n=316; 64.6%), dilated pancreatic duct (n=284; 58.1%), atrophy (n=176; 36.0%), mass (n=73; 14.9%) and common bile duct dilatation (n=56; 11.5%).
Magnetic resonance cholangiopancreatography (MRCP) was available in 104 patients (10.1%) and the most common findings were: calculi (n=44; 42.3%), stricture (n=40; 38.5%), fistula (n=16; 15.4%), and common bile duct dilatation (n=89; 85.6%). ERCP was carried out in 172 patients (16.7%). Calculi were present in 84 (48.8%) patients, dilated duct in 143 (83.1%), fistulae in 17 (9.9%) and strictures in 62 (34.0%) patients.
DISCUSSION
We report the results of the first nationwide, prospective study of subjects with chronic pancreatitis from the Indian subcontinent. The results of our study, conducted on 1,086 patients, clearly show that: i) idiopathic pancreatitis is the most common form of chronic pancreatitis in India, accounting for about two-thirds of the cases; ii) one-third of all cases are due to alcoholic pancreatitis and in males, alcoholism accounted for nearly half the cases; iii) ‘tropical’ chronic pancreatitis, as classically described, is now less common. As compared to previous reports [2, 18, 19], there is an increasing prevalence of alcoholic chronic pancreatitis in India. This could be because alcohol consumption has steeply increased in India (and particularly in the state of Kerala) over the last two decades, reflecting changing lifestyles [20, 21]. The male predominance of alcoholic chronic pancreatitis in India is likely to be because alcoholism is quite uncommon amongst Indian women. The mean daily intake, as well as the duration of the consumption of alcohol, is similar to that reported by subjects with alcoholic chronic pancreatitis from the developed world [14].
A notable finding of this paper was that of documenting the decline of ‘tropical chronic pancreatitis’ in its classical sense. Several studies from South India have reported that ‘tropical chronic pancreatitis’ has classically been described as occurring in young subjects (16-30 years) with significant malnutrition and a tendency of exocrine and endocrine dysfunction as well as a higher tendency to malignancy [22, 23]. In this series, using a rigid age-based cut-off, only 39 out of the 1,033 subjects (3.8 %) could be defined as having the classical form of ‘tropical’ chronic pancreatitis.
Smoking as a factor related to chronic pancreatitis is important in India, as evidenced by the fact that about 28% (n=292) of the 1,033 subjects were smokers. Interestingly and somewhat expectedly, given the gender-related differences in this part of the world, almost all the smokers were males. Smoking and alcohol tended to occur together: the majority of the alcoholics were smokers and, conversely, the majority of the smokers were alcoholics. Smoking is now recognized as an independent risk factor for chronic pancreatitis, and it is a leading risk factor for pancreatic cancer [24]. The frequency of smoking is increasing in India, and this is an important cause of concern [25, 26].
Cassava, as a cause of chronic pancreatitis, has been a subject of intense debate in developing countries [27, 28]. However, in India, the intake of cassava has decreased over the past decade, even in areas where it constitutes a major component of the diet [29, 30]. The decline of cassava intake, and the intake of a more nutritious diet, when coupled with an increasing occurrence of smoking and alcoholism could have been factors contributing to the profile of chronic pancreatitis as described in our study. Nevertheless, 189 patients in this study did consume cassava. However, in the absence of a control group, the data are insufficient to implicate cassava as a risk factor for chronic pancreatitis.
In this study, 4% of the subjects had pancreatic adenocarcinoma. This proportion is comparable to that associated with alcoholic chronic pancreatitis worldwide, but much lower than the previously described rate of adenocarcinoma complicating tropical pancreatitis [22, 23]. The true incidence and prevalence of adenocarcinoma complicating chronic pancreatitis in India may be known only after prospective follow-up studies. This study also documents the clinical profile of chronic pancreatitis-related diabetes. Diabetes was present in 40% of the subjects. Nearly half of these subjects were controlled by diet and/or oral hypoglycemic agents, whereas half required insulin. Interestingly, our study showed that alcoholism was a factor associated with diabetes in subjects with chronic pancreatitis. Our study also showed that females (who were non-alcoholic) had a higher risk of developing diabetes as compared with non-alcoholic males. Thus, female gender and alcohol intake could both, by hitherto undefined mechanisms, be etiologically associated with the occurrence of diabetes in subjects with chronic pancreatitis. This study has several strengths and weaknesses. Obvious strengths include the reasonable sample size, the use of a welldefined online proforma and the prospective nature of the study. Limitations include occasionally missing data and the lack of information regarding diet and nutrient intake. In addition, the lack of a ‘not done’ option for endoscopic procedures and surgery means that there may have been some understatement of data regarding these procedures.
Despite the limitations, the study is the first example of a fully online, nationwide, prospective, multicenter disease registry from the Indian subcontinent. This study assumes importance in the light of a previous report suggesting a high prevalence of chronic pancreatitis in India [31]. It had been hypothesized earlier that the spectrum of chronic pancreatitis might be changing in the Indian subcontinent [29]. This study confirms the changing profile of chronic pancreatitis in this region, and especially records the decline of tropical chronic pancreatitis in its classical form.
Conflict of interest
The authors have no potential conflicts of interest
References
- Zuidema PJ. Cirrhosis and disseminated calcification of the pancreas in patients with malnutrition. Trop Geogr Med 1959; 11:70-4 [PMID 13659585]
- GeeVarghese PJ, Pillai VK, Joseph MP, Pitchumoni CS. The diagnosis of pancreatogenous diabetes mellitus. J Assoc Physicians India 1962; 10:173-78.
- Shaper AG. Chronic pancreatic disease and protein malnutrition. Lancet 1960;1:1223-4. [PMID 14445497]
- Chandak GR, Idris MM, Reddy DN, Mani KR, Bhaskar S, Rao GV, Singh L. Absence of PRSS1 mutations and association of SPINK1 trypsin inhibitor mutations in hereditary and non-hereditary chronic pancreatitis. Gut 2004; 53:723-8. [PMID 15082592]
- Geevarghese PJ. Pancreatic diabetes. A clinicopathological study of growth onset diabetes with pancreatic calculi. Popular Prakashan, Bombay, 1968.
- Viswanathan M, Sampath KS, Subramanyam S, Krishnaswami CV. Etiopathological and clinical angle of pancreatic diabetes from Madras. J Assoc Physicians India 1973; 21:753-9. [PMID 4604446]
- Kaushik SP, Vohra R, Varma R. Spectrum of pancreatitis at Chandigarh. A ten years experience. Indian J Gastroenterol 1983; 2:9-11. [PMID 6565638]
- Shah SC. Chronic pancreatitis - Follow up of operated cases. Indian J Gastroenterol 1986; 3:157-9. [PMID 3744443]
- Mohan V, Mohan R, Susheela L, Snehalatha C, Bharani G, Mahajan VK, et al. Tropical pancreatic diabetes in South India. Heterogeneity in clinical and biochemical profile. Diabetologia 1985; 28:229-32. [PMID 4018450]
- Balakrishnan V. Chronic calcific pancreatitis in the Tropics. Indian J Gastroenterol 1984; 3:65-7. [PMID 6565646]
- Rakesh Tandon, Rai PR, Nundy S, Vashist S. A study of chronic pancreatitis at the All India Institute of Medical Sciences, New Delhi. In: Chronic pancreatitis in India. Ed. Balakrishnan V. Pub Indian Society of Gastroenterology 1987. St Joseph's Press, Trivandrum, India (1st Edn).
- Tripathy BB, Samal KC, Mishra H. Diabetes with Exocrine pancreatic diseases. In: Diabetes mellitus in developing countries. Edr: Bajaj JS, Madan R, Shah AK, Mohan N. New Delhi: Interprint 1984.
- Website of the Indian Pancreatitis Study Group. www.ipans.org. Accessed on 5th June, 2008.
- Etemad B, Whitcomb DC. Chronic pancreatitis: Diagnosis, classification and new genetic developments. Gastroenterology 2001; 120-682-707. [PMID 11179244]
- Balakrishnan V. Tropical Pancreatitis - epidemiology, pathogenesis and etiology. In: Balakrishnan V, Ed. Chronic pancreatitis in India. Indian Society of Pancreatology, Trivandrum 1987; 79- 85.
- Balakrishnan V. Pancreatic tropicale. In: Bernades P, Hugier M. Eds. Progress en Hepatogastroenterologie: Maladies Du Pancreas Exocrine. Paris: Doin editeurs 1987; 207-27.
- Mohan V, Premalatha G. Fibrocalculous pancreatic diabetes. Int J Diabetes 1995; 3:71-82.
- Balakrishnan V, Lakshmi R, Nandakumar R. Tropical pancreatitis - what is happening to it? In: Chronic Pancreatitis and Pancreatic Diabetes in India. Eds: Balakrishnan V, Harish Kumar, Sudhindran S, Unnikrishnan AG. Cochin: Indian Pancreatitis Study Group 2006; 23 -54.
- Mohan V, Nagalotimath SJ, Yajnik CS, Tripathy BB. Fibrocalculous Pancreatic Diabetes. Diabetes Metab Rev 1998; 14:153-70. [PMID 9679668]
- The Hoax of God's Own Country. Outlook Magazine 2004; 12:53.
- Das SK, Balakrishnan V, Vasudevan DM. Alcohol: its health and social impact in India. Natl Med J India 2006; 19:94-9. [PMID 16756199]
- Chari ST, Mohan V, Pitchumoni CS, Viswanathan M, Madanagopalan N, Lowenfels AB. Risk of Pancreatic Carcinoma in tropical calcifying pancreatitis: an epidemiologic study. Pancreas 1994; 2:62. [PMID 8108373]
- Mori M, Hariharan M, Anandakumar M, Tsutsumi M, Ishikawa O, Konishi Y, et al. A case control study on the risk factors for pancreatic diseases in Kerala, India. HepatoGastroenterology 1999; 46:25-30 [PMID 10228760]
- Lin Y, Tamakoshi A, Hayakawa T, Ogawa M, Ohno Y. Cigarette smoking as a risk factor for chronic pancreatitis: a case-control study in Japan. Research Committee on Intractable Pancreatic Diseases. Pancreas 2000; 21:109-14. [PMID 10975702]
- Pradeepkumar AS, Mohan S, Gopalakrishnan P, Sarma PS, Thankappan KR, Nichter M. Tobacco use in Kerala. Findings from three recent studies. Natl Med J India 2005; 18:148-53. [PMID 16130619]
- Rani M, Bonu S, Jha P, Nguyen SN, Jamjour L. Tobacco use in India: Prevalence and predictors of smoking and chewing in a national cross sectional household survey. Tob Control 2003;12:e4. [PMID 14660785]
- Geevarghese PJ. Calcific Pancreatitis. Bombay: Varghese Publishing House 1986.
- Narendranathan M, Cheriyan A. Lack of association between cassava consumption and tropical pancreatitis syndrome. J Gastroenterol Hepatol 1994; 9:282-5 [PMID 8054529]
- Balakrishnan V, Nair P, Radhakrishnan L, Narayanan VA. Tropical pancreatitis - a distinct entity, or merely a type of chronic pancreatitis? Indian J Gastroenterol 2006, 25; 74-81. [PMID 16763335]
- Ramasundaram P, Lakshmi Kr, Anantharaman M. Changing scenario of cassava in Kerala economy. International Symposium on Tropical Tuber Crops - Problems, Prospects and Future Strategies. Trivandrum: Central Tuber Crops Research Institute. 1993:69.
- Garg PK, Tandon RK. Survey on chronic pancreatitis in the Asia-Pacific region. J Gastroenterol Hepatol 2004; 19:998-1004. [PMID 15304116]


