Ragesh Babu Thandassery1, Sathish Kumar Raamya Mothilal2, Shrawan Kumar Singh2, Abdul Khaliq1, Lalan Kumar1, Rashi Kochhar1, Kartar Singh1 and Rakesh Kochhar1
Departments of 1Gastroenterology and 2Urology,
Postgraduate Institute of Medical Education and Research. Chandigarh, India
- *Corresponding Author:
- Rakesh Kochhar
Department of Gastroenterology; Postgraduate Institute of Medical
Education and Research; Chandigarh-160012; India
Phone: +91-172.275.6617; +91-172.275.6608
Fax: +91-172.274.4401
E-mail: dr_kochhar@hotmail.com
Received June 29th, 2011 - Accepted August 15th, 2011
Keywords
Pancreatic Fistula; Pancreatic Pseudocyst; Pancreatitis, Alcoholic; Pancreatitis, Chronic
INTRODUCTION
Acute or chronic inflammation of the pancreas can result in the development of a pseudocyst in the pancreas or in the surrounding non-pancreatic tissues [1, 2]. Pancreatic pseudocysts are organized nonepithelized fluid collections in the context of acute or chronic pancreatitis, and have been described in virtually every organ of the body depending upon where the activated pancreatic enzymes are released and what path the enzymatic digestion takes [3]. Although there is controversy over the nomenclature, a pancreatic abscess is a circumscribed intra-abdominal collection of pus, mostly occurring in relation to the pancreas, containing little or no pancreatic necrosis and arising after infection of the pseudocyst [4]. Pseudocysts at atypical locations such as the spleen, liver, mediastinum, pelvis and kidney have rarely been reported [5, 6, 7, 8, 9, 10, 11, 12]. They may occur in unusual locations through the spread of the pancreatic enzymes along the intra-abdominal fat planes. Pseudocysts at atypical locations pose a unique and difficult diagnostic as well as therapeutic challenge, even more so when they present as abscesses. We report an unusual presentation of a pancreatic pseudocyst in a patient who presented with a left perinephric abscess.
CASE REPORT
A 25-year-old male presented with a two-month history of dull pain in the left loin which had worsened in severity in the preceding two weeks. He also had the sensation of a lump in the left loin and a low grade fever of two months duration. He denied any history of weight loss or vomiting, or any luminal or urinary symptoms. He was a chronic alcohol abuser, consumed about 500 mL of alcoholic beverages daily for the preceding 8 years. He was initially evaluated in a peripheral hospital where he underwent an ultrasound of the abdomen which showed a left perinephric abscess for which he was referred to the Department of Urology at our hospital.
On evaluation, he was febrile (39°C) and had an 8x8 cm tender ballotable lump in the upper left abdomen. Ultrasonography of the abdomen showed a 12x8 cm left perinephric collection, and a percutaneous pig-tail catheter drain was placed under ultrasound guidance. It drained 600 mL of purulent fluid for the first two days and, thereafter, about 100 mL of hazy fluid per day. A bacterial culture of the fluid isolated alpha hemolytic Streptococci sensitive to ampicillin and amino- glycosides, and he was started on parenteral amikacin. The pig-tail catheter drain continued to drain about 100 mL fluid per day for more than 7 days although his fever subsided. A routine urine examination and a bacterial urine culture did not reveal any evidence of infection. Blood sugar was normal and HIV serology was negative. Electrocardiography and echocardiography were also normal. In view of the persistent drain output, the fluid was further investigated; the amylase level in the fluid was found to be 2,566 U/L (reference range: 20-96 U/L) and the corresponding serum amylase was 76 U/L. Contrast-enhanced computerized tomography (CECT) of the abdomen was carried out which showed dense foci of calcification in the head of the pancreas, a mildly prominent pancreatic duct with a 12.3x8.6 cm hypodense collection in the posteroinferior part of the left kidney, displacing it anteriorly and eroding its posteroinferior capsule (Figure 1). There was no evidence of fluid collection anywhere else in the abdomen. A diagnosis of chronic calcific pancreatitis with a left perinephric abscess was made and a gastroenterological opinion was sought. His serum parathyroid hormone and triglyceride levels were normal. There were no signs of pancreatic exocrine or endocrine insufficiency. He underwent endoscopic retrograde cholangiopancreatography (ERCP) but selective pancreatic ductal cannulation could not be achieved, possibly because of the dense calcification. A needle knife sphincterotomy of the ampulla of Vater was carried out in the direction of the 1 o’clock position, from the ampullary orifice. The patient had a reduction in drain output following this procedure. On the 11th day, the drainage stopped completely; repeat ultrasonography showed no residual collection and the pig-tail catheter drain was removed. He was asymptomatic on discharge and a follow-up CECT scan one month later showed complete resolution of the perinephric abscess (Figure 2).
Figure 1. a. CECT abdomen showing calcification in the head of the pancreas and the left perinephric abscess. b. Coronal section showing the left
perinephric abscess.
Figure 2. a. CECT abdomen showing the percutaneous catheter drainage of the left perinephric abscess. b. Follow-up CECT showing resolution of
the perinephric abscess.
DISCUSSION
We have described a patient with a left perinephric abscess which had possibly occurred after an episode of acute pancreatitis. The elevated amylase level suggested underlying pancreatic pathology which was confirmed on CECT. Pancreatitis results in injury to the pancreatic acinar cells, and the release of the activated digestive enzymes, amylase and lipase. This leads to local pancreatic tissue destruction and pancreatic pseudocyst formation. Infected pseudocysts and abscesses develop as a consequence of infection of the pseudocyst and have similar treatment and outcome [4]. Drainage of the enzymes along anatomic fascial planes causes digestion of the surrounding tissues and results in non-pancreatic pseudocysts. Non-pancreatic pseudocysts have been reported to occur in the mediastinum, groin and spleen, and, infrequently, in the kidney [2, 5, 6, 7, 8, 9, 10, 11, 12]. Seepage of the pancreatic enzymes beneath Gerota’s fascia into the perirenal fatty tissues, and digestion of the perirenal fat by the pancreatic enzymes possibly results in renal pseudocyst formation. Only eight cases of renal pseudocyst formation due to pancreatitis have been reported (Table 1) [8, 13, 14, 15, 16, 17, 18, 19].
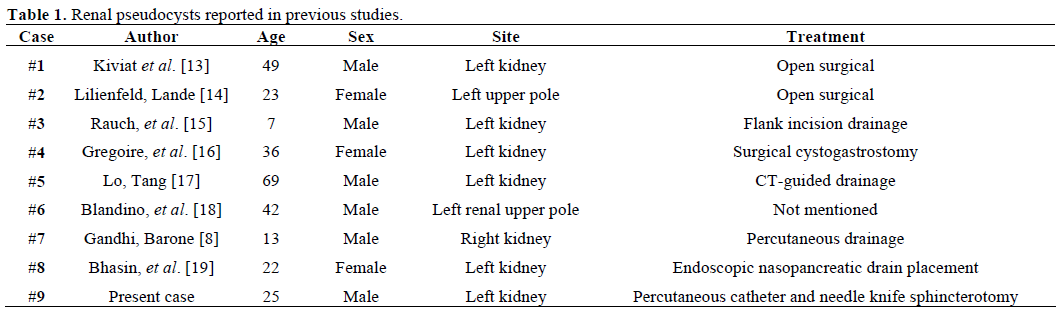
In most cases, renal pseudocysts involve the left kidney, and it has been suggested that the duodenal loop acts as an anatomic barrier for the right kidney (only one report) [8]. Renal pseudocyst formation should be suspected in cases of renal collections of uncertain etiology which are not resolved with conventional treatment methods. The diagnosis can be established with ultrasonography, CECT or magnetic resonance imaging. Treatment consists of cyst drainage (pig-tail catheter drain or surgery) and/or ERCP. In seven of the eight reported cases, this was accomplished with open surgical drainage [8, 13, 14, 15, 16, 17, 18]. There is only one previous case of a renal pseudocyst which was successfully treated with nasopancreatic drain placement [19]. In our case, an indwelling catheter had failed to show any resolution of the perinephric abscess. However, after needle knife sphincterotomy of the ampulla of Vater, the drainage gradually ceased. Endoscopic sphincterotomy alone has been shown to result in the resolution of pancreatic ascites as it results in obliteration of the high pressure gradient at the pancreatic sphincter which results in the preferential drainage of the pancreatic enzymes into the duodenum similar to the management of patients with bile leaks where obliteration of the transpapillary gradient alone is satisfactory [20, 21]. In all the reported cases of renal pseudocysts, including ours, significant clinical and radiographic improvement occurred after pseudocyst drainage, and recurrence was not reported in any case. Our case report represents the first report of a perinephric abscess in relation to chronic calcific pancreatitis and also only the second such case managed non operatively.
CONCLUSION
Renal pseudocyst and abscess formation should be considered in all patients with perinephric abscesses not responding to drainage. Endoscopic sphincterotomy alone can result in complete resolution of an abscess.
Conflict of interest
The authors have no potential conflicts of interest
References
- Gooding GAW. Pseudocysts of the pancreas with mediastinal extension. J ClinUltrasound 1977;5: 121-123. [PMID 404329]
- Salvo AF, Nematolahi H. Distant dissection of pancreatic pseudocyst into the groin. Am J Surg 1973; 126: 430-432. [PMID 4728934]
- Lehman GA. Pseudocysts. GastrointestEndosc 1999; 49:S81- S84. [PMID 10049456]
- Bollen TL, Besselink MG, van Santvoort HC, Gooszen HG, van Leeuwen MS. Toward an update of the atlanta classification on acute pancreatitis: review of new and abandoned terms. Pancreas 2007 Aug;35(2):107-13. [PMID 17632315]
- Bhasin DK, Rana SS, Chandail V, Nanda M, Nadkarni N, Sinha SK, Nagi B. Intrahepatic pancreatic pseudocyst successfully treated by endoscopic transpapillarynasopancreatic drainage alone. JOP. J Pancreas (Online) 2005; 6:593-597. [PMID 19915913]
- Bhasin DK, Rana SS, Chandail VS, Nanda M, Sinha SK, Nagi B. Successful resolution of a mediastinalpseudocyst and pancreatic pleural effusion by endoscopic nasopancreatic drainage. JOP. J Pancreas (Online) 2005; 6:359-364. [PMID 16006688]
- Bhasin DK, Udawat HP, Rana SS, Sood AK, Sinha SK, Nagi B. Intra-splenic pancreatic abscess successfully treated by endoscopic transpapillary drainage through the minor papilla. Gastrointest 2005; Endosc 62:192-194. [PMID 15990853]
- Gandhi M, Barone JG. Pediatric renal pseudocyst due to pancreatitis. Urology 2006; 68:1344 e5-1344 e6. [PMID 17169661]
- Topa L, La´szlo´ F, Sahin P, Pozsa´r J. Endoscopic transgastric drainage of a pancreatic pseudocyst with mediastinal and cervical extensions. GastrointestEndosc 2006; 64:460-463. [PMID 16923506]
- Balzan S, Kianmanesh R, Farges O, Sauvanet A, O'Toole D, Levy P, Ruszniewski P, Ogata S, Belghiti J. Right intrahepatic pseudocyst following acute pancreatitis: an unusual location after acute pancreatitis. J HepatobiliaryPancreatSurg 2005; 12:135-137. [PMID 15868077]
- Gupta R, Munoz JC, Garg P, Masri G, Nahman NS Jr, Lambiase LR. Mediastinal pancreatic pseudocyst- a case report and review of the literature. MedGenMed 2007; 9:8. [PMID 17955064]
- Shenoy P, Ganesan P, Swaminathan RP. Systemic hypertension due to compression of the kidney by a pancreatic pseudocyst. Eur J Intern Med 2007; 18:507-508. [PMID 17822666]
- Kiviat M, Miller E, and Ansell J. Pseudocysts of the pancreas presenting as renal mass lesions. Br J Urol 1971; 43: 237-262. [PMID 5556866]
- Lilienfeld R, Lande A. Pancreatic pseudocysts presenting as thick walled renal and perinephric cysts. J Urol 1976; 115:123-125. [PMID 1249862]
- Rauch R, Korobkin M, and Silverman P. Subcapsular pancreatic pseudocyst of the kidney. J Comput Assist Tomogr 1983; 7: 536-538. [PMID 7560337]
- Gregoire M, Rosenberg L, Haegert D, et al. Pancreatic pseudocyst rupture into the renal collecting system. Pancreas 1989; 4: 751-754. [PMID 2813334]
- Lo J, Tang S. CT of multiple subcapsularpseudocysts of the kidney complicating acute pancreatitis. J Comput Assist Tomogr 1995; 19: 823-824. [PMID 7560337]
- Blandino A, Scribano E, Aloisi G, et al. Subcapsular spread of a pancreatic pseudocyst. AbdominImag 1996; 21: 73-74. [PMID 7560337]
- Bhasin DK, Rana SS, Nanda M, Chandail V, Massodi I ,Kang M, Kalra N, Sinha SK, Nagi B, Singh K. Endoscopic management of pancreatic pseudocysts at atypical locations. SurgEndosc 2010; 24:1085-1091. [PMID 19915913]
- Bhasin DK, Malhi NS, Nagi B, Singh K. Pancreatic ascites treated by endoscopic pancreatic sphincterotomy alone: A case report. GastrointestEndosc 2003; 5 (6): 802-804. [PMID 12739571]
- Bjorkman DJ, Carr-Locke DL, Lichtenstein DR, Ferrari AP, Slivka A, Van Dam J, et al. Postsurgical bile leaks: endoscopic obliteration of transpapillary gradient is enough. Am J Gastroenterol 1995;90:2128-33. [PMID 8540501]



