Preethi John1, Kathleen McConnell2, Muhammad Wasif Saif1,2*
1Department of Internal Medicine and 2Division of Hematology and Oncology, Tufts Medical Center. Boston, MA, USA
- *Corresponding Author:
- Muhammad Wasif Saif
Department of Medicine and Cancer Center
Tufts Medical Center
800 Washington Street Box 245
Boston, MA 02111; USA
Phone +1-617.636.5627
Fax +1-617.636.8535
E-mail wsaif@tuftsmedicalcenter.org
Received: August 20th, 2013 Accepted: September 26th, 2013
Keywords
Anxiety; Depression; Pancreatic Neoplasms; Paroxetine; Tremor
Abbreviations
5-HT: serotonin; SNRI: serotonin and noradrenaline reuptake inhibitor; SSRI: selective serotonin reuptake inhibitor
INTRODUCTION
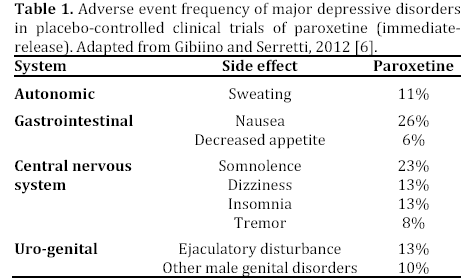
Mood disorders such as anxiety and depression are on the rise in this decade. According to the Centers for Disease Control and Prevention, about 30% of Americans will develop an anxiety disorder and about 17% will develop major depressive disorder [1]. Antidepressants were the third most common prescription drug taken by Americans of all ages in 2005-2008 [2]. It is the most common prescription drug taken by Americans between the ages of 18- 44. The rate of antidepressant use in the United States among all ages has increased almost 400% from 1988-1994 through 2005-2008 [2]. It is evident that these numbers will continue to increase as more people are diagnosed with mood disorders. The World Health Organization has estimated that depression will rival heart disease as the second most prevalent cause of illness-induced disability by the year 2020 [3]. Mood disorders are especially significant in the population of patients with cancer. One meta-analysis of 94 interviewbased studies showed that among patients with cancer, the pooled prevalence of Diagnostic and Statistical Manual of Mental Disorders-defined major depression was about 16% and the prevalence of anxiety disorders was about 10% [4]. Therefore, antidepressants and anti-anxiolytics are also being used in the cancer population. These medications rely on targeting the serotonin (5-HT) transporter. The selective serotonin reuptake inhibitors (SSRIs) account for about 80% of the antidepressants on the market [3]. The mechanism of action of SSRIs involves inhibiting 5-HT reuptake after it is released from the synapse, thereby prolonging the availability of serotonin in the synaptic gap. This allows repeated stimulation of the receptors of the recipient cell [3]. The success of SSRIs relies on the theory that major depressive disorder is a low serotonin state [5]. Other antidepressant drugs such as the serotonin and noradrenaline reuptake inhibitors (SNRIs) or the classic tricyclic antidepressant are used as well. However, SSRIs are better tolerated because of the absence of severe side effects compared with the tricyclic drugs [3]. However, SSRIs still have an extensive side effect profile. Since it is increasingly used among cancer patients it is imperative to be aware of its toxicities (Table 1).
We now describe a case of a patient who developed chin tremors within 2 weeks of treatment with paroxetine for anxiety. This report is clinically relevant as paroxetine remains one of the most commonly used SSRIs for treatment of anxiety and depression.
CASE REPORT
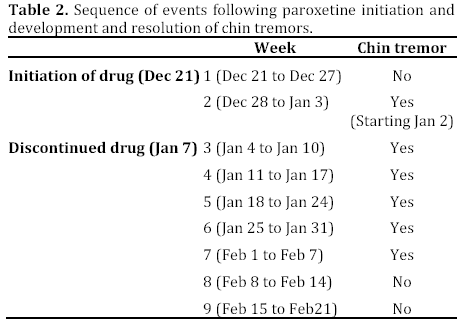
A 68-year-old Vietnamese female with a past medical history including GIST and pancreatic cancer status post Whipple procedure and six months of adjuvant chemotherapy with gemcitabine presented with symptoms of anxiety on cycle 1 day 15 of gemcitabine, which was December 21st, 2012. She reported difficulty sleeping which included waking up frequently through the night and therefore sleeping for two to three hours at a time. Prior to this, she would sleep about six hours straight through the night. She informed us that she was worried about her cancer. She was started on paroxetine 10 mg po once daily as well as lorazepam 1 mg po 1-2 tablets every six hours as needed. However, approximately 2 weeks after initiation of paroxetine, she developed a chin tremor. She noticed her chin and lower jaw were constantly shaking which resolved when she would sleep. She had no other tremors, headaches, dizziness, vision changes, slurred speech, confusion, lethargy, or any other neurologic complaints. On physical exam, she had a fine, constant tremor localized to the patient's entire chin and lower mandible with the axis being horizontal. The tremor decreased slightly when she smiled, puffed out her cheeks, spoke, or drank water. The tremor stopped when she clenched her teeth or opened her jaw wide. There were no focal motor or sensory deficits noted. Her cranial nerves were intact, deep tendon reflexes were symmetric in all extremities and her coordination was intact. There were no extremity tremors or rigidity seen on exam. Her vital signs were within normal limits. She does not have a history of essential tremors or Parkinson’s disease and neither does her family. Her labs were significant for stable anemia and a low absolute neutrophil count of 1,400 cells/μL likely secondary to bone marrow suppression from chemotherapy. Electrolytes were significant for hyponatremia with Na of 133 mEq/L (reference range: 137-142 mEq/L) in the setting of decreased oral intake. Therefore, cycle 2 day 2 of gemcitabine was held and paroxetine was discontinued. She did continue taking lorazepam as needed for insomnia. However, the tremor persisted despite delaying gemcitabine. At this time, it was hypothesized that her symptoms could be secondary to early-Parkinsonism, somatization from anxiety, or a side effect of paroxetine. She was seen by a neuro-oncology specialist and was found to have no neurological deficits and it was suggested that her symptoms are likely related to paroxetine. Her WBC and absolute neutrophil count improved and she was given day eight of cycle two five days late and gemcitabine was no longer held. By week 7, patient reported her chin tremors had been decreasing in frequency to only once per week. By week 8, her symptoms had completely resolved and it has not recurred since. She was continued on lorazepam for anxiety with improvement in anxiety symptoms. Please refer to Table 2 for sequence of events.
DISCUSSION
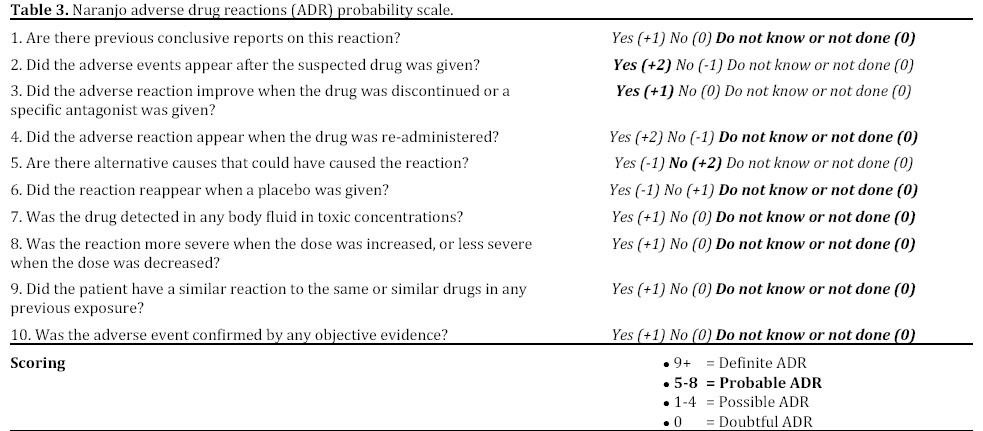
Paroxetine, a widely used SSRI has many side effects that have been extensively studied in the medical literature. However, there is limited data regarding the relationship between chin tremors and paroxetine. To our knowledge, this is the first case report of chin tremors as a side effect of paroxetine. There are web reviews showing rare cases of patients experiencing chin tremors while taking paroxetine. Based on the Naranjo adverse drug reactions probability scale there is a probable adverse reaction of chin tremors secondary to the use of paroxetine (Table 3).
The exact pathophysiology of chin tremors due to paroxetine remains unclear. There have been several proposed mechanisms for similar movement disorders caused by paroxetine. There are case reports of paroxetine causing akathisia-like movement disorders such as bruxism. The mechanism behind these movement disorders was suggested to be secondary to elevated levels of serotonin (5-HT) inhibiting central dopamine activity [7]. Paroxetine functions by inhibiting the pre-synaptic re-uptake of 5-HT resulting in elevated levels of 5-HT [8]. It has been hypothesized that elevated levels of 5-HT cause an increased serotonergic effect on the meso-cortical neurons from the ventral tegmental area leading to decreased dopamine levels. Since the meso-cortical tract is responsible for motor activity, a deficit of dopamine leads to movement disorders such akathisia-like jaw movements [7]. Other SSRIs such as citalopram have been reported to cause jaw tremors that were also suggested to be secondary to a decrease in central dopamine levels [9]. Further research is necessary to better delineate the relationship between jaw movement disorders and SSRIs so the appropriate symptomatic treatment can be determined.
The incidence of side effects of SSRIs is increasing with time as more patients are exposed to the drug. Therefore the side effect profile of SSRIs reported in clinical trials is not necessarily reflective of what patient’s experience [10]. There may be many other unreported cases of chin/jaw tremors and other movement disorders secondary to SSRIs that are affecting patient’s quality of life. Therefore, it is imperative that physicians treating depression or anxiety with SSRIs are aware of this side effect in order to prevent adverse outcomes. Our report is the first to establish the side effect of chin tremors in relation to paroxetine.
Conflicts of interest and source of funding
None declared
References
- National Center for Health Statistics (US). Health, United States, 2010: With Special Feature on Death and Dying. Hyattsville (MD): National Center for Health Statistics (US); 2011 Feb. PMID: 21634072
- Pratt LA, Brody DJ, Gu Q. Antidepressant use in persons aged and over: United States, 2005-2008. NCHS Data Brief. 2011 Oct; (76):1-8. PMID: 22617183
- Celada P, Puig M, Amargós-Bosch M, Adell A, Artigas F. The therapeutic role of 5-HT1A and 5-HT2A receptors in depression. J Psychiatry Neurosci. 2004 Jul; 29(4):252-65. PMID: 15309042
- Mitchell AJ, Chan M, Bhatti H, Halton M, Grassi L, Johansen C, Meader N. Prevalence of depression, anxiety, and adjustment disorder in oncological, haematological, and palliative-care settings: a meta-analysis of 94 interview-based studies. Lancet Oncol. 2011 Feb; 12(2):160-74. PMID: 21251875
- Owens MJ, Nemeroff CB. Role of serotonin in the pathophysiology of depression: focus on the serotonin transporter. Clin Chem. 1994 Feb; 40(2):288-95. PMID: 7508830
- Gibiino S, Serretti A. Paroxetine for the treatment of depression: a critical update. Expert Opin Pharmacother. 2012 Feb; 13(3):421-31. PMID: 22263916
- Milanlioglu A. Paroxetine-induced severe sleep bruxism successfully treated with buspirone. Clinics (Sao Paulo). 2012; 67(2):191-2. PMID: 22358247
- Foster RH, Goa KL. Paroxetine : a review of its pharmacology and therapeutic potential in the management of panic disorder. CNS Drugs. 1997 Aug; 8(2):163-88. PMID: 23338224
- Tarlaci S. Citalopram-induced jaw tremor. Clin Neurol Neurosurg. 2004 Dec; 107(1):73-5. PMID: 15567557
- Ferguson JM. SSRI Antidepressant Medications: Adverse Effects and Tolerability. Prim Care Companion J Clin Psychiatry. 2001 Feb; 3(1):22-27. PMID: 15014625

