Keywords
Angiography; Celiac Artery; Hepatic Artery; Mesenteric Arteries; Pancreatectomy; Pancreaticoduodenectomy; Tomography; Spiral Computed
INTRODUCTION
According to the classic anatomic study of Michels [1], extensive angiographic, transplantation and CT angiography data [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17, 18] of celiaco-mesenteric arterial aberrations were described in 22-48% of observations. The preoperative knowledge of variant celiacomesenteric arterial anatomy is of great value in planning extended pancreatic and multiorgan resections, and the importance of such awareness is conditioned by the necessity of wide periaortic and periarterial dissection and extensive vessel skeletonization during extended pancreaticoduodenectomy and extended distal pancreatectomy. This knowledge also facilitates upper abdominal surgery and helps avoid iatrogenic injury when the organ relationship is changed, visualization is limited or when the organs are too susceptible to ischemia, even if temporary [19, 20, 21, 22, 23, 24, 25, 26]. Modern MDCT enables a rapid acquisition of thin-slice high-resolution images of abdominal arteries during the phase of maximal contrast enhancement. Data processing during a routine CT examination allows 3D reconstructions to be immediately created, providing the surgeon with a 3D model of the patient’s arterial anatomy [18, 27, 28, 29, 30]. In this study, the capability of CT angiography to identify celiac and mesenteric arterial anatomy aberrations were analyzed by comparing the CT angiograms with the pictures of the operative field.
MATERIALS AND METHODS
CT Angiography
In order to pre-surgically estimate individual vascular trees, 3D reformations of axial MDCT scans in the arterial phase of bolus contrast enhancement were used. A bolus of 100 mL of a contrast medium (350 mg/mL of iodine) followed by 50 mL of saline solution was administered into the antecubital vein by the power injector. The arterial MDCT acquisition phase starts in the 10th second after achieving 150 HU threshold attenuation of the abdominal aorta.
A CT angiography database from July 2008 to February 2010 included 378 consecutive CT angiograms of 350 patients, all of whom were examined on 64- and 256-MDCT scanners (Brillians- 64® and Brillians iCT®, Philips, Cleveland, OH, USA) for pancreatic or hepatobiliary malignant and nonmalignant conditions. Each patient was included only once in the study. CT was performed to establish the diagnosis, determine tumor resectability in case of malignancy and to aid surgical planning. Threedimensional reconstructions of CT angiograms were received using the software involved during a routine CT examination. All the CT angiographic images were read by the attending surgeon, and the variants of celiac and mesenteric arterial anatomy were recorded according to Michels’ [1] and Hiatt’s [10] criteria.
Procedure
A standard pancreaticoduodenectomy includes the removal of lymph nodes of the anterior and posterior pancreatoduodenal, pyloric, hepatoduodenal ligament, and superior and inferior pancreatic head and body lymph node stations.
An extended pancreaticoduodenectomy in our institution consists of the additional removal of all the lymph nodes from the hepatic hilum, along the aorta from the diaphragmatic hiatus to the inferior mesenteric artery and laterally to both the renal hila, clearance of the circumference of the origin of the celiac trunk and the superior mesenteric artery with total resection of the nerve plexus around the superior mesenteric artery and portal vein. The procedure includes removal of perivascular lymphatics and nerves and retroperitoneal connective tissue.
An extended distal pancreatectomy, which we usually perform “from the right to the left”, consists of removal of the spleen, pancreatic neck, body and tail with the splenic vessels, all the lymph nodes from the hepatic hilum, along the aorta from the diaphragmatic hiatus to the inferior mesenteric artery, clearance of the circumference of the origin of the celiac trunk and the superior mesenteric artery with the resection of the nerve plexus to the left and to the right of the superior mesenteric artery. The procedure includes removal of perivascular lymphatics and nerves and retroperitoneal connective tissue. If malignancy is suspected during frozen section examination of the posterior border of the specimen, a left adrenalectomy with periglandular tissue is performed.
Over the same period of time, 59 patients with pancreatic neoplasms underwent extended pancreaticoduodenectomy, extended distal pancreatectomy or multi-organ resections for pancreatic ductal adenocarcinoma (53 patients), intraductal papillary mucinous carcinoma (3 patients) and endocrine carcinoma (3 patients). After finishing the vessel dissection, operative fields were photographed and compared to CT angiogram at a later stage. Assessing and comparing the data, we regarded such a pattern as a "trifurcation" (division of the common hepatic artery into gastroduodenal, right and left hepatic arteries) and some other types not included in Michels’ classification, such as a subtype of the classic anatomy.
ETHICS
Our institutional review board approved this prospective review and special patient informed consent, other than standard consent for the operation, was not required.
STATISTICS
Descriptive statistics were applied: absolute and relative frequencies.
RESULTS
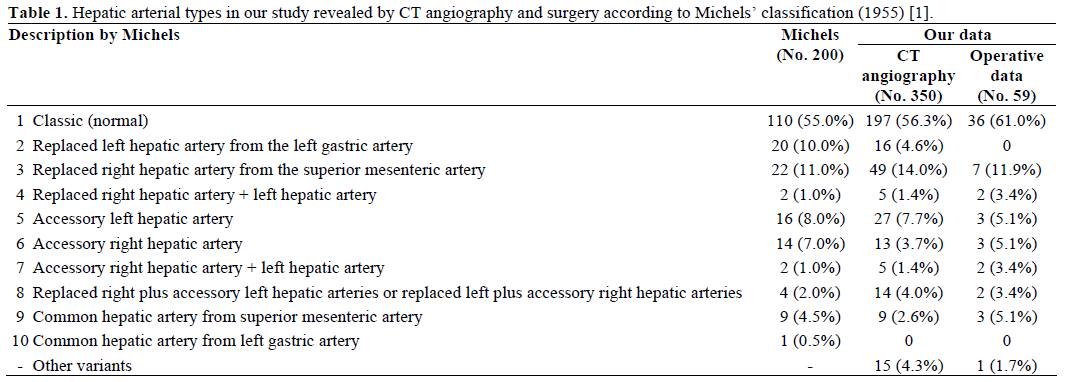
All CT angiographic studies were considered to be of diagnostic quality. One hundred and ninety-seven out of the 350 patients (56.3%) had the classic arterial anatomy identified at CT angiography (Figure 1). The most common variant identified was a replaced right hepatic artery originating from the superior mesenteric artery, seen in 49 patients (14.0%) (Figure 2). The second most common variant was an accessory left hepatic artery originating from the left gastric artery, seen in 23 patients (6.6%). One hundred and thirty-one patients (37.4%) had a single arterial aberration, and 22 patients (6.3%) showed more than one arterial variant (Figure 3). Variations in the origin of the common hepatic artery were seen in 18 patients (5.1%): the common hepatic artery originated from the superior mesenteric artery in 9 patients (2.6%) (Figure 4) and the common hepatic artery originated from the abdominal aorta in 9 patients (2.6%) (Figure 5). An accessory right hepatic artery, originating from the celiac axis or the superior mesenteric artery was seen in 13 patients (3.7%) and originating from the aorta in one patient (0.3%). A left gastric artery originating from the aorta was identified in 3 patients (0.9%) and a left hepatic artery originating from the aorta was seen in one patient (0.3%). Different combinations of accessory hepatic arteries were identified in 45 patients (12.9%) (Figure 6). The frequencies of the different types of arterial variants identified are reported and compared with the data of other studies in Tables 1 and 2. An example describing the importance of preoperative knowledge of the arterial architecture is shown in Figures 6 and 7; in a typical operative situation, after skeletonization of the hepatoduodenal ligament, the surgeon often finds a large artery to the right of the portal vein (Figure 6) and usually he or she has no idea what it is, where it comes from and where it is going. As is seen from the CT angiography in Figure 7 which corresponds to the operative pictures, the origin and destination of these arteries are very different.
Figure 1.Michels’ type I (classic) celiaco-mesenterial anatomy in а
47-year-old man with neuroendocrine carcinoma of the pancreatic
head. a. 3D CT angiographic image after the removal of the renal
artery image. b. View of the operating field after the extended
pancreaticoduodenectomy.
CHA: common hepatic artery; CT: celiac trunk; GDA:
gastroduodenal artery; IVC: inferior vena cava; LGA: left gastric
artery; LHA: left hepatic artery; PS: pancreatic stump; PV: portal
vein; RHA: right hepatic artery; SA: splenic artery; SMA: superior
mesenteric artery
Figure 2. Michels’ type III anatomy in a 75-year-old woman with
pancreatic head adenocarcinoma. Replaced right hepatic artery
(rRHA) originating from the superior mesenteric artery (SMA). a. 3D
CT angiographic image after the removal of the renal artery image. b. View of the operating field after extended pancreaticoduodenectomy.
CT: celiac trunk; IVC: inferior vena cava; LHA: left hepatic arteries;
PV: portal vein; PS: pancreatic stump; SA: splenic artery
Figure 3. Michels’ type IV anatomy in a 53-year-old woman with
pancreatic head and body cystadenocarcinoma. Replaced right
hepatic artery (rRHA) originating from the superior mesenteric artery
(SMA) and replaced left hepatic artery (rLHA) originating from the
left gastric artery (LGA). a. 3D CT angiographic image after the
removal of the renal artery image. b. View of the operating field after
pancreaticoduodenectomy and pancreatic body resection.
GDA: gastroduodenal artery; PS: pancreatic stump; PV: portal vein;
SA: splenic artery
Figure 4. Michels’ type IX (Hiatt’s type V) anatomy in a 56-year-old
man with pancreatic head adenocarcinoma. Replaced common
hepatic artery (CHA) arising from the superior mesenteric artery
(SMA). a. 3D CT angiographic image after the removal of the renal
artery image. b. View of the operating field after extended
pancreaticoduodenectomy.
aRHA: accessory right hepatic artery; CT: celiac trunk; GDA:
gastroduodenal artery; LHA: left hepatic artery; PS: pancreatic
stump; PV: portal vein; RHA: right hepatic artery; SA: splenic artery
Figure 5. Unclassified by Michels, Hiatt’s type X anatomy in a 63-
year-old man with pancreatic head adenocarcinoma. Replaced
common hepatic artery (CHA) arising from the aorta. a. 3D CT
angiographic image after the removal of the renal artery image. b. View of the operating field after pancreaticoduodenectomy.
CT: celiac trunk; IVC: inferior vena cava; PS: pancreatic stump; PV:
portal vein; SMA: superior mesenteric artery
Figure 6. Views of the operating fields after the skeletonization of the hepatoduodenal ligament during pancreaticoduodenectomy. The surgeon
discovers a large artery to the right of the portal vein which has a different origin in all three cases.
aRHA: accessory right hepatic artery; GDA: gastroduodenal artery; LHA: left hepatic artery; PHA: proper hepatic artery; PV: portal vein; RHA: right
hepatic artery; rRHA: replaced right hepatic artery
Figure 7. 3D CT angiographic image after the removal of the renal artery
image. a. Michels’ type VIII anatomy in a 47-year-old man with
pancreatic head adenocarcinoma. Replaced right hepatic artery (rRHA)
originating from the superior mesenteric artery (SMA) and accessory left
hepatic artery (aLHA) originating from the left gastric artery. b. Michels’
type VII anatomy in a 63-year-old woman with pancreatic head
adenocarcinoma. Accessory right hepatic artery (aRHA) originating from
the celiac trunk. c. Michels’ type IV anatomy. Right hepatic artery (RHA)
originating from the celiac trunk (CT) and replaced left hepatic artery
(LHA) originating from the superior mesenteric artery (SMA).
CHA: common hepatic artery; GDA: gastroduodenal artery, RGEA: right
gastro-epiploic artery; RHA: right hepatic artery
Celiac axis compression syndrome in 7 cases (2.0%) and atherosclerotic stenoses and obstructions of celiac and mesenteric arteries in 19 cases (5.4%) were indentified on CT angiography. Only one situation was clinically meaningful and required celiac trunk stenting (Figure 8) before a distal pancreatectomy. Five patients (1.4%) with non-malignant pancreatic lesions and 8 patients (2.3%) with miscellaneous liver diseases associated with celiac and mesenterial artery stenoses were operated on without additional procedures on the visceral arteries.
Figure 8. 3D CT angiographic image after the removal of the renal artery image in a 64-year-old woman with chronic pancreatitis and suspected
pancreatic head adenocarcinoma. a. Celiac trunk (CT) stenosis and superior mesenteric artery (SMA) occlusion b. Upper abdomen blood supply from
the minor pelvis through the arcade of Riolan. In the case of inadvertent damage of this arcade during abdominal surgery, notable intestinal necrosis
is possible which necessitates celiac trunk stenting as a first stage procedure. c. d. Changes in functioning arterial collaterals after celiac trunk
stenting. Arcade of Riolan is not defined and powerful hepatic arteries are visible.
aRHA: accessory right hepatic artery; CHA: common hepatic artery; GDA: gastroduodenal artery; SA: splenic artery
Aneurysms of celiac and mesenteric arterial branches were seen in 11 cases (3.1%). All the lesions except one (Figure 9) were associated with chronic pancreatitis, confirmed at surgery or angiography, and treated by embolization or surgically.
Figure 9. 3D CT angiographic image after the removal of the renal
artery image in a 39-year-old man with pancreatic head
adenocarcinoma. a. Left gastric artery (LGA) originating from the
aorta with the aneurysm in its proximal part. b. View of the operating
field during pancreaticoduodenectomy. The aneurysm was dissected
away from the surrounding tissue and excised with the trunk of the
left gastric artery.
A: aneurysm; CHA: common hepatic artery; SMA: superior
mesenteric artery
All operative pictures were considered descriptive. Thirty-six (61.0%) out of the 59 patients who underwent an extended pancreaticoduodenectomy or extended distal pancreatectomy had a classic celiacomesenteric anatomy. A replaced right hepatic artery originating from the superior mesenteric artery was seen in 7 (11.9%) patients. An accessory left hepatic artery originating from the left gastric artery, an accessory right hepatic artery originating from the celiac trunk or superior mesenteric artery and a common hepatic artery originating from the superior mesenteric artery (hepatomesenteric trunk) were encountered in 3 separate patients (5.1% each). Four patients (6.8%) had two arterial variants identified. Finally, in one case (1.7%), the left gastric and, in two cases (3.4%), the common hepatic artery originated from the aorta. We did not encounter an isolated replaced left hepatic artery in the surgical series. The frequencies of the arterial variant types identified are shown in Table 1.
According to a comparison of operative photographs and 3D CT angiography reconstructions, CT angiography demonstrated 100% accuracy in identifying celiaco-mesenterial anatomy variants. In 3 cases of hepatomesenteric trunk and in 7 cases of a replaced right hepatic artery in the operative series, there were no cases of arterial involvement by a tumor. In two patients who were not operated on, CT angiography showed the hepatomesenteric trunks to be encircled by a tumor on a background of liver metastases. Other cases of these aberrations found on CT angiography were in patients with liver and nonmalignant pancreatic lesions.
DISCUSSION
In different fields of surgery, knowledge of celiac and mesenteric arterial variants is of great significance [19, 20, 21]. During a standard pancreaticoduodenectomy, arterial anomalies can increase the operative complexity and necessitate extended procedures demanding wide tissue dissection around the aorta and its visceral branches, demonstrating that an awareness of the celiac and mesenteric arterial anatomy is vitally important [22, 23, 24, 25, 26].
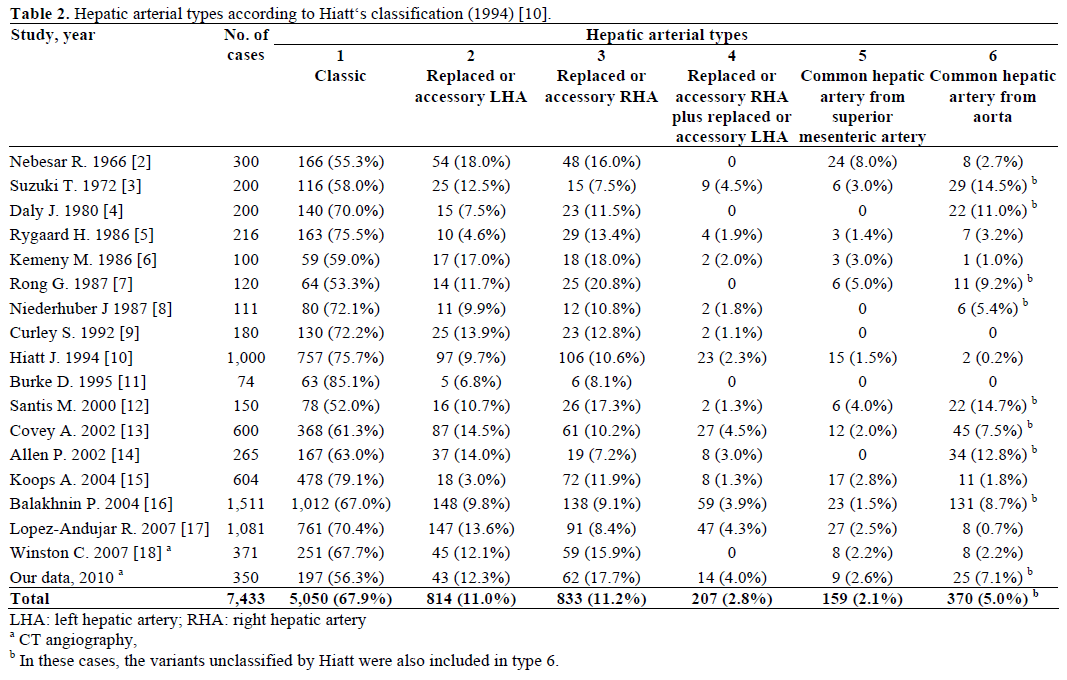
Michels’ classification of 1955, based on an autoptic series of 200 dissections [1], as well as Hiatt’s classification of 1994, based on 1,000 transplantations [10], are in general use in our institution for the description of celiac and mesenterial architecture. Because “… no two arterial vascularization patterns of any of the organs above the transverse colon are ever the same …” [1], Michels’ and Hiatt’s motivation was to “… maximize the database of the surgeon performing procedures in and around the porta hepatis, to avoid injury to vascular and ductal structures …” [10]. But this vast database cannot be used in each specific case exactly because of its size: “… It is obvious that no one mind can possibly remember all of the arterial variations that have been encountered in any given extensive investigation …” [1].
The current CT angiographic series (Table 1) shows almost the same incidence of variant patterns as was shown by Michels, except for a two-fold difference in the incidence between the accessorial left and the right hepatic arteries. We did not distinguish the common hepatic artery from the left gastric artery (Michels’ type 10); we distinguished the common hepatic artery from the aorta which was not described by Michels fairly often (9 cases, 2.6%). As compared to our results, more normal scheme patterns were revealed in the CT angiographic series published in 2007 by Winston et al., and no “doubled” aberrations were observed in that study [18].
Multidetector CT angiography is an effective tool not only for predicting tumor resectability [27, 28] but also for creating precise 3D reconstructions of the abdominal arteries during a routine CT examination in each specific case. It not only clearly delineates the course of the aberrant vessels, but also reveals the arterial stenoses and occlusions which may be critical if undiagnosed or if diagnosed during or after surgery [31, 32, 33, 34, 35, 36, 37, 38]. Knowledge of the vascular anatomy is of great value because the organ relationship is usually changed and direct visualization of the surgical field is often limited in patients with large pancreatic tumors, in “border-line resectable” cases, in obesity, prominent local inflammation after biliary stenting and dense adhesions after prior surgery [19, 20, 21, 22, 23, 24, 25, 26]. Preoperative knowledge of variant arterial anatomy may obviate extensive dissection to identify the vessels and avert vascular damage [22] or, vice versa, allows the surgeon to excise vessels infiltrated by a tumor knowing in advance that it is accessorial, thus avoiding an erroneous judgment about tumor unresectability [23]. The policy of our institution is not to operate on pancreatic cancer cases involving the arteries, except for the indications regarding the modified Appleby procedure. And then, we usually detect arterial involvement before surgery using CT and endoscopic ultrasound. Our thinking on the subject of local involvement of only the hepatomesenteric trunk or replaced right hepatic artery from the superior mesenteric artery by pancreatic cancer is “to resect and repair” if it does not originate from the superior mesenteric artery, but we did not encounter cases of isolated involvement of these arteries.
The most common variation in the hepatic arterial anatomy is the presence of a replaced right hepatic artery originating from the superior mesenteric artery. This has been reported to occur in 11-21% of patients [39]. In our series, the hepatomesenteric trunk and replaced right hepatic artery (10 cases) passed laterally behind the portal vein and behind or above the pancreatic head and entered the hepatoduodenal ligament posterolaterally to the bile duct. However, there have been reports of such vessels traveling behind or through the head of the pancreas in which case they are susceptible to damage [22, 40]. A replaced hepatomesenteric trunk and right hepatic artery should be recognized and preserved. Typically, we encircled the root of the superior mesenteric artery after an extensive Kocher’s maneuver. However, based on the experience presented in this series, it does not help much in preventing the hepatomesenteric trunk or replaced right hepatic artery from going above or behind the pancreatic head from an inadvertent injury, especially in the case of a large tumor. Since the origin of the hepatomesenteric trunk or replaced right hepatic artery is not close to the aorta where the superior mesenteric artery usually taped, you cannot keep these arteries in direct vision between the right side of the portal vein and superior mesenteric artery until after the uncinate process is in place. In our opinion, the most reliable technique, which we use as a standard, is the following: detection of the artery to the right of the portal vein and, after transection of all organs including the pancreatic neck, disclosure of the superior mesenteric artery behind the superior mesenteric vein, and meticulous detachment of the uncinate process ligament from the right surface of the superior mesenteric artery. In so doing, there is no chance of missing the origin of the hepatomesenteric trunk or replaced right hepatic artery or to accidentally injure their branches to the pancreas. After the origin of the aberrant vessel is detected, it is much easier to free the vessel from the surrounding tissue. Yet, irrespective of the technique used, whether the vascular architecture is discovered preoperatively, knowledge of the arterial anatomy helps in dealing with the aberrant vessel.
There were no arterial injuries during surgery in this series. It is hard to say whether or not it was due to the 3D CT angiography, as we are only now able to compare this series with the previous one of standard Whipple procedures retrospectively. However, 3D CT angiography makes the surgeon more confident when working in the perivascular and periaortal spaces.
The absence of visual surgical confirmation of radiological data is a limitation of the majority of stanndard or CT angiographic studies of the celiac and mesenteric arterial anatomy. A comparison of the operative and radiological pictures presented in our series shows that CT angiography is absolutely reliable for identifying arterial variants and arterial lesions while planning and performing extended pancreatic or other complex surgery in the upper abdomen.
Conflict of interest The authors have no potential conflict of interest
References
- Michels NA. Blood Supply and Anatomy of the Upper
Abdominal Organs with a Descriptive Atlas. Philadelphia, PA:
Lippincott, 1955.
- Nebesar RA, Kornblith PL, Pollard JJ, Michels NA. Celiac and
superior mesenteric artery a correlation of angiograms and
dissections. Boston, USA: Little, Brown and Co., 1969.
- Suzuki T, Nakayasu A, Kawabe K, Takeda H, Honjo I. Surgical
significance of anatomic variations of the hepatic artery. Am J Surg
1971; 122:505-12. [PMID 5098656]
- Daly JM, Kemeny N, Oderman P, Botet J. Long-term hepatic
arterial infusion chemotherapy. Anatomic considerations, operative
technique, and treatment morbidity. Arch Surg 1984; 119:936-41.
[PMID 6378147]
- Rygaard H, Forrest M, Mygind T, Baden H. Anatomic variants
of the hepatic arteries. Acta Radiol Diagn (Stockh) 1986; 27:425-7.
[PMID 3776676]
- Kemeny MM, Hogan JM, Goldberg DA, Lieu C, Beatty D,
Kokal WA, et al. Continuous hepatic artery infusion with an
implantable pump: problems with hepatic artery anomalies. Surgery
1986; 99:501-4. [PMID 3952672]
- Rong GH, Sindelar WF. Aberrant peripancreatic arterial
anatomy: consideration in performing pancreatectomy for malignant
neoplasms. Am Surg 1987; 53:726-9. [PMID 3425998]
- Niederhuber JE, Ensminger WD. Surgical consideration in the
management of hepatic neoplasia. Semin Oncol 1983; 10:135-47.
[PMID 6306833]s
- Curley SA, Chase JL, Roh MS, Hohn DC. Technical
consideration and complications associated with the placement of
180 implantable hepatic arterial infusion devices. Surgery 1993;
114:928-35. [PMID 8236017]
- Hiatt JR, Gabbay J, Busuttil RW. Surgical anatomy of the
hepatic arteries in 1000 cases. Ann Surg 1994; 220:50-2. [PMID
8024358]
- Burke D, Earlam S, Fordi C, Allen-Mersh TG. Effect of aberrant
hepatic arterial anatomy on tumor response to hepatic artery infusion
of floxuridine for colorectal liver metastases. Br J Surg 1995;
82:1098-100. [PMID 7648164]
- De Santis M, Ariost P, Cab GF, Romagnoli R. Hepatic arterial
vascular anatomy and its variants. Radiol Med 2000; 100:145-51.
[PMID 11148880]
- Covey AM, Brody LA, Maluccio MA, Getrajdman GI, Brown
KT. Variant hepatic arterial anatomy revisited: Digital subtraction
angiography performed in 600 patients. Radiology 2002, 224:542-7.
[PMID 12147854]
- Allen PJ, Stojadinovic A, Ben-Porat L, Gonen M, Kooby D,
Blumgart L, et al. The management of variant arterial anatomy
during hepatic arterial infusion pump placement. Ann Surg Oncol
2002; 9:875-80. [PMID 12417509]
- Koops A, Wojciechowski B, Broering DC, Adam G, Krupski-
Berdien G. Anatomic variations of the hepatic arteries in 604
selective celiac and superior mesenteric angiographies. Surg Radiol
Anat 2004; 26:239-44. [PMID 14968265]
- Balakhnin PV, Tarazov PG, Polykarpov PA, Suvorov YV,
Kozlov AV. Hepatic arteries anatomy according to 1511 angiograms.
Ann Surg Hepatol (Moscow) 2004; 9:14 -21.
- Lopez-Andujar R, Moya A, Montalva E, Berenguer M, De Juan
M, San Juan F, et al. Lessons learned from anatomic variants of the
hepatic artery in 1,081 transplanted livers. Liver Transpl 2007;
13:1401-4. [PMID 17902125]
- Winston CB, Lee NA, Jarnagin WR, Teitcher J, DeMatteo RP,
Fong Y, Blumgart LH. CT angiography for delineation of celiac and
superior mesenteric artery variants in patients undergoing
hepatobiliary and pancreatic surgery. AJR Am J Roentgenol 2007;
189:W13-9. [PMID 17579128]
- Redman HC, Reuter SR. Angiographic demonstration of
surgically important vascular variations. Surg Gynecol Obstet 1969;
129:33-9. [PMID 5790699]
- Thomas PG, Baer HU, Matthews JB, Gertsch P, Blumgart LH.
Post-operative hepatic necrosis due to reduction in hepatic arterial
blood flow during surgery for chronic biliary obstruction. Dig Surg
1990; 7:31-5.
- Fasel JH, Muster M, Gailloud P, Mentha G, Terrier F.
Duplicated hepatic artery: radiologic and surgical implications. Acta
Anat (Basel) 1996; 157:164-8. [PMID 9142340]
- Furukawa H, Shimada K, Iwata R, Moriyama N. A replaced
common hepatic artery running through the pancreatic parenchyma.
Surgery 2000; 127:711-2. [PMID 10840370]
- Yamamoto S, Kubota K, Rokkaku K, Nemoto T, Sakuma A.
Disposal of replaced common hepatic artery coursing within the
pancreas during pancreatoduodenectomy: report of a case. Surg
Today 2005; 35:984-7. [PMID 16249858]
- Yang SH, Yin YH, Jang JY, Lee SE, Chung JW, Suh KS, et al.
Assessment of hepatic arterial anatomy in keeping with preservation
of the vasculature while performing pancreatoduodenectomy: an
opinion. World J Surg 2007; 31:2384-91. [PMID 17922256]
- Yang F, Long J, Fu DL, Jin C, Yu XJ, Xu J, Ni QX. Aberrant
hepatic artery in patients undergoing pancreaticoduodenectomy.
Pancreatology 2008; 8:50-4. [PMID 18230918]
- Perwaiz A, Singh A, Singh T, Chaudhary A. Incidence and
management of arterial anomalies in patients undergoing
pancreaticoduodenectomy. JOP. J Pancreas (Online) 2010; 11:25-30.
[PMID 20065548]
- Brennan DD, Zamboni GA, Raptopoulos VD, Kruskal JB.
Comprehensive preoperative assessment of pancreatic
adenocarcinoma with 64-section volumetric CT. Radiographics
2007; 27:1653-66. [PMID 18025509]
- Zamboni GA, Kruskal JB, Vollmer CM, Baptista J, Callery MP,
Raptopoulos VD. Pancreatic adenocarcinoma: value of multidetector
CT angiography in preoperative evaluation. Radiology 2007;
245:770-8. [PMID 17951353]
- Winter TC 3rd, Nghiem HV, Freeny PC, Hommeyer SC, Mack
LA. Hepatic arterial anatomy: demonstration of normal supply and
vascular variants with three-dimensional CT angiography.
Radiographics 1995; 15:771-80. [PMID 7569128]
- Takahashi S, Murakami T, Takamura M, Kim T, Hori M,
Narumi Y, et al. Multi-detector row helical CT angiography of
hepatic vessels: depiction with dual-arterial phase acquisition during
single breath hold. Radiology 2002; 222:81-8. [PMID 11756709]
- Bull DA, Hunter GC, Crabtree TG, Bernhard VM, Putnam CW.
Hepatic ischemia, caused by celiac axis compression, complicating
pancreaticoduodenectomy. Ann Surg 1993; 217:244-7. [PMID
8095781]
- Berney T, Pretre R, Chassot G, Morel P. The role of
revascularization in celiac occlusion and pancreatoduodenectomy.
Am J Surg 1998; 176:352-6. [PMID 9817254]
- Manabe T, Baba N, Setoyama H, Ohshio G, Tobe T. Venous
bypass grafting for celiac occlusion in radical
pancreaticoduodenectomy. Pancreas 1991; 6:368-71. [PMID
1862070]
- Song SY, Chung JW, Kwon JW, Joh JH, Shin SJ, Kim HB, Park
JH. Collateral pathways in patients with celiac axis stenosis:
angiographic-spiral CT correlation. Radiographics 2002; 22:881-93.
[PMID 12110717]
- Hasegawa K, Imamura H, Akahane M, Miura Y, Takayama T,
Ohtomo K, Makuuchi M. Endovascular stenting for celiac axis
stenosis before pancreaticoduodenectomy. Surgery 2003; 133:440-2.
[PMID 12717363]
- Machado MC, Penteado S, Montagnini AL, Machado MA. An
alternative technique in the treatment of celiac axis stenosis
diagnosed during pancreaticoduodenectomy. HPB Surg 1998;
10:371-3. [PMID 9515234]
- Okamoto H, Suminaga Y, Toyama N, Konishi F, Kawahito H.
Autogenous vein graft from iliac artery to splenic artery for celiac
occlusion in pancreaticoduodenectomy. J Hepatobiliary Pancreat
Surg 2003; 10:109-12. [PMID 12918470]
- Ouaissi M, Verhelst R, Astarci P, El Khouri G, Hubert C, Van
Beers B, et al. Celiac artery occlusive disease: a rare but potentially
critical condition in patients undergoing pancreaticoduodenectomy.
Pancreatology 2009; 9:526.
- Shukla PJ, Barreto SG, Kulkarni A, Nagarajan G, Fingerhut A.
Vascular anomalies encountered during pancreatoduodenectomy: do
they influence outcomes? Ann Surg Oncol 2010; 17:186-93. [PMID
19838756]
- Biehl TR, Traverso LW, Hauptmann E, Ryan JA Jr. Preoperative
visceral angiography alters intraoperative strategy during the
Whipple procedure. Am J Surg 1993; 165:607-12. [PMID 8098185]










