Keywords
Pancreaticoduodenectomy; Pancreas
Abbreviations
o/s-SSIs organ/space surgical site infection; PD
pancreaticoduodenectomy
INTRODUCTION
Surgical site infection (SSI) after abdominal
gastrointestinal surgery extends hospital stay and
increases medical costs. Additionally, it has a negative
impact on not only patients but also hospital management
[1, 2, 3]. Therefore, techniques should be identified to
avoid and appropriately treat SSI.
Many studies have reported that a prophylactic drain
is not required for gastrointestinal surgery [4, 5], and
one study concluded that the drain was needed only at
esophagectomy and total gastrectomy [6]. However, other
studies have advocated the requirement of a prophylactic
drain in cases of pancreatic resection, including
pancreaticoduodenectomy (PD) [7, 8, 9]. Several studies
have reported that long-term dwelling of the drain can
cause pancreatic fistulas and increase the incidence of
organ/space SSIs (o/s-SSIs) [10, 11]. Because clinicians
often have the impression that complications such as o/s-
SSI and pancreatic fistulas would be more serious without
a drain than complications with a drain [7], these beliefs
may contradict the findings of many previous studies.
The present study analyzed the risk factors for o/s-
SSI after PD and examined the relationship between
prophylactic drain placement and the occurrence of o/s-
SSI according to the classification of microorganisms
detected in samples cultured from the drain at the time of
o/s SSI.
METHODS
A total of 97 consecutive patients who underwent
PD were considered for inclusion in this retrospective
study. However, four patients were excluded because of
lack of data. Therefore, 93 patients were finally enrolled
between 2001 and 2014. These patients were divided into
either the o/s-SSI-positive (o/s-SSI+) group, which had
a positive bacterial culture of the drainage fluid, or the
o/s-SSI-negative group (o/s-SSI−), which had a negative
bacterial culture of the fluid. The risk factors for o/s-SSI
were examined by comparing the following variables
between the two groups: age; sex; body mass index (BMI);
indication for operation; laboratory data at first visit,
including total bilirubin level, albumin level, hemoglobin
A1c (HbA1c) level, white blood cell (WBC) count, and
C-reactive protein (CRP) level; preoperative biliary stent
placement; American Society of Anesthesiologists physical
status (ASA-PS) classification; operation time; operative
blood loss; blood transfusion; quantity of peritoneal lavage
during operation; type of prophylactic drain used (open
or closed); duration of prophylactic drain placement;
duration of prophylactic antibiotic administration; and
pancreatic fistula development.
Additionally, by differentiating the bacteria detected
in the drainage fluid and by identifying the relationship
between the bacteria from the drainage fluid at the time of
o/s-SSI and the bacteria from bile samples obtained preor
intra-operatively, we determined whether the causative
bacteria of o/s-SSI were present in the abdominal cavity or
outside the body.
The preoperative biliary stents were selected from the
following: endoscopic biliary stent, endoscopic nasobiliary
drainage tube, and self-expandable metallic stent,
according to the preference of the endoscopic physician
and the quality of the existing cholangitis.
Prophylactic peritoneal drains were placed in all
patients. The types of prophylactic drains were “open”
and “closed.” The former was used from 2001 to 2007,
and the latter was used thereafter. The closed drain was
maintained with vacuum at low pressure. o/s-SSI was
suspected by the property of the drain fluid and diagnosed
from results of the bacterial culture of the fluid.
The severity of the pancreatic fistulas was classified
according to International Study Group on Pancreatic
Fistula definitions [12].
Data are expressed as means ± standard deviation
(SD). Patient characteristics and perioperative and
postoperative variables were compared between the o/s-
SSI+ and o/s-SSI− groups using the χ2 and Fisher exact
tests. Variables with p-values<0.05 were incorporated
into a logistic regression model in order to determine the
independent risk factors for o/s-SSI. The independent
risk factors were expressed as odds ratios (ORs) and 95%
confidence intervals (CIs). All statistical analyses were
performed using JMP, version 12 (SAS Institute, Cary,
NC, USA). P-values <0.05 were considered statistically
significant.
RESULTS
The mean age of the patients was 72.6±9.3 years (range,
52–92 years). Of the 93 patients, 58 were male and 35
were female. The indications for operation were pancreas
head tumors in 44 patients (pancreatic head cancer in 36,
intraductal papillary mucinous neoplasm in seven, and
serous cystadenoma in one), bile duct tumors in 34 patients
(bile duct cancer in 33, and gall bladder cancer in one),
tumors of the papilla of Vater in seven patients (cancer in
five and adenoma in two), duodenal tumors in five patients
(cancer in three, gastrointestinal stromal tumor in one, and
lymphoma of mucosa-associated lymphoid tissue in one),
and others in two patients (fibrosing cholangitis in one and
gastric cancer recurrence in one).
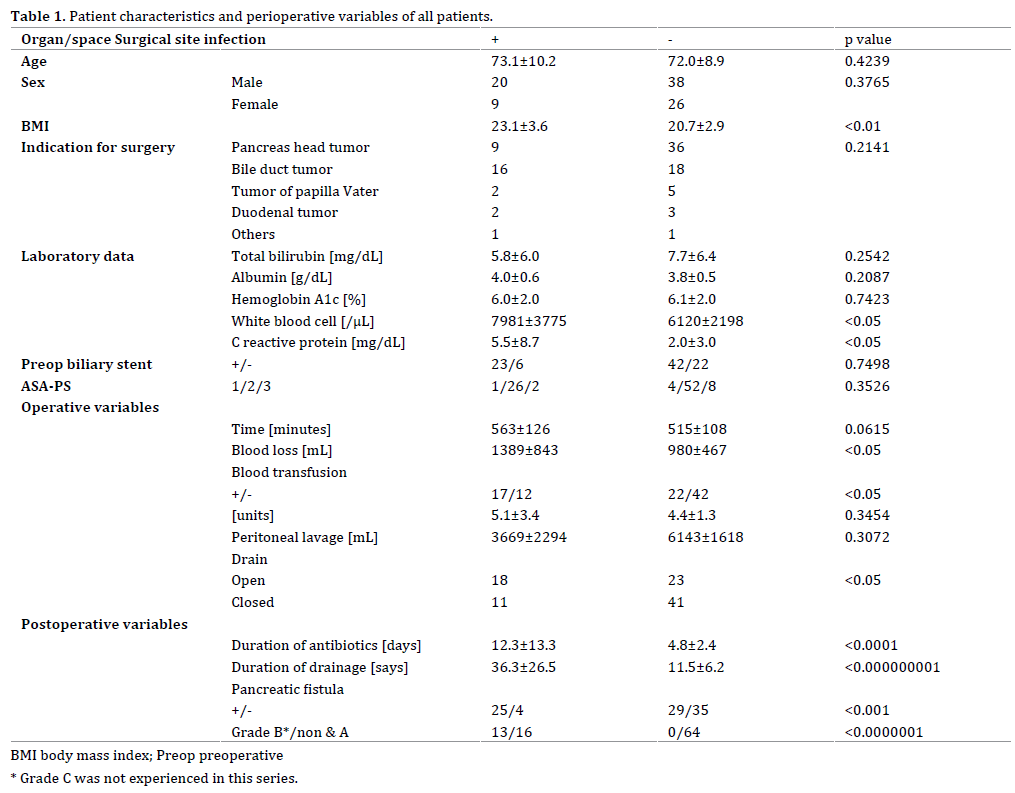
Comparison of Perioperative Variables between the
o/s-SSI+ and o/s-SSI− Groups
Of the 93 patients, 29 and 64 were included in the o/s-
SSI+ and o/s-SSI− groups, respectively. The comparison of
variables between the o/s-SSI+ and the o/s-SSI− groups
are presented in Table 1. Age and sex did not differ
significantly between the groups. However, BMI was significantly higher in the o/s-SSI+ group than in the o/s-
SSI− group (23.1±3.6 kg/m2 vs. 20.7±2.9 kg/m2, p<0.01).
The number of patients with pancreas head tumors
was higher in the o/s-SSI− group than in the o/s-SSI+;
however, the difference was not statistically significant.
The total bilirubin, albumin, and HbA1c levels did not
differ significantly between the two groups. The WBC
counts (7981±3775/mL vs. 6120±2198/mL, p<0.05) and
CRP levels (5.5±8.7 mg/dL vs. 2.0±3.0 mg/dL p<0.05) were
significantly higher in the o/s-SSI+ group than those in
the o/s-SSI− group. The incidence of preoperative biliary
stent placement and ASA-PS classifications did not differ
significantly between the two groups. Among operative
variables, blood loss was significantly higher in the o/s-
SSI+ group than that in the o/s-SSI− group (1389±843
mL vs. 980±467 mL, p<0.05), and blood transfusions were
performed more frequently in the o/s-SSI+ group than in
the o/s-SSI− group (17/29 vs. 22/64, p<0.05); however,
operative time and volume of peritoneal lavage did not
differ significantly between the two groups. The open
drain induced o/s-SSI significantly more frequently than
the closed drain (18/41 vs. 11/52, p<0.05). The duration
of prophylactic antibiotic administration was significantly
longer in the o/s-SSI+ group than in the o/s-SSI− group
(12.3±13.3 days vs. 4.8±2.4 days, p<0.0001). The duration
of drain placement was significantly longer in the o/s-
SSI+ group than in the o/s-SSI− group (36.3±26.5 days vs.
11.5±6.2 days, p <0.000000001). All grades of pancreatic
fistulas occurred in 54 of 93 patients, and they were
significantly more common in the o/s-SSI+ group than in
the o/s-SSI− group (25 of 29 patients vs. 29 of 64 patients,
p <0.001). High-grade (grades B and C) pancreatic fistulas
were not observed in the o/s-SSI− group (13 of 29 patients vs. 0 of 64 patients, p <0.0000001).
Risk Factors for o/s-SSI
The risk factors for o/s-SSI in univariate analysis
are presented in Table 2. The risk factors included
blood transfusion (OR, 2.70; p<0.05), peritoneal lavage
volume<5,000 mL (OR, 3.08; p<0.05), open type of
prophylactic drain (OR, 2.92; p<0.05), and the incidence of
pancreatic fistula (OR, 7.54, p<0.001).
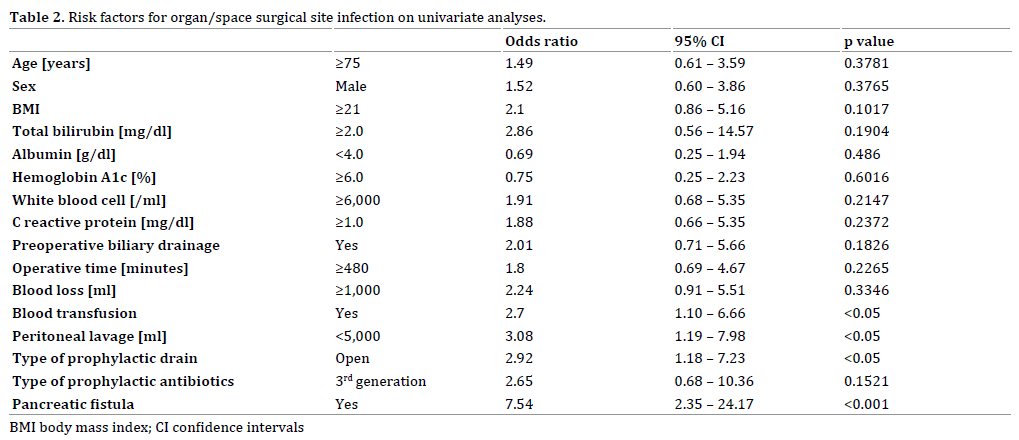
Multivariate logistic regression analysis did not reveal an
independent risk factor among the risk factors for o/s-SSI.
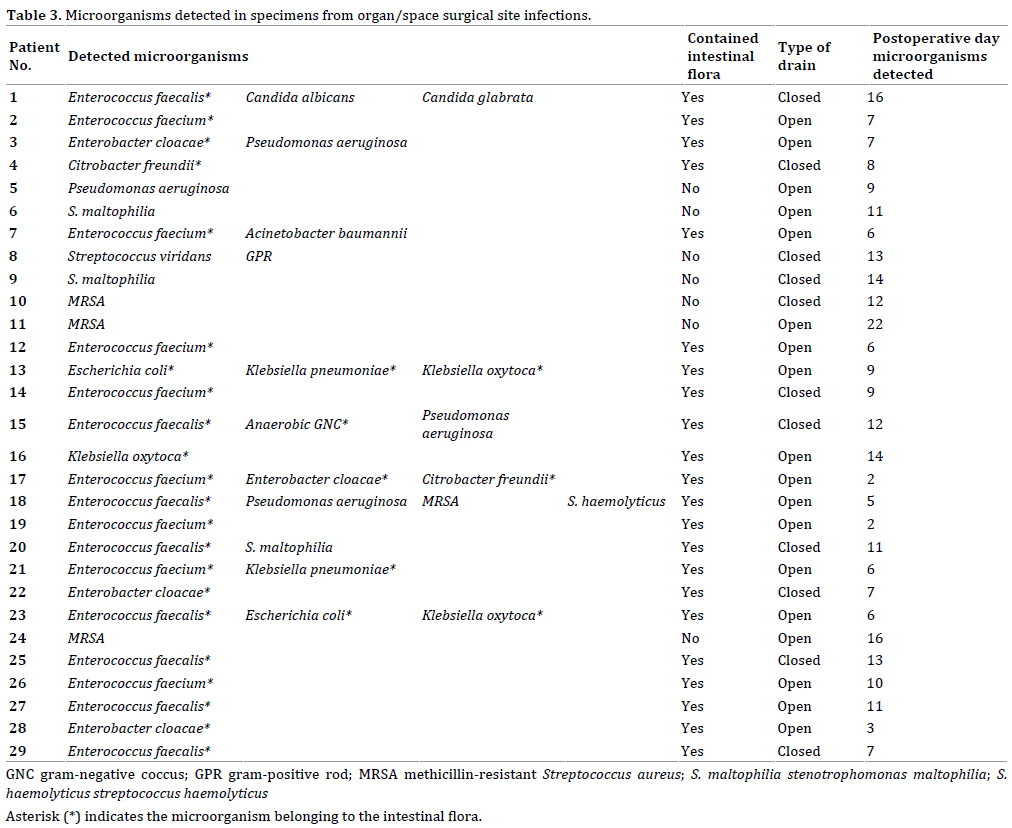
Microorganisms Related to o/s-SSI
Twenty-nine of the 93 patients were diagnosed with
o/s-SSI. Table 3 shows the microorganisms detected in
cultured fluid from the prophylactic drain when o/s-SSI
was clinically suspected. The microorganisms belonging
to intestinal flora were isolated from the drained fluid
sampled from 22 out of the 29 patients (75.9%). The
postoperative period, when microorganisms were detected
in the drained fluid, was 9.4±4.5 days (2 – 22 days, median
9 days). There was not a significant difference in this
period between patients with open drains (8.4±5.1 days,
2 – 22 days, median 7 days) and those with closed drains
(11.1±3.0 days, 7 – 16 days, median 12 days) (p = 0.1300).
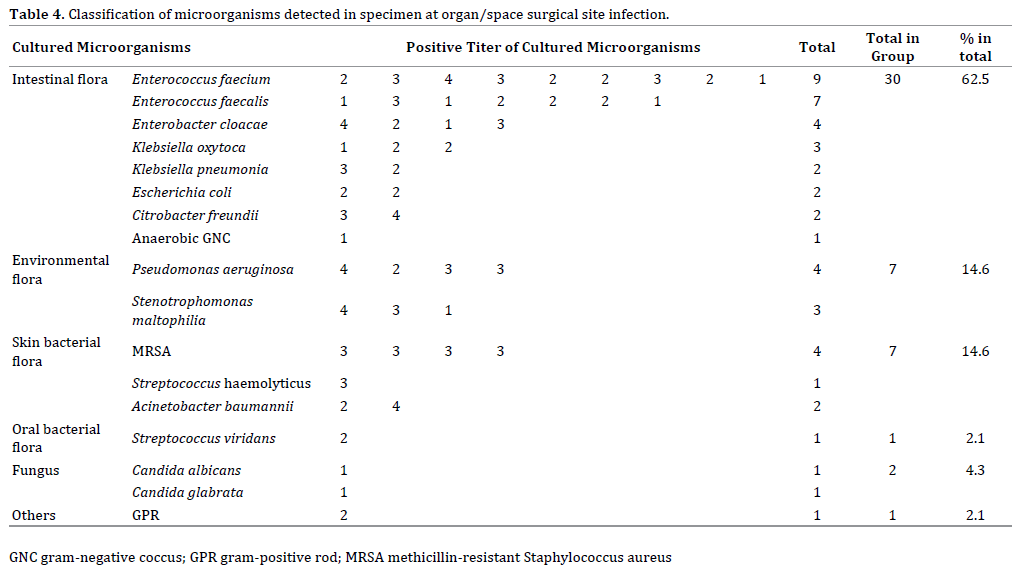
The 48 detected microorganisms included 30 (62.5%)
typically observed in intestinal flora, 7 (14.6%) from
environmental flora, 7 (14.6%) from skin flora, 1 (2.1%)
from oral flora, 2 (4.3%) from fungi, and 1 (2.1%) from
unclassified gram-positive rod. Bacteria of intestinal flora
were the most common cause of o/s-SSI (Table 4).
When classified by the type of drain, intestinal flora
were identified in samples from 21 patients (67.7%),
environmental flora in four patients (12.9%), and skin flora
in six patients (19.4%) with open drains, while intestinal
flora were identified in samples from nine patients
(52.3%), environmental flora in three patients (17.6%), skin flora in two patients (11.8%), fungus in two patients
(11.8%), and unclassified gram-positive rod in one patient
(5.9%) with closed drains. These results indicated that
there was not a significant difference between the two
types of prophylactic drain.
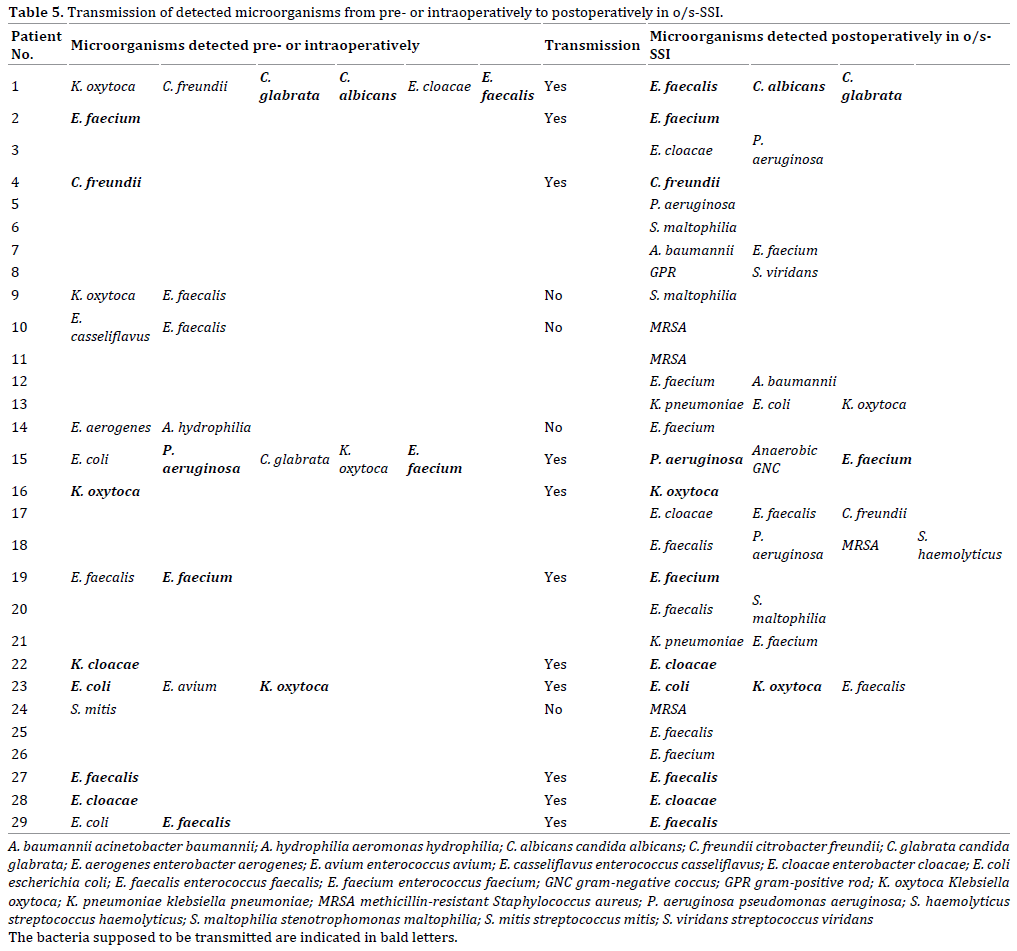
Microorganisms were identified in preoperatively
sampled bile or intra-operatively collected biliary stent
from 15 of 29 patients with o/s-SSI. In 11 of the 15
patients (73.3%), these microorganisms were the same
kind as those detected at the site of the o/s-SSI. Pre- and
intraoperative samples from the remaining 14 patients
were free from biliary microorganisms; in 10 of these
patients (71.4%), the microorganisms detected in the
o/s-SSI samples belonged to intestinal bacterial flora (p =
0.1729).
DISCUSSION
SSI is the most common type of nosocomial infection,
which is defined as an operation-related infection that
occurs at or near the incision site within 30 days, according
to the criteria from the United States Centers for Disease
Control and Prevention (CDC) [13].
The reported incidence rates of o/s-SSI after colorectal
surgery, and hepatectomy are 2.8–10% [5, 14, 15] and
4.0–8.6% [16, 17]. In comparison, the reported incidence
rates of o/s-SSI after PD are 47.8% (195 of 408 cases) [9]
and 45.0% (27 of 60 cases) [18]. In the present study, the
incidence of o/s-SSI after PD was 31.2% (29 of 93 cases),
which was much higher than that after any other type of
abdominal operation.
The relationship between prophylactic abdominal
drains and o/s-SSI has become the subject of debate. Kato et al. reported that intra-abdominal abscesses after PD
were found in the open-drain group only [19], and Sugiura et al. showed in multivariate analysis that the use of semiclosed
drain system was significantly associated with o/s-
SSI [9]. Also in our series, open drains were picked up as
a risk factor for o/s-SSI. The superiority of closed-type
drains has been confirmed for the suppression of o/s-SSI.
Only one paper was found, which concluded that
perioperative transfusions were associated with increased
risk factors of surgical site infections in newborns [20].
Also in our analyses, intraoperative blood transfusion was
one of the risk factors of o/s-SSI. Because the necessity of blood transfusion depends on the condition of the patients,
our efforts not to transfuse are limited.
There have been several reports of pancreatic fistulas
as a risk factor for o/s-SSI after PD. Sugiura et al.
emphasized that the presence of pancreatic fistulas was
the strongest risk factor for o/s-SSI [9], and Nanashima et al. reported the results of multivariate analysis
indicating that only postoperative pancreatic fistulas
were significantly associated with SSIs [21]. Because
there is a report that infection control could effectively
prevent pancreatic fistulas [22], it is clear that there
may be a close relationship between pancreatic fistulas
and o/s-SSI.
To our knowledge, no reports have concluded that
prophylactic drain placement after PD is meaningless
for the prevention of o/s-SSI. Many authors [23, 24, 25]
concluded that prophylactic drainage after pancreatic
resection did not decrease the frequency and severity
of postoperative complication; however, they did not
always deny drain placement. Wang et al. [23] concluded
that the necessity of drain placement was controversial,
and Dou et al. [8] stated in their systematic review
and meta-analysis that, although prophylactic drain
placement did not have a beneficial effect on the clinical
outcome, it did not significantly increase the risk of
abdominal abscess formation and that the elimination
of prophylactic abdominal drainage after PD led to a
significantly increased mortality rate (OR, 2.39; p =
0.01). Based on the literature, it is impossible to deny
the requirement of prophylactic drain placement after
PD.
Kawai et al. reported that drain removal on postoperative
day 4 was an independent factor in reducing the incidence of intra-abdominal infection [10]. Bassi et al. also reported
that a prolonged period of drain insertion was associated
with a higher rate of postoperative complication, and that,
in patients at low risk of pancreatic fistula, drains could be
safely removed on post-operative day three [11].
Thus, although the propriety of prophylactic drain
placement is controversial, there appears to be a consensus
that o/s-SSI may be less of a concern if the drain were to
be removed within term three to four days. However, this
consensus is inconsistent with the actual clinical course
after PD.
Sugiura et al. concluded that bacterial contamination
during PD had an adverse impact on the development of
o/s-SSI [26]. Horzog et al. also concluded that SSI was often
caused by the same microorganisms that were present
in intraoperative bile duct cultures [27]. In addition, we
showed intraoperative peritoneal lavage volumes <5000
mL to be a significant risk factor by univariate analysis
for the occurrence of o/s-SSI; furthermore, the use of
the antibiotics effective against the bacteria detected in
the perioperative bile samples inhibit the occurrence of
postoperative peritoneal infections [28, 29, 30]. Thus,
microorganisms derived from the bile may contaminate
the abdominal cavity intra-operatively, and induce o/s-
SSI.
In our analyses, intestinal bacterial flora was
detected in 75.9% patients with o/s-SSI (Table 3), and
comprised 62.5% of all detected bacteria in patients
with o/s-SSI (Table 4). Herzog et al. [27] and Sugiura et
al. [9] also reported gut-derived microorganisms to be
the predominant bacterial species in SSI foci. Because
biliary bacteria are gut-derived and bile contamination
may be the main cause of o/s-SSIs and intestinal bacteria were identified in o/s-SSI in patients with both
open and closed drains, there is no contradiction in the
conclusion that the origin of most o/s-SSI after PD was
the intra-peritoneal space or organs and that retrograde
infection through prophylactic drains is not the main
cause of o/s-SSI (Table 5).
CONCLUSION
The results of the current study confirm that pancreatic
fistulae are the most significant risk factor of o/s-SSI after
PD; in addition, based on our analysis of the microorganisms
detected in patients with o/s-SSI, the main causative
microorganisms of o/s-SSI originate in the peritoneal space
or organs. Several authors have recommended early removal
of prophylactic drain in order to prevent retrograde infection
through the drain, which could make o/s-SSI worse; therefore,
it is necessary to analyze and investigate the various aspects
related to drain management after PD.
Conflict of Interest
The authors have no financial conflicts of interest
concerning the manuscript to disclose.
References
- Berenguer CM, Ochsner MG Jr, Lord SA, Senkowski CK. Improving
surgical site infections: using national surgical quality improvement program
data to institute surgical care improvement project protocols in improving
surgical outcomes. J Am Coll Surg 2010; 210:737-741. [PMID: 20421041]
- Mahmoud NN, Turpin RS, Yang G, Saunders WB. Impact of surgical
site infections on length of stay and cost in selected colorectal procedures.
Surg Infect 2009; 10:539-544. [PMID: 19708769]
- Urban JA. Cost analysis of surgical site infections. Surg Infect 2006; 7
Suppl 1:S19-22. [PMID: 16834543]
- Liu HP, Zhang YC, Zhang YL, Yin LN, Wang J. Drain versus no-drain
after gastrectomy for patients with advanced gastric cancer: systematic
review and meta-analysis. Dig Surg 2011; 28:178-189. [PMID: 21540606]
- Tang R, Chen HH, Wang YL, Changchien CR, Chen JS, Hsu KC, et al. Risk
factor for surgical site infection after elective resection of the colon and
rectum: a single-center prospective study of 2,809 consecutive patients.
Ann Surg 2001; 234:181-189. [PMID: 11505063]
- Petrowsky H, Demartines N, Rousson V, Clavien PA. Evidence-based
value of prophylactic drainage in gastrointestinal surgery. Ann Surg
2004; 240:1074-1085. [PMID: 15570212]
- Van Buren G 2nd, Bloomston M, Hughes SJ, Winter J, Behrman
SW, Zyromski NJ, et al. A randomized prospective multicenter trial of
pancreaticoduodenectomy with and without routine intraperitoneal
drainage. Ann Surg 2014; 259:605-612. [PMID: 24374513]
- Dou CW, Liu ZK, Jia YL, Zheng X, Tu KS, Yao YM, et al. Systemic review
and meta-analysis of prophylactic abdominal drainage after pancreatic
resection. World J Gasrtoeterol 2015;21: 5719-5734. [PMID: 25987799]
- Sugiura T, Uesaka K, Ohmagari N, Kanemoto H, Mizuno T. Risk factor
of surgical site infection after pancreaticoduodenectomy. World J Surg
2012; 36:2888-2894. [PMID: 22907393]
- Kawai M, Tani M, Terasawa H, Ina S, Hirono S, Nishioka R, et al. Early
removal of prophylactic drains reduced the risk of intra-abdominal
infections in patients with pancreatic head resection. Ann Surg 2006;
244: 1-7. [PMID: 16794381]
- Bassi C, Molinari E, Malleo G, Crippa S, Butturini G, Salvia R, et al.
Early versus late drain removal after standard pancreatic resections:
results of a prospective randomized trial. Ann Surg 2010; 252:207-214.
[PMID: 20622661]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al.
International Study Group on Pancreatic Fistula Definition. Postoperative
pancreatic fistula: an international study group (ISDPF) definition.
Surgery 2005; 138:8-13. [PMID: 16003309]
- Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG. CDC
definitions of nosocomial surgical site infections, 1992: a modification
of CDC definitions of surgical wound infections. Infect Control Hosp
Epidemiol 1992; 13:606-608. [PMID: 1334988]
- Biondo S, Kreisler E, Fraccalvieri D, Basany EE, Codina-Cazador A,
Ortiz H. Risk factors for surgical site infection after elective resection for
rectal cancer. A multivariate analysis on 2131 patients. Colorectal Dis
2012; 14:e95-e102. [PMID: 21883813]
- Ho VP, Barie PS, Stein SL, Trencheva K, Milsom JW, Lee SW, et al.
Antibiotic regimen and the timing of prophylaxis are important for
reducing surgical site infection after elective abdominal colorectal
surgery. Surg Infect (Larchmt) 2011; 12:255-260. [PMID: 21790479]
- Kokudo T, Uldry E, Demartines N, Halkic N. Risk factors for incisional
and organ space surgical site infections after liver resection are different.
World J Surg 2015; 39:1185-1192. [PMID: 25561190]
- Sadamori H, Yagi T, Shinoura S, Umeda Y, Yoshida R, Satoh D, et al.
Risk factors for major morbidity after liver resection for hepatocellular
carcinoma. Br J Surg 2013; 100:122-129. [PMID: 23175234]
- Kimura F, Shimizu H, Yoshidome H, Ohtsuka M, Kato A, Yoshitomi H,
et al. Increased plasma levels of IL-6 and IL-8 are associated with surgical
site infection after pancreaticoduodenectomy. Pancreas 2006; 32:178-
185. [PMID: 16552338]
- Kato D, Sasaki T, Yamashita K, Shinya S, Nakashima R, Yamashita Y, et al.
Drain selection reduces pancreatic fistulae risk: a propensity-score matched
study. Hepatogastroenterology 2015; 62:485-492. [PMID: 25916087]
- Fawley J, Chelius TH, Anderson Y, Cassidy LD, Arca MJ. Relationship
between perioperative blood transfusion and surgical site infections in
the newborn population: An ACS-NSQIP-Pediatrics analysis. J Pediatr
Surg 2016; 51:1397-1404. [PMID: 27325358]
- Nanashima A, Abo T, Arai J, Oyama S, Mochinaga K, Matsumoto H.
Clinicopathological parameters associated with surgical site infection in
patients who underwent pancreatic resection. Hepatogastroenterology
2014; 61:1739-1743. [PMID: 25436372]
- Kobayasi S, Gotohda N, Kato Y, Takahashi S, Konishi M, Kinoshita
T. Infection control for prevention of pancreatic fistula after
pancreaticoduodenectomy. Hepatogastroenterology 2013; 60:876-882.
[PMID: 23732781]
- Wang Q, Jiang YJ, Li J, Yang F, Di Y, Yao L, et al. Is routine drainage
necessary after pancreaticoduodenectomy? World J Gastroenterol 2014;
20:8110-8118. [PMCID: PMC4081682]
- Adham M, Chopin-Laly X, Lepilliez V, Gincul R, Valette PJ, Ponchon T.
Pancreatic resection: drain or no drain? Surgery 2013; 154:1069-1077.
[PMID: 23876363]
- Kaminsky PM, Mezhir JJ. Intraperitoneal drainage after pancreatic
resection: a review of the evidence. J Surf Res 2013; 184: 925-930.
[PMID: 23866787]
- Sugiura T, Mizuno T, Okamura Y, Ito T, Yamamoto Y, Kawamura I,
et al. Impact of bacterial contamination of the abdominal cavity during
pancreaticoduodenectomy on surgical-site infection. Br J Surg 2015;
102:1561-1566. [PMID: 26206386]
- Herzog T, Belyaev O, Akkuzu R, Hölling J, Uhl W, Chromik AM. The
impact of bile duct cultures on surgical site infection in pancreatic
surgery. Surg Infect 2015; 16:443-449. [PMID: 26110464]
- Sudo T, Murakami Y, Uemura K, Hashimoto Y, Kondo N, Nakagawa
N, et al. Perioperative antibiotics covering bile contamination prevent
abdominal infectious complications after pancreaticoduodenectomy in
patients with preoperative biliary drainage. World J Surg 2014; 38:2952-
2959. [PMID: 25022981]
- Augenstein VA, Reuter NP, Bower MR, McMasters KM, Scoggins
CR, Martin RC. Bile cultures: a guide to infectious complications after
pancreaticoduodenectomy. J Surg Oncol 2010; 102:478-481. [PMID:
20872951]
- Kondo K, Chijiiwa K, Ohuchida J, Kai M, Fujii Y, Otani K, et al. Selection
of prophylactic antibiotics according to the microorganisms isolated from
surgical site infection (SSIs) in a previous series of surgeries reduces SSI
incidence after pancreaticoduodenectomy. J Hepatobiliary Pancreat Sci
2013; 20:286-293. [PMID: 22481442]

