Keywords
Alkylating Agents; BRCA1 Protein; BRCA2 Protein; Genes, BRCA1; Genes, BRCA2; Pancreatic Neoplasms; Poly(ADP-ribose) Polymerases
Abbreviations
PARP: poly(ADP-ribose) polymerase
INTRODUCTION
In the United States, one in four deaths are due to cancer. Pancreatic cancer is the fourth most common cause of cancer death and has the worst 5-year survival rate at 6% [1]. A family history of pancreatic cancer is found in 5-10% of pancreatic cancer patients [2, 3]. Of the known genetic mutations involved in familial pancreatic cancer, BRCA1 and BRCA2 are the most common. These genes are involved in the repair of double-strand DNA breaks and act as tumor suppressor genes. BRCA2 mutation carriers have a 3.5-fold risk of developing pancreatic cancer [4, 5]. The risk associated with BRCA1 mutation is unclear as some studies suggested a 2.2-fold risk, while others have shown no increased risk. The unique biology of cancer cells with BRCA mutations offers potential therapeutic advantages with agents such as platinums, that induce DNA double-strand breaks, and poly(ADP-ribose) polymerase (PARP) inhibitors, which prevent PARP in tumor cells from repairing single-strand breaks leading eventually to cell death. Due to the relative rarity of BRCA-positive pancreatic cancer, there is a paucity of literature in this area.
What Did We Learn at the 2013 ASCO Gastrointestinal Cancers Symposium?
At this meeting, there were two abstracts that furthered our knowledge of BRCA-positive pancreatic adenocarcinoma.
Perspectives on Platinum-Based Chemotherapeutics
In patients with BRCA associated ovarian cancer, platinum-based chemotherapy appears to be particularly efficacious [6]. However, less is known about the characteristics and response of BRCAassociated pancreatic adenocarcinoma. Golan et al. (Abstract #278 [7]) identified patients with BRCA1 or BRCA2-associated pancreatic adenocarcinoma from the databases of three institutions. They found 63 cases of BRCA-associated pancreatic cancer. BRCA2- associated disease accounted for over two-thirds of the cases. One patient had both BRCA1 and BRCA2 mutations (after discussion with the original author, the numbers of each subtype of BRCA-associated cases identified differs from the original published abstract and are corrected here in Table 1). Among patients with stage IV disease, 12 were treated with platinumbased first-line chemotherapy and had a median progression free survival of 90 days compared to 18 patients who were treated with non-platinum-based regimens and had a median progression free survival of 92 days (P=0.641). Data is summarized in Table 1. Disease in two patients became resectable after downstaging with gemcitabine/cisplatin chemotherapy.
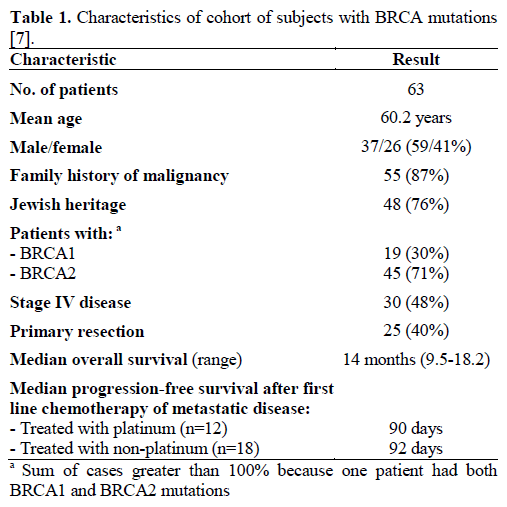
The authors concluded that the natural history of BRCA-associated pancreatic adenocarcinoma was similar to the sporadic cases. Also, in patients with metastatic disease, platinum-based regimens did not produce a superior progression free survival compared to non-platinum regimens.
Promise of PARP Inhibitors
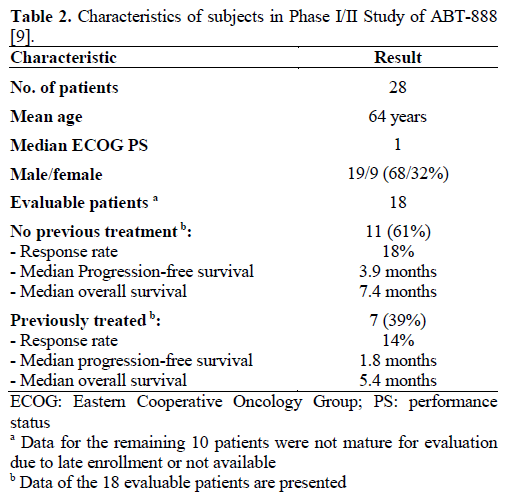
ABT-888 is a PARP inhibitor currently in phase I and II clinical trials for the treatment of various malignancies [8]. PARP inhibitors are thought to have potent sensitizing effects to chemotherapy. Pishvaian et al. (Abstract #147 [9]) presented data from the phase I portion of their phase I/II trial in metastatic pancreatic cancer. Patients were enrolled in a trial with standard dose escalation of ABT-888 and treated concurrently with 5-FU, leucovorin and oxaliplatin. Twenty-eight patients were enrolled with 18 patients being evaluable at the time of this presentation. For the 11 patients who had received no prior treatment, response rate was 18%, with a progression free survival and overall survival of 3.9 and 7.4 months, respectively. Seven of the patients had prior therapy. The progression free survival and overall survival of this group were 1.8 and 5.4 months with a response rate of 14%. Data are reported in Table 2. Two patients had BRCA2-associated pancreatic cancer. One achieved a partial response until progressing at 17 months. He is alive still at 22 months. The other had a complete response and is alive still at 14 months. This combination regimen with the PARP inhibitor appears well tolerated and potentially efficacious. Patients with BRCA2 mutations may be particularly responsive to this agent.
Discussion
While BRCA-associated pancreatic cancer is the most common known cause of familial pancreatic cancers accounting for up to 17% of cases, our knowledge of this disease is limited by its relative rarity still [10]. With the poor survival observed in pancreatic cancer, there is much interest in exploiting any therapeutic targets the BRCA mutation may confer. BRCA1 is involved with DNA damage surveillance and repair responses while BRCA2 plays a role in repairing DNA double-stranded breaks by homologous recombination [2, 8]. If these proteins are dysfunctional, the cell cannot use the more accurate homologous recombination to repair double-strand breaks and instead must rely upon more error-prone repair mechanisms which are more likely to result in cell death. Thus, agents such as platinum chemotherapy, which induce DNA double-strand breaks, and PARP inhibitors, which inhibit single-strand break repairs, have been the focus of much research. Considering the potentially important therapeutic implications, BRCA testing by DNA sequencing is commercially available and may be appropriate testing for patients with a family history of cancer [3, 11].
In a prior study by Lowery et al. involving 15 patients with BRCA-associated pancreatic cancer, they found a marked response in a subset of patients with metastatic disease to first-line platinum-based chemotherapy with 5 out of 6 patients developing a complete or partial response. However, in Abstract #278, Golan et al. did not observe a significant difference in progression free survival in 30 patients with metastatic disease treated with platinum-based chemotherapy compared to nonplatinum regimens. The apparent differences in effectiveness are intriguing. Upon publication, further examination of the complete characteristics of the patients in this study may yield further information. In the Lowery et al. study, all the patients with metastatic disease who were treated with platinum had BRCA2 mutations. It will be interesting to evaluate the distribution of the BRCA1/2 mutation between the treatment groups in Golan et al. study. It has been observed in ovarian cancer that patients with BRCA2 mutations are more chemosensitive compared to BRCA1 [12]. The role of platinum agents in patients with BRCA-associated pancreatic cancer is challenged by this study.
PARP inhibitors are another agent that may be particularly effective in BRCA-associated pancreatic cancer. In the cohort of 15 patients identified by Lowery et al., three patients were treated with PARP inhibitors. Two of the three patients had a partial response and one had stable disease. There has even been a case report of a patient with BRCA2-associated pancreatic cancer developing a complete response after receiving treatment with gemcitabine plus a PARP inhibitor [13]. In Abstract #147, Pishvaian et al. presented data from the phase I portion of a study in patients with metastatic pancreatic cancer treated with a PARP inhibitor (ABT-888) in combination with 5- FU and oxaliplatin. Although there were only two patients with BRCA2 mutations in this study, both of them had an impressive response. One achieved a partial response and is still on study at 17 months while the other reached a complete response and remains on study after 10 months. These data are very intriguing and further support the limited data that exist.
Although studies on BRCA-associated pancreatic cancer are limited, both abstracts presented at the 2013 ASCO Gastrointestinal Cancers Symposium further contribute to our knowledge of this uncommon disease. While the efficacy of platinum-based chemotherapeutics has become less clear, the data on PARP inhibitors appear all the more promising. With the limited number of reports on patients with BRCAassociated pancreatic cancer, more studies will be needed to shed further light as to whether the effectiveness of these agents are as great as our expectations.
Conflict of interest
The authors have no potential conflicts of interest.
References
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA: A Cancer Journal for Clinicians 2013; 63: 11–30. [PMID: 23335087].
- Lowery MA, Kelsen DP, Stadler ZK, Yu KH, Janjigian YY, Ludwig E et al. An emerging entity: pancreatic adenocarcinoma associated with a known BRCA mutation: clinical descriptors, treatment implications, and future directions. Oncologist 2011; 16:1397-1402. [PMID: 21934105]
- Klein AP. Genetic susceptibility to pancreatic cancer. Mol Carcinog. 2012;51:14-24. [PMID: 22162228].
- The Breast Cancer Linkage Consortium. Cancer Risks in BRCA2 Mutation Carriers. J Natl Cancer Inst 1999; 91(15): 1310-1316. [PMID: 10433620].
- Thompson D, Easton DF. Cancer Incidence in BRCA1 mutation carriers. J Natl Cancer Inst 2002; 94:1358–65. [PMID: 12237281].
- Cass I, Baldwin RL, Varkey T, Moslehi R, Narod SA, Karlan BY. Improved survival in women with BRCA-associated ovarian carcinoma. Cancer 2003; 97: 2187–2195. [PMID: 12712470].
- Golan T, Kanji Z, Epelbaum R, Devaud N, Dagan E, Holter S et al. Chemosensitiviy and clinical characteristics of pancreatic malignancies in BRCA mutation carriers. J Clin Oncol 2013; Abstract 278.
- Do K, Chen A. Molecular pathways: Targeting PARP in cancer treatment. Clin Cancer Res 2012; in publication. [PMID: 23269547].
- Pishvaian M, Wang H, Zhuang T, He A, Hwang J, Hankin A, Ley L, et al. A phase I/II study of ABT-888 in combination with 5- fluorouracil (5-FU) and oxaliplatin (Ox) in patients with metastatic pancreatic cancer (MPC). J ClinOncol 2013; Abstract 147.
- Murphy KM, Brune KA, Griffin C, Sollenberger JE, Petersen GM, Bansal R et al. Evaluation of candidate genes MAP2K4, MADH4, ACVR1B and BRCA2 in familial pancreatic cancer: deleterious BRCA2 mutations in 17%. Cancer Res 2002; 62:3789– 93. [PMID: 12097290].
- Myriad Genetic Laboratories. “Panexia.” Www.Myriadpro.Com. Myriad Genetic Laboratories. Web Feb 2013. < https://www.myriadpro.com/test-offerings/genetic-testing/panexia>.
- Yang D, Khan S, Sun Y, Hess K, Shmulevich I, Sood AK et al. Association of BRCA1 and BRCA2 mutations with survival, chemotherapy sensitivity, and gene mutator phenotype in patients with ovarian cancer. JAMA 2011; 306: 1557–1565. [PMID: 21990299].
- Fogelman DR, Wolff RA, Kopetz S, Javle M, Bradley C, Mok I, et al. Evidence for the efficacy of Iniparib, a PARP-1 inhibitor, in BRCA2-associated pancreatic cancer. Anticancer Res 2011; 31(4): 1417-1420. [PMID: 21508395].

