Caroline Lacombe1,2, Louis de Mestier1,2, Yohann Grassano2,3, Margot Bucau2,4, Magaly Zappa2,5, Philippe Lévy1,2
1Department of Gastroenterology and Pancreatology, Beaujon Hospital (APHP), Clichy, France
2Paris 7 University, Paris, France
3Department of Urology, Bichat Hospital (APHP), Paris, France
4Department of Pathology, Bichat Hospital (APHP), Paris, France
5Department of Radiology, Beaujon Hospital (APHP), Clichy, France
- *Corresponding Author:
- Louis de Mestier
Department of Gastroenterology and Pancreatology
Beaujon Hospital (APHP), Clichy, France
Phone +33140875225
Fax +33 0142703784
E-mail louis.demestier@aphp.fr/louisdemestier@hotmail.com
Received June 29th, 2018 – Accepted September 11th, 2018
Keywords
Immunohistochemistry; Neoplasm Metastasis; Pancreatic Neoplasms; Urinary Bladder
Abbreviations
BM bladder metastasi(e)s; CT computed tomography; PDAC pancreatic ductal adenocarcinoma
INTRODUCTION
Pancreatic ductal adenocarcinoma (PDAC) is the seventh most frequent cause of cancer worldwide and will become the second most common cause of cancer-related death in 2030 [1]. Its prognosis is very poor with 5-year survival rate around 5% for all stages together, especially because it is usually diagnosed at a late stage when the tumor has already metastasized to distant organs. Indeed, around 50% of the patients with PDAC have metastases synchronous to the diagnosis. The most common metastatic location of PDAC is the liver, the peritoneum and the lungs. PDAC-related bladder metastases (BM) are very infrequent and may mimic primary urothelial malignancies. We report here a case of a patient with metastatic PDAC who developed asymptomatic BM two years after the initial diagnosis, and provide a comprehensive literature review of similar cases.
CASE REPORT
A Seventy-six-year-old woman was referred in October 2015 for abdominal pain. She had a medical history of right ovarian benign cysts, negligible alcohol consumption and limited tobacco use interrupted 20 years ago. A computed tomography (CT) of the abdomen revealed a mass in the area of the body of the pancreas with synchronous pulmonary and peritoneal nodules. Endoscopic ultrasonography with biopsy was performed and pathological examination revealed well-differentiated PDAC. She was treated by chemotherapy which consisted in FOLFIRINOX regimen. This treatment started on November 2015, oxaliplatin was interrupted on April 2016 because of neurotoxicity and stable disease. She then received 5-fluorouracile only from October 2016 because of stable disease. Tumor evolution was assessed by CT-scan every 3 months, and was always stable.
On September 2017, she had received a total of 42 chemotherapy cycles. A new reevaluation CT-scan revealed an enhanced lesion of the posterolateral wall of the bladder, measuring 11 mm (Figure 1a). No pancreatic, pulmonary or peritoneal progression was present on this CT-scan comparing to the pretreatment imaging, indicating the absence of disease progression. Moreover, the patient was still in excellent general condition (ECOG 0) and did not have any clinical sign of disease progression. Retrospectively, this lesion was already present but was not noticed on the CT-scan of January 2017 (Figure 1b). We observed that this lesion had grown slowly from 3 mm to 11 mm. The patient had no history of urinary disease and no urinary symptom. Cystoscopy was performed and revealed a unique 12-mm lesion of the left lateral bladder wall, distant from left ureter with no associated urothelial lesion. This lesion was removed by transurethral resection and its pathological analysis showed an adenocarcinoma invading the muscularis propria with lymphovascular invasion (Figure 2a). Its morphological features were compatible with those of the PDAC, including mucosecretion as demonstrated with Alcian blue staining (Figure 2b) and MUC1 expression (Figure 2c). None of the previous CT-scans showed peritoneal carcinomatosis close to the bladder. The final diagnosis retained was BM from PDAC. After discussion at oncological multidisciplinary meeting, the same treatment was continued given the absence of disease progression elsewhere, the excellent general condition and tolerance of the treatment. Six months after the resection of the BM, the patient was still stable with unremarkable clinical examination.
Figure 1. Contrast-enhanced CT-scans performed for the follow-up of a 76-year old patient with pancreatic ductal adenocarcinoma. (a). diagnosis of a 11 mm enhanced nodule of the left posterolateral wall of the bladder (September 2017). (b). retrospectively this nodule was present as from January 2017.
Figure 2. Pathologic examination of the bladder nodule. Infiltration of the muscularis propria of the bladder by adenocarcinoma ((a). Hematoxylin-Phloxine-Saffron, 100X) with evidence of mucosecretion ((b). Alcian blue, 200X) and membranous and cytoplasmic expression of MUC1 ((c). anti-MUC1
antibody, 100X).
DISCUSSION
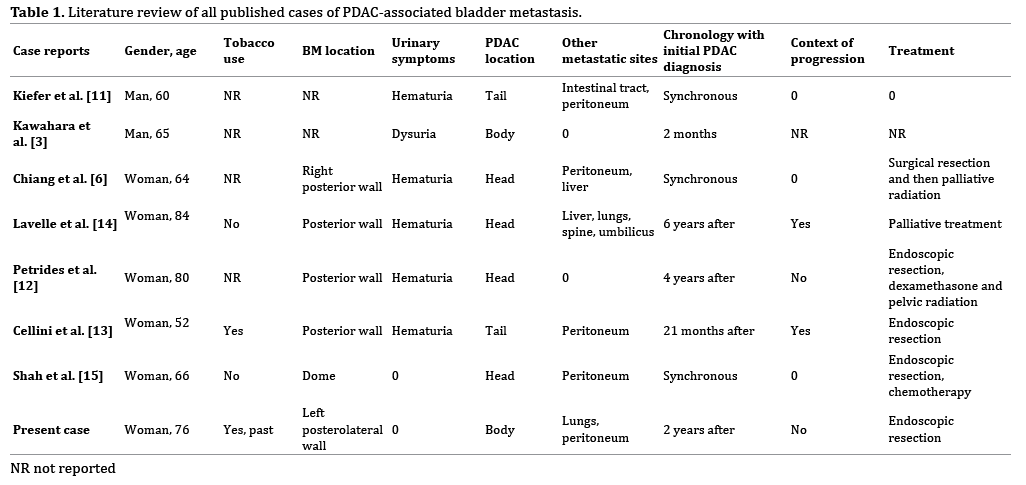
BM from PDAC is very rare, with unknown prevalence. Because of the intimate anatomical relationship of the kidney and the pancreas, the involvement of the urinary tract is not uncommon in PDAC. Cases of urinary lesions were previously described, such as ureteral obstruction, kidney mass, or renal compression which accounted for 10/25, 5/25, and 10/25 patients respectively, in the restrospective series by Warden et al. [2] and 5/10 and 4/10 patients respectively in the retrospective study by Kawahara et al. (no case of renal compression) [3]. However, BM are even more exceptional. In two necropsy series, BM accounted for 2/609 cases and 1/96 cases respectively [4, 5]. Moreover, in the literature, from 1951 to 1980, around ten cases of bladder metastasis have reported through series, with no precise case description although urinary symptoms seemed unfrequent (1/15 patient presented with hematuria in the review by Chiang et al.) [6, 7, 8, 9, 10]. We reported 7 cases of PDAC-associated BM summarized in Table 1 [3, 6, 11, 12, 13, 14, 15]. The majority was women and had a unique pathologically-proven BM mostly located in the posterior wall of the bladder, one was located on the dome. Six patients had urinary symptoms, especially hematuria. Excepted in two patients who had isolated BM [3, 12], PDAC was associated with other metastatic locations, the most frequent one being peritoneum. This raises the question whether those BM might be, in fact, peritoneal carcinomatosis invading the bladder. However, in our case, the patient had no pelvic carcinomatosis and there was no aspect of extrinsic compression during cystoscopy. Another diagnostic issue was making the distinction between BM and urinary primary tumor, notably because both PDAC and urothelial carcinoma occur in patients with tobacco use. This may be ruled out by pathological examination, as bladder adenocarcinoma is very rare. Additional immuno-histochemical analyses, including MUC-1 immunostaining, were useful.
CONCLUSION
In summary, PDAC-associated BM is very rare but must be suspected in patients with PDAC and unique bladder tumor.
Conflict of Interest
The authors declare no conflict of interest.
References
- Neuzillet C, Tijeras-Raballand A, Bourget P, Cros J, Couvelard A, Sauvanet A, et al. State of the art and future directions of pancreatic ductal adenocarcinoma therapy. Pharmacol Ther 2015; 155:80–104. [PMID: 26299994].
- Warden SS, Fiveash JG, Tynes WV, Schellhammer PF. Urologic Aspects of Pancreatic Adenocarcinoma. J Urol 1981; 125:265–267. [PMID: 7206071].
- Kawahara S, Honda M, Li KS, Kosuda S, Tamura K, Nobusawa H, et al. Urinary tract involvement from pancreas carcinoma. Nihon Igaku Hoshasen Gakkai Zasshi 1989; 49:1102–1111. [PMID: 2587193].
- Bell ET. Carcinoma of the pancreas. I. A clinical and pathologic study of 609 necropsied cases. II. The relation of carcinoma of the pancreas to diabetes mellitus. Am J Pathol 1957; 33:499–523. [PMID: 13424657].
- Sheehan EE, Greenberg SD, Scott R. Metastatic neoplasms of the bladder. J Urol 1963; 90:281–284. [PMID: 14055988].
- Chiang KS, Lamki N, Athey PA. Metastasis to the bladder from pancreatic adenocarcinoma presenting with hematuria. Urol Radiol 1991; 13:187–189. [PMID: 1539411].
- Klinger ME. Secondary Tumors of the Genito-Urinary Tract. J Urol 1951; 65:144–153. [PMID: 14804776].
- van Dyk D, Lang R, Jutrin Y, Shapira J, Ravid M. Bizarre urologic manifestations of pancreas carcinoma. Hepatogastroenterology 1980; 27:62–63. [PMID: 7203359].
- Goldstein AG. Metastatic carcinoma to the bladder. J Urol 1967; 98:209–215. [PMID: 6046998].
- Sommers SC, Meissner WA. Unusual carcinomas of the pancreas. AMA Arch Pathol 1954; 58:101–111. [PMID: 13170907].
- Everett D, Kiefer MD. Carcinoma of the pancreas. Arch Intern Med 1927; 40:1-29.
- Petrides N, Singh R, Hodgson D. A case of delayed vesical pancreatic adenocarcinoma metastasis. J Clin Urol 2013; 6:127–128.
- Cellini M, Deighton D. Radiological Case: Non-papillary bladder metastasis from pancreatic adenocarcinoma. Appl Radiol 2014; 43:74–6.
- Lavelle RS, Williams SB, O’Leary MP. An 84-Year-old Female with Gross Hematuria. Urology 2011; 77:533–534. [PMID: 21215435].
- Shah A, Korrapati P, Siegel J, Kasmin F. Rare Metastasis of Primary Pancreatic Adenocarcinoma to the Bladder. ACG Case Rep J 2018; 5:e27. [PMID: 29619402].



