Kathryn LA Rogers, Ravindra S Date, Jeremy B Ward
Department of Gastrointestinal Surgery, Lancashire Teaching Hospitals NHS Foundation Trust. Chorley, Lancashire, United Kingdom
- *Corresponding Author:
- Ravindra S Date
Department of Gastrointestinal Surgery
Lancashire Teaching Hospital NHS Foundation
Trust Preston Road Chorley Lancashire, PR7
1PP United Kingdom
Phone: +44-01257.245.267
Fax: +44-01257.245.495
E-mail: ravidate@hotmail.com
Received November 28th, 2007 - Accepted December 14th, 2007
Keywords
Amylases; Pancreatitis; Shock, Septic
INTRODUCTION
The recent review of Atlanta classification recommends that the diagnosis of acute pancreatitis should incorporate two of the following three criteria: upper abdominal pain, amylase and/or lipase levels at least three times the upper limit of normal, and CT or MRI findings compatible with acute pancreatitis [1].
Hyperamylasaemia can also be associated with other conditions such as parotitis, peritonitis, ectopic pregnancy, severe sepsis and acidosis [2]. However serum amylase levels rarely exceed three times upper limit of normal in these conditions.
Toxic shock syndrome, secondary to Staphylococcus infection, is well recognised in young girls following the use of tampons, and can be associated with hyperamylasaemia.
We report a case of a young girl who presented with upper abdominal pain and very high serum amylase levels combined with systemic shock causing a diagnostic dilemma.
CASE REPORT
A young girl of 17 was admitted to the medical assessment unit with sudden onset of diarrhoea and vomiting over the previous 12 hours. She also complained of upper abdominal and back pain. She was known to be sexually active and was currently menstruating. She denied drinking alcohol. On examination she was cold and clammy. Her pulse was 119 beats/min, temperature 38.5°C and blood pressure was 124/42 mmHg. Abdominal examination revealed minimal tenderness in right upper quadrant but was otherwise unremarkable. At the time of catheterisation she was found to have a retained tampon, which was removed, and vaginal swabs were sent for culture.
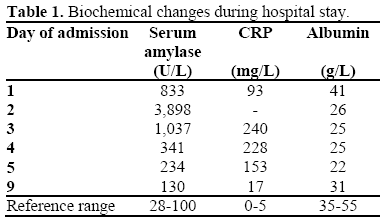
Her blood investigations showed severe metabolic acidosis, hemoglobin 15.1 g/dL (reference range: 11.5-16.5 g/dL), white blood cells 17.2 x109/L (reference range: 4-11 x109/L), urea 8.4 mmol/L (reference range: 1.7-8.3 mmol/L), creatinine 339 μmol/L (reference range: 44-80 μmol/L) and serum amylase 833 U/L (reference range: 28-100 U/L). Her urine examination was entirely normal. She was referred to surgeons with the working diagnosis of acute pancreatitis. An urgent CT scan was requested which showed some retroperitoneal oedema but a completely normal pancreas (Figure 1). Urology consult was made to rule out renal sepsis. She was also examined by the gynaecologists who thought that the diagnosis of toxic shock was unlikely. She was commenced on broadspectrum intravenous antibiotics. Over the next 24 hours her condition deteriorated, and she developed multi-organ failure (MOF) requiring ventilatory and ionotropic support along with haemofiltration. Serum amylase levels reached 3,898 U/L. Rest of the relevant daily investigations are tabulated in Table 1.
Figure 1. CT scan showing normal pancreas.
Two days later she had an ultrasound scan which showed a normal pancreas and no gallstones in the gallbladder. In the interim her blood cultures grew Staphylococcus aureus, as did the vaginal swabs supporting the diagnosis of toxic shock. Her stool cultures also grew Shigella and so appropriate alterations to the antibiotics were made. Over next few days her general condition improved and serum amylase levels returned to normal. The patient made a full recovery and was discharged home 8 days later.
DISCUSSION
Toxic shock syndrome is a clinical condition most commonly caused by either
Staphylococcus aureus or Streptococcus pyogenes. Hyperamylasaemia in toxic shock is due to acinar cell damage, secondary to either overwhelming sepsis or the toxins produced by the organisms.
In this case it is not clear why serum amylase levels reached such high levels that are not normally associated with toxic shock syndrome. Possible mechanisms, which could have contributed to extreme hyperamylasaemia in our patient, are renal failure, impairing the clearance of amylase, and Shigella infection. Though there is no reported association between the Shigella infection and pancreatitis, acute pancreatitis secondary to Campylobacter jejuni infection has been reported, particularly in the presence of genetic mutations [3]. We suspect that some element of acute interstitial pancreatitis itself could have contributed to hyperamylasaemia. However, it is unlikely that severe acute pancreatitis complicated by three-organ-failure would respond so dramatically to antibiotics and recover so quickly.
In this case the peak serum amylase level of 3,898 U/L led us to believe in the diagnosis of pancreatitis, even though the overall clinical presentation was not entirely in keeping with this. Review of the clinical situation and the quest for logical explanation of patient’s clinical condition led us to the diagnosis of toxic shock syndrome secondary to a retained tampon.
Toxic shock syndrome can mimic several common diseases [4] and so can be difficult to diagnose. The incidence of toxic shock syndrome is increasing [5, 6] and a high index of suspicion is necessary for the diagnosis, especially as the presentation may not be classical [7].
In conclusion, we suggest that even such high level of serum amylase may not always be diagnostic of pancreatitis, especially when an obvious cause is not demonstrated. The management of the patients should be guided by repeated evaluation of clinical situation and not merely by conventional interpretation of biochemistry results.
References
- Bollen TL, van Santvoort HC, Besselink MG, van Leeuwen MS, Horvath KD, Freeny PC, et al. The Atlanta Classification of acute pancreatitis revisited. Br J Surg 2008; 95:6-21. [PMID 17985333]
- Frulloni L, Patrizi F, Bernardoni L, Cavallini G. Pancreatic hyperenzymemia: clinical significance and diagnostic approach. JOP. J Pancreas (Online) 2005; 6:536-51. [PMID 16286704]
- Kandula L, Khan S, Whitcomb DC, Lowe ME. Acute pancreatitis in association with Campylobacter jejuni-associated diarrhea in a 15-year-old with CFTR mutations: is there a link? JOP. J Pancreas (Online) 2006; 7:482-5. [PMID 16998246]
- Herzer CM. Toxic shock syndrome: broadening the differential diagnosis. J Am Board Fam Pract 2001; 14:131-6. [PMID 11314920]
- Schlievert PM, Tripp TJ, Peterson ML. Reemergence of staphylococcal toxic shock syndrome in Minneapolis-St. Paul, Minnesota, during the 2000- 2003 surveillance period. J Clin Microbiol 2004; 42:2875-6. [PMID 15184497]
- Tierno PM Jr. Reemergence of staphylococcal toxic shock syndrome in the United States since 2000. J Clin Microbiol 2005; 43:2032-3. [PMID 15815055]
- Taylor CM, Riordan FA, Graham C. New football boots and toxic shock syndrome. BMJ 2006; 332:1376- 8. [PMID 16763251]


