Keywords
Autoimmunity; Pancreatitis;
Steroids
Abbreviations
ACA-II: anti-carbonic
anhydrase II antibody; AIP: autoimmunerelated
pancreatitis; ALF: anti-lactoferrin
antibody; AMA: anti-mitochondrial antibody;
ANA: anti-nuclear antibody; ASMA: antismooth
muscle antibody; BT-PABA: Nbenzoyl-
L-tyrosyl-para-aminobenzoic acid;
CA-II: carbonic anhydrase-II; CBD: common
bile duct; DM: diabetes mellitus; ELISA:
enzyme-linked immunosorbent assay; ERCP:
endoscopic retrograde cholangiopancreatography;
FDG: F-18 fluoro-2-deoxy-
D-glucose; IDDM: insulin dependent diabetes
mellitus; IFN-g: interferon-g; IL-4:
interleukin-4; LF: lactoferrin; LPSP:
lymphoplasmacytic sclerosing pancreatitis;
mAb: monoclonal antibody; MRCP: magnetic
resonance cholangio-pancreatography;
NIDDM: not insulin dependent diabetes
mellitus; nTx: neonatally thymectomized;
PBC: primary biliary cirrhosis; PBL:
peripheral blood lymphocyte; PET: positron
emission tomography; PNPD: pancreatitis
showing the narrowing appearance of the
pancreatic duct; PSC: primary sclerosing
cholangitis; RA: rheumatoid arthritis; RF:
rheumatoid factor; SjS: Sjögren's syndrome
Introduction
Idiopathic pancreatitis, in which obvious
causes are not detected, accounts for about
30-40% of cases of chronic pancreatitis [1].
Since Sarles et al. observed the first case of
pancreatitis with hypergammaglobulinemia
[2], the occasional coexistence of pancreatitis
with other autoimmune diseases such as
Sjögren's syndrome (SjS) [3], primary
sclerosing cholangitis (PSC) [4, 5] or primary
biliary cirrhosis (PBC) [4] has been reported.
These findings support the hypothesis that an
autoimmune mechanism may be involved in
the pathogenesis and pathophysiology in
some patients with pancreatitis [6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16, 17], which leads us to
the concept of autoimmune-related
pancreatitis [15], which is called
"autoimmune pancreatitis" (AIP) [8].
Recently, the concept of AIP is thought to be
acceptable as a new clinical entity due to its
unique clinical and histological findings.
Several hundred cases of AIP have been
reported in the Japanese literature [5, 8, 9, 10, 11, 12, 13, 18, 19, 20]. We encountered 30
cases of AIP in a total of 620 cases of chronic
pancreatitis (5%). Males are predominant and
most patients were diagnosed at middle or
advanced age (mean: 58 years). In this paper,
we report recent etiopathological and clinical
findings based on our experience.
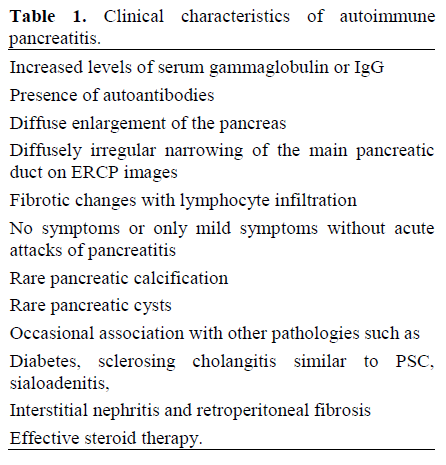
Definition and Concept of AIP
Although the pathogenesis and pathophysiology
of AIP are still unclear, clinical
aspects have been accumulated [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16]. The
characteristic findings in the most cases of
AIP [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16] can be summarized as follows: i)
increased levels of serum gammaglobulin or
IgG; ii) the presence of autoantibodies; iii)
diffuse enlargement of the pancreas; iv)
diffusely irregular narrowing of the main
pancreatic duct on endoscopic retrograde
cholangio-pancreatography (ERCP) images;
v) fibrotic changes with lymphocyte
infiltration; vi) no symptoms or only mild
symptoms, usually without acute attacks of
pancreatitis; vii) rare pancreatic calcification;
viii) rare pancreatic cysts; ix) occasional
association with other lesions such as
diabetes, sclerosing cholangitis similar to
primary sclerosing cholangitis (PSC), sialoadenitis, interstitial nephritis and
retroperitoneal fibrosis, and x) effective
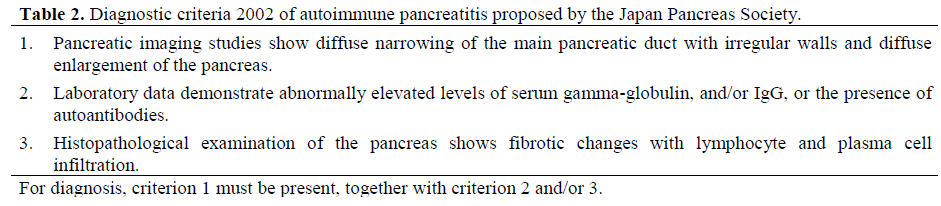
steroid therapy (Table 1). Recently,
“Diagnostic Criteria for Autoimmune
Pancreatitis 2002” containing three criteria,
pancreatic imaging, laboratory data, and
histopathological findings has been proposed
by the Japan Pancreas Society (Table 2) [3].
The occasional coexistence of pancreatitis
with other systemic exocrinopathies, bile
ductal lesions, and diabetes mellitus (DM)
have led to the concept of "a complex
syndrome" [4], "dry gland syndrome" [5] and
"autoimmune exocrinopathy”. Other names
such as "chronic inflammatory sclerosis of the
pancreas", "lymphoplasmacytic sclerosing
pancreatitis" (LPSP), "pancreatitis showing
the narrowing appearance of the pancreatic
duct" (PNPD), "pseudotumor of the
pancreas", "tumefactive chronic pancreatitis",
and "IgG4 related autoimmune disease" have
been proposed for cases similar to AIP [18, 19]. Recently, histological findings such as
LPSP are thought to be extremely similar to
AIP [18].
Associated Lesions (Table 3)
Patients with AIP often show bile duct lesions
such as intra-pancreatic stenosis or a sclerotic
appearance of the extra-pancreatic bile duct similar to PSC. Unlike PSC, biliary lesions in
AIP usually improve by administering
steroids, which suggests that the mechanism
of the development of biliary lesions in AIP
may be different from typical PSC. DM is
often (43-68%) observed in AIP and the
majority of patients have type II DM; some
improve after steroid therapy. Although the
mechanism is obscure, cytokines from T cells
and macrophages suppressing the function of
islet beta-cells may be down-regulated by
steroids. Eleven of our 30 cases did not have
any other lesions, while 19 patients with AIP
had one or more associated lesions. Fifteen
patients (50%) had diabetes, 8 sclerosing
cholangitis (27%), 6 rheumatoid arthritis
(23%), 5 sialoadenitis (17%), 3 renal
dysfunction (10%), and 3 retroperitoneal
fibrosis (10%). It has been noted that there is
a possibility of development of other
complications even in the patients diagnosed
as having only pancreatitis [10].

Histopathology
Microscopic findings in AIP are consistent
with lymphoplasmacytic sclerosing
pancreatitis as previously reported by
Kawaguchi et al. [6]: i) diffuse
lymphoplasmacytic infiltration with
pronounced acinar atrophy; ii) marked fibrosis of the contiguous soft tissue as well
as the total pancreas similar to retroperitoneal
fibrosis; iii) obliterated phlebitis in
and around the pancreas involving the portal
vein; iv) inflammatory wall thickness of the
common bile duct (CBD) and gallbladder;
and v) the minor salivary gland in the lip
biopsy having inflammation similar to the
pancreatic lesion or Sjögren's syndrome. In
addition to these findings, in AIP, T-cells,
which are usually HLA-DR+ CD4+ or HLADR+
CD8+ cells, predominantly infiltrate
around the pancreatic duct over B cells
(Figure 1) [10]. Although the mechanism is
still unclear, the histological differences
between lymphoplasmacyte and T cell
dominance may suggest the different stages of
the diseases.
Figure 1. Immunohistochemistry of the pancreas in
autoimmune pancreatitis. Immunohistochemistry
showed T-cells mainly infiltrated around the pancreatic
duct (x 250). a. pan T cells (pancreatic duct); b. pan B
cell (pancreatic duct); c. pan T cell (intra-pancreatic
bile duct); d. pan B cell (intra-pancreatic bile duct).
Clinical Symptoms
Patients with AIP usually have no or only
slight discomfort in the epigastrium or back,
and symptoms related to other associated
diseases [2, 3, 4, 5, 6, 7, 8, 9, 10, 11, 12, 13, 14, 15, 16]. The clinical symptoms are different
from those in the cases of acute or severe
pancreatitis. In our 30 patients, 19 patients
had jaundice (63%), 8 had abdominal pain
(27%), and 6 had back pain (20%).
Obstructive jaundice due to the stenosis of the
CBD or sclerosing cholangitis is characteristic
in AIP as compared to other types of
pancreatitis. Steroid therapy is usually
effective for stenosis of the bile duct
associated with AIP and improves clinical and
laboratory findings [9, 10, 11, 12, 13].
Pancreatic and Biliary Imaging
Computed tomography (CT), magnetic
resonance imaging (MRI) or ultrasonography
(US) show the diffusely enlarged pancreas
with its so called "sausage-like" appearance
(Figure 2), and a capsule-like rim which
appears to have low density on CT and to be
hypo-intense on T2-weighted MR images,
and shows delayed enhancement on dynamic
MR imaging [20, 21]. Pancreatic calcification
or pseudocyst is seldom observed. F-18 fluoro-2-deoxy-D-glucose (FDG)-positron
emission tomography (PET) shows
accumulative signals in the pancreatic lesions
similar to the imaging of pancreatic cancer
[22]. ERCP images in the AIP patients show
segmental or diffuse narrowing of the main
pancreatic duct (Figure 3) [9, 10, 11, 12, 13, 14]. On the other hand, the pancreas often
shows atrophic changes after steroid
treatment. This may be due to the
improvement of pancreatic edema with acinar
atrophy. Although magnetic resonance
cholangio-pancreatography (MRCP) does not
adequately show the narrowing or stenosis of
the pancreatic duct, it can well demonstrate
images of the CBD. Patients with AIP often
show stenosis of the intra-pancreatic CBD resulting in dilatation of the upper-stream and.
the sclerosing stenosis of the extra-pancreatic
CBD similar to primary sclerosing cholangitis
(PSC) [14]. Steroid therapy in AIP is usually
effective for the stenosis of CBD as well as
the pancreatic duct [13, 14], while it is not
very effective for classic PSC [23]. These
findings suggest that the stenotic mechanism
of CBD in AIP may be different from that in
classic PSC.
Figure 2. Computed tomography of the pancreas. The
CT image shows the diffusely enlarged pancreas with
its so-called "sausage-like" appearance before
treatment.
Figure 3. ERCP images of autoimmune pancreatitis
and effects of steroid therapy. Both the narrowing main
pancreatic duct and intra-pancreatic common bile duct
improved one month after steroid therapy.
Laboratory Data (Figures 4 and 5)
Patients with AIP usually show increased
pancreatic enzymes, gamma-globulin, IgG
especially the IgG4 subtype [24], several autoantibodies such as antinuclear antibody
(ANA), anti-lactoferrin antibody (ALF), anticarbonic
anhydrase-II antibody (ACA-II),
rheumatoid factor and anti-smooth muscle
antibody [25]. Patients with jaundice or
stenosis of the CBD show abnormal levels of
serum bilirubin and hepatobiliary enzymes. In
these cases, other liver diseases such as viral
hepatitis, autoimmune hepatitis or PBC
should be differentiated from AIP. The
laboratory data of our 30 cases showed an
increase in serum hepatic, biliary and
pancreatic enzymes, and total bilirubin in 22
(73%), 25 (83%), 19 (63%) and 16 (53%)
patients, respectively. The pancreatic exocrine
function was slightly or moderately abnormal.
Seventeen of our 30 patients showed
hypofunction (58%) using an N-benzoyl-Ltyrosyl-
para-aminobenzoic acid (BT-PABA)
exocrine test. Most cases of diabetes mellitus
were type II, not insulin dependent (NIDDM)
but not type Ia, insulin dependent (IDDM)
[26, 27]. After steroid therapy, many
abnormal laboratory findings were reversible
and many cases of DM were brought under
control using steroid therapy [10, 11, 12, 13, 14, 26, 27].
Figure 4. Laboratory data in 30 patients with
autoimmune pancreatitis. The laboratory data of our 30
cases showed the increase of serum hepatic, biliary and
pancreatic enzymes, and total bilirubin in 22 (73%), 25
(83%), 19 (63%) and 16 (53%) patients, respectively.
Seventeen of our 30 patients showed hypofunction
(58%) by N-benzoyl-L-tyrosyl-para-aminobenzoic acid
(BT-PABA) exocrine test.
Figure 5. Autoantibodies in 30 patients with
autoimmune pancreatitis. Of 30 patients, ANA was
detected in 75%,, ALF in 75%, ACA-II in 55%, RF in
25% and ASMA in 15%. However, AMA was absent
in all cases.
Pathophysiology of AIP
Humoral Immunity and Target Antigens
The occasional coexistence of pancreatitis
with other lesions suggests that there may be
common target antigens in the pancreas and
other exocrine organs such as the salivary
gland, biliary tract and renal tubules. We
identified several autoantibodies such as
antinuclear antibody (ANA), anti-lactoferrin
(LF) antibody (ALF), and anti-carbonic
anhydrase-II (CA-II) antibody (ACA-II) by
using the patient’s serum and expression
vector encoding human pancreatic cDNA
[25]. Lactoferrin and CA-II are distributed in
the various human tissues, including the
lactating breast, bronchial, salivary and
gastric glands, the pancreas and renal tubules
[28]. We used animal models of autoimmune
pancreatitis along with sialoadenitis and
cholangitis using neonatally thymectomized (nTx) mice immunized with LF or CA-II and
nude mice transferred with lymphocytes
prepared from nTx mice [29]. The high
prevalence of these auto-antibodies in animal
models suggest that CA-II and LF may be the
candidates for target antigens in AIP.
However, it is noted that these antibodies are
not necessarily specific for AIP because
ACA-II can be detected in some patients with
SjS or systemic lupus erythematosus [30], and
ALF in ulcerative colitis or PSC [31].
Although the majority of patients with AIP
show increased levels of IgG, especially the
IgG4 subtype [24], the roles of IgG4 in AIP
are still unclear. The majority of cases of
diabetes mellitus associated with AIP show
type II diabetes, while 10% of patients with
diabetes mellitus show autoimmune diabetes
(type Ia) due to the presence of autoantibodies
against glutamic acid decarboxylase, insulin,
or tyrosine phosphatase-like protein [13].
Interestingly, anti-CA-II and anti-LF are often
observed in type I diabetes.
Cellular Immunity and Effector Cells
The role of the effector cells in AIP has been
poorly understood. The activated CD4+ and
CD8+ T-cells bearing HLA-DR and CD45RO
were elevated in the peripheral blood
lymphocytes (PBLs) as well as in the
pancreas in AIP as compared to other causes
of pancreatitis such as alcoholic or gallstonerelated
pancreatitis [10, 25]. CD4+ T-cells are
further subdivided into Th1 and Th2 cells
based on profiles of cytokine production, and
these two T-cell populations counterregulate
each other [32]. Thl cells, which produce IL-
2, tumor necrosis factor (TNF)-a and IFN-g,
mediate cellular immunity, macrophage
activation, cytotoxicity and facilitate B cell
production of opsonizing and complementfixing
antibodies. In contrast, Th2 cells,
which produce IL-4, 5, 6 and 10, promote
humoral and allergic responses [32]. Similar
to SjS or PSC, CD4+ T-cells showing the Th1
type of immune response are predominantly
involved in the development of AIP as
effector cells over Th2 type CD4+ T-cells
[24]. Similarly, Th1 immune response is involved in the development of pancreatitis
and sialoadenitis in animal models. In some
patients with AIP, HLA-DR antigens are
expressed on the pancreatic duct cells as well
as CD4+ T-cells [10, 31, 32]. However, there
is also a possibility that CD8+ T-cells may be
effector cells, because HLA-DR+CD8+ Tcells
as well as CD4+ T-cells increased in
PBLs and infiltrated the pancreas in patients
with AIP [25].
Treatment and Prognosis
In AIP patients with mild symptoms, the
usual treatment for acute pancreatitis such as
fasting, protease inhibitors and antibiotics is
not necessarily required. In cases of jaundice,
percutaneous transhepatic or endoscopic
retrograde biliary drainage is often needed,
especially with the complication of bacterial
infection. Steroid therapy is usually effective
for bile duct and salivary lesions as well as
pancreatic duct lesions [9, 10, 11, 12, 13, 14, 18]. It has been noted that some patients may
spontaneously improve without any treatment
[14]. Some patients associated with type II
diabetes mellitus may improve after steroid
therapy [13]. In the cases of bile duct lesions
without response to steroid therapy, surgery is
often necessary in order to differentiate them
from a malignancy as well as for relieving the
symptoms [14]. Twenty-one of our 30
patients were treated successfully with
prednisolone, two with pancreatectomy, and
four without medication. The long-term
prognosis of AIP is unknown. As the clinical
and laboratory findings of most cases are
reversible after steroid therapy [13, 14, 28],
the prognosis of AIP may depend on the
severity of the complications such as other
autoimmune diseases or diabetes mellitus.
Conclusion
In summary, recent studies support the
concept of autoimmune pancreatitis, which
appears to be a unique clinical entity.
Histopathologically, AIP is similar to LPSP
showing fibrosis, infiltration of lymphocytes
and plasmacytes, and obliterative phlebitis in the pancreas; major lymphocytes infiltrating
around the pancreatic duct are T cells.
Although the pathogenesis of AIP is still
unknown, several hypotheses have been
proposed from the clinical and animal
experimental aspects. The first step in the
disease may be an antigenic alteration at the
pancreatic duct or acinar cells such as an
aberrant expression of HLA-DR. Although
the long-term prognosis of AIP is unknown,
the clinical and laboratory findings of most
cases are reversible after steroid therapy.
Acknowledgments This study was supported
by Grant-in-Aid for Scientific Research of the
Ministry of Culture and Science of Japan
16590645
References
- Steer ML, Waxman I, Freedman S. Chronic
pancreatitis. N Engl J Med 1995; 332:1482-90. [PMID
7739686]
- Sarles H, Sarles JC, Camatte R, Muratore R, Gaini
M, Guien C, et al. Observation on 205 confirmed cases
of acute pancreatitis, recurring pancreatitis, and chronic
pancreatitis. Gut 1965; 6:545-59. [PMID 5857891]
- Japan Pancreas Society. Diagnostic criteria for
autoimmune pancreatitis by the Japan Pancreas Society
(2002). J Jpn Pancreas Soc 2002; 17:585-7.
- Montefusco PP, Geiss AC, Bronzo RL, Randall S,
Kahn E, McKinley MJ. Sclerosing cholangitis, chronic
pancreatitis, and SjS: A syndrome complex. Am J Surg
1984; 147:822-6. [PMID 6731702]
- Epstein O, Chapman RW, Lake-Bakaar G, Foo
AY, Rosalki SB, Sherlock S. The pancreas in primary
biliary cirrhosis and parimary sclerosing cholangitis.
Gastroenterology 1982; 83:117-82. [PMID 7129026]
- Kawaguchi K, Koike M, Tsuruta K, Okamoto A,
Tabata I, Fujita N. Lymphoplasmacytic sclerosing
pancreatitis with cholangitis: A variant primary
sclerosing cholangitis extensively involving pancreas.
Hum Pahtol 1991; 22:387-95. [PMID 2050373]
- Etemad B, Whitcomb DC. Chronic pancreatitis:
diagnosis, classification, and new genetic
developments. Gastroenterology 2001; 120:682-707.
[PMID 11179244]
- Lankisch PG, Koop H, Seelig R, Seelig HP.
Antinuclear and pancreatic acinar cell antibodies in
pancreatic disease. Digestion 1981; 21:65-8. [PMID
6971769]
- Yoshida K, Toki F, Takeuchi T, Watanabe S,
Shiratori K, Hayashi N. Chronic pancreatitis caused by
autoimmune abnormality. Proposal of concept of
autoimmune pancreatitis. Dig Dis Sci 1995; 40:1561-8.
[PMID 7628283]
- Ohana M, Okazaki K, Hajiro K, Kobashi Y.
Multiple pancreatic masses associated with
autoimmunity. Am J Gastroenterol 1998; 93:99-102.
[PMID 9448184]
- Horiuchi A, Kaneko T, Yamamura N, Nagata A,
Nakamura T, Akamatsu T, et al. Autoimmune chronic
pancreatitis simulating pancreatic lymphoma. Am J
Gastroenterol 1996; 91:2607-9. [PMID 8946997]
- Horiuchi A, Kawa S, Akamatsu T, Aoki Y,
Mukawa K, Furuya N, et al. Characteristic pancreatic
duct appearance in autoimmune chronic pancreatitis: a
case report and review of the Japanese literature. Am J
Gastroenterol 1998; 93:260-3. [PMID 9468255]
- Ito T, Nakano I, Koyanagi S, Miyahara T, Migita
Y, Ogoshi K, et al. Autoimmune pancreatitis as a new
clinical entity. Three cases of autoimmune pancreatitis
with effective steroid therapy. Dig Dis Sci 1997;
42:1458-68. [PMID 9246047]
- Uchida K, Okazaki K, Konishi Y, Ohana M,
Takakuwa H, Hajiro K, Chiba T. Clinical analysis of
autoimmune-related pancreatitis. Am J Gastroenterol
2000; 95:2788-94. [PMID 11051349]
- Coll J, Navarro S, Tomas R, Elena M, Martinez E.
Exocrine pancreatic function in Sjogren syndrome.
Arch Intern Med 1989; 149:848-52. [PMID 2784958]
- Sheikh SH, Shaw-Stiffel TA. The gastrointestinal
manifestations of Sjögren's syndrome. Am J
Gastroenterol 1995; 90:9-14. [PMID 7801957]
- Waldram R, Kopelman H, Tsantoulas D, Williams
R. Chronic pancreatitis, sclerosing cholangitis, and
sicca complex in two siblings. Lancet 1975; 7906:550-
2. [PMID 47019]
- Pearson RK, Longnecker DS, Chari ST, Smyrk
TC, Okazaki K, Frulloni L, Cavallini G. Controversies
in clinical pancreatology: autoimmune pancreatitis:
does it exist? Pancreas 2003, 27:1-13. [PMID
12826899]
- Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike
M, Tsuruta K, et al. A new clinicopathological entity of
IgG4-related autoimmune disease. J Gastroenterol
2003; 38:982-4. [PMID 14614606]
- Irie H, Honda H, Baba S, Kuroiwa T, Yoshimitsu
K, Tajima T, et al. Autoimmune pancreatitis: CT and
MR characteristics. AJR Am J Roentgenol 1998;
170:1323-7. [PMID 9574610]
- Furukawa N, Muranaka T, Yasumori K,
Matsubayashi R, Hayashida K, Arita Y. Autoimmune
pancreatitis: radiologic findings in three histologically
proven cases. J Comput Assist Tomogr 1998; 22:880-3.
[PMID 9843225]
- Nakamoto Y, Sakahara H, Higashi T, Saga T, Sato
N, Okazaki K, et al. Autoimmune pancreatitis with F-
18 fluoro-2-deoxy-D-glucose PET findings. Clin Nucl
Med 1999; 24:778-80. [PMID 10512104]
- Angulo P, Lindor KD. Primary sclerosing
cholangitis. Hepatology 1999; 30:325-32. [PMID
10385674]
- Hamano H, Kawa S, Horiuchi A, Unno H, Furuya
N, Akamatsu T, et al. High serum IgG4 cncentrations
in patients with sclerosing pancreatitis. N Engl J Med
2001; 344:732-8. [PMID 11236777]
- Okazaki K, Uchida K, Ohana M, Nakase H, Uose
S, Inai M, et al. Autoimmune-related pancreatitis is
associated with autoantibodies and Th1/Th2-type
cellular immune response. Gastroenterology 2000;
118:573-81. [PMID 10702209]
- Tanaka S, Kobayashi T, Nakanishi K, Okubo M,
Murase T, Hashimoto M, Takeuchi K. Corticosteroidresponsive
diabetes mellitus associated with
autoimmune pancreatitis. Lancet 2000; 356:910-1.
[PMID 11036899]
- Eisenbarth GS. Type I diabetes mellitus: a chronic
autoimmune disease. N Engl J Med 1986; 314:1360-8.
[PMID 3517648]
- Masson PL, Heremans JF. New data on lactoferrin,
the iron-binding protein of secretion. In: Protides of
Biological Fluids. Peters H, Eds. Oxford: Pergamon
Press, 1968:633-8.
- Uchida K, Okazaki K, Nishi T, Uose S, Nakase H,
Ohana M, Matsushima Y, Omori K, Chiba T.
Experimental immune-mediated pancreatitis in
neonatally thymectomized mice immunized with
carbonic anhydrase II and lactoferrin. Lab Invest 2002 ;
82:411-24. [PMID 11950899]
- Inagaki Y, Jinno-Yoshida Y, Hamasaki Y, Ueki H.
A novel autoantibody reactive with carbonic anhydrase
in sera from patients with systemic erythematosus and
Sjogren's syndrome. J Dermatol Sci 1991; 2:147-54.
[PMID 1908698]
- Peen E, Almer S, Bodemar G, Ryden BO, Sjolin
C, Tejle K, Skogh T. Anti-lactoferrin antibodies and
other types of ANCA in Crohn’s disease, ulcerative
colitis, and primary schlerosing cholangitis. Gut 1993;
34:56-62. [PMID 8432453]
- De Carli M, D'Elios MM, Zancuoghi G,
Romagnani S, Del Prete G. Human Th1 and Th2 cells:
functional properties, regulation of development and
role in autoimmunity. Autoimmunity 1994; 18:301-8.
[PMID 7858116]






