Raffaele Pezzilli1, Riccardo Casadei2, Lucia Calculli3, Donatella Santini4
Departments of 1Internal Medicine, 2Surgery, 3Radiology, and 4Pathology,
Sant'Orsola-Malpighi Hospital. Bologna, Italy
- *Corresponding Author:
- Raffaele Pezzilli
Department of Internal Medicine
Sant’Orsola-Malpighi Hospital Via Massarenti
9 40138 Bologna,
Italy
Phone +39-051.636.4148
Fax +39-051.549.653
E-mail pezzilli@aosp.bo.it
Received October 18th, 2004 - Accepted October 28th, 2004
Keywords
Autoimmune Diseases; Biological Markers; Tomography, Spiral Computed; Diagnosis, Differential; Magnetic Resonance Imaging; Pancreatitis; Pancreatic Neoplasms; Ultrasonography
INTRODUCTION
Autoimmune pancreatitis is a rare but fascinating type of chronic pancreatitis and an increasing number of cases are being reported from Japan and Europe [1]. Patients with autoimmune pancreatitis rarely complain of the typical severe abdominal pain of pancreatitis and usually arrive at the hospital due to painless jaundice [2]; other symptoms of autoimmune pancreatitis include nonspecific mild abdominal pain and weight loss. There is no laboratory hallmark of the disease, even if cholestatic profiles of liver dysfunction with only mild elevations of amylase and lipase levels have been reported [3]. We report a case which was suspected of being pancreatic cancer but which revealed histologic evidence of autoimmune pancreatitis.
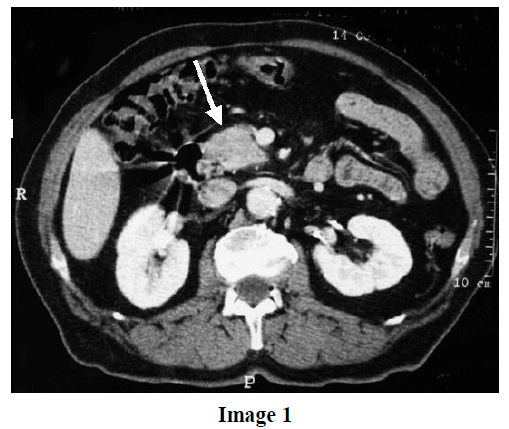
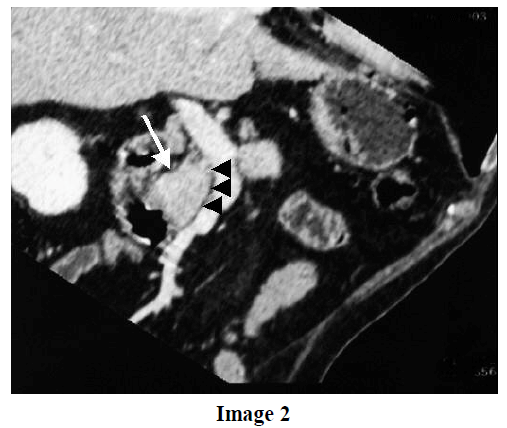
A 68-year old male was admitted to our Department because of asthenia and weight loss (about 8 kg in 2 months). He was a light drinker (he started to drink 40 g of pure alcohol per day at the age of 18 years) and a heavy smoker (he started to smoke 30 cigarettes per day at the age of 18 years). At the age of 45, he underwent a left colectomy for the perforation of a diverticulum; at the age of 48, he was found to be affected by arterial hypertension and was treated with ACE-inhibitors and beta-blockers); finally, at the age of 53, he was operated on for carcinoma of the prostate. He underwent a colonoscopy one month before admission which showed colonic diverticula of the right and transverse colon. On admission, physical examination was unremarkable. The laboratory examination revealed normal values of white blood cell count, hemoglobin, mean cellular volume, hematocrit, and platelet count. The renal and hepatic functions were also normal. Plasma glucose was 2.12 g/L (reference range: 0.60-1.10 g/L), plasma Cpeptide 0.8 ng/mL (reference range: 0.8-3.9 ng/mL), glycosylated A1 hemoglobin was 10% (reference range: 4.3-5.9%). Serum amylase was normal and pancreatic isoamylase slightly abnormal (117 U/L, reference range: 17-115 U/L). The serum carcinoembryonic antigen was normal, whereas serum CA 19-9 was 97 U/mL (reference range: 0-37 U/mL). Non-organ and organ specific autoantibodies were negative, and there was no hypergammaglobulinemia or elevated levels of serum IgG. An abdominal ultrasonography showed a hypoechogenic mass having a diameter of 24x19 mm localized in the pancreatic head with a normal main pancreatic duct. Since pancreatic cancer was suspected, an abdominal CT was carried out. This examination showed a nonhomogeneous mass in the head of the pancreas (Image 1) without surrounding tissue infiltration, and the cleavage between the mass (Image 2; white arrow) and the mesenteric vein was preserved (Image 2; head arrows). The main pancreatic duct was normal and no liver alterations were detected at CT scan. A multiplanar reconstruction image showed no infiltration of the peripancreatic vascular vessels by the pancreatic mass (Image 3).

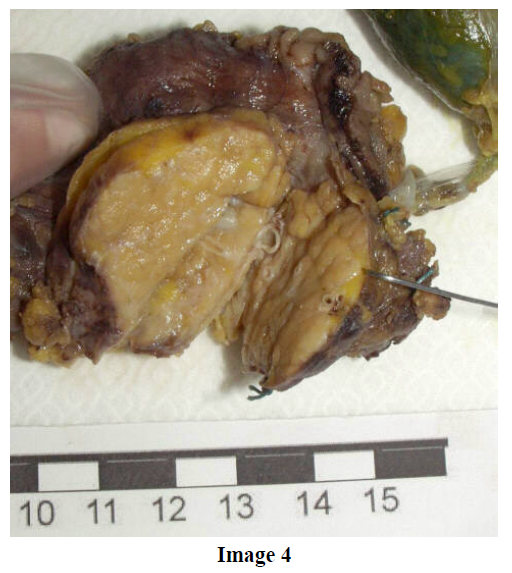
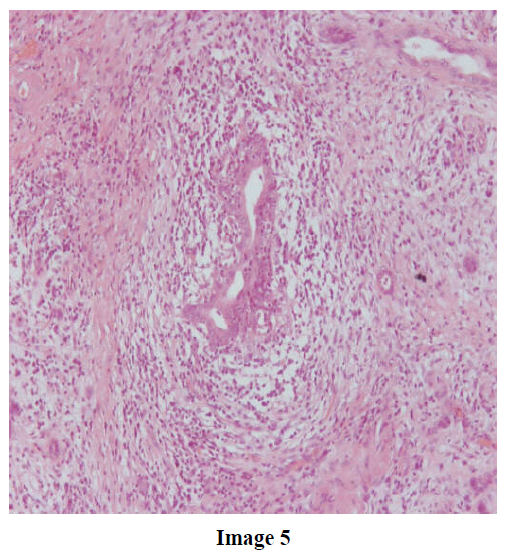
Fine needle aspiration of the lesion was carried out, but the specimen obtained was not sufficient for cytological examination; thus, the patient underwent a surgical procedure which consisted of a pyloruspreserving pancreaticoduodenectomy and a regional lymphadenectomy (Image 4). The histological examination showed a picture compatible with autoimmune pancreatitis: inflammatory infiltrates concentrated around the duct (Image 5; H&E, original magnification 20x), peri-phlebitis in the pancreatic and peripancreatic tissue (Image 6; H&E, original magnification 20x), and ductocentric lymphoplasmacytic infiltrates with germinal centres and dense interstitial fibrosis (Image 7; H&E, original magnification 20x).


Recovery was uneventful and the patient remains symptom-free.
Autoimmune pancreatitis is resolved with steroids, so clinical identification of the disease is very important from a clinical point of view; however, its diagnosis is still a challenge [4].
One of the most important criteria seems to be the clinical association with other postulated autoimmune diseases of the gastrointestinal tract (such as primary sclerosing cholangitis, primary biliary cirrhosis, ulcerative colitis, Crohn’s disease and Sjögren’s syndrome) [5], but these diseases were not present in our case.
Other biochemical criteria such as the presence of non-organ specific autoantibodies at high titer (anti-nuclear, anti-mitochondria, anti-smooth muscle, anti-neutrophil cytoplasmic), were absent in our patient; normal IgG levels were present. Antibodies to carbonic anhydrase types I and II were not carried out because they are not available in our laboratory, even if their presence could be useful in identifying autoimmune disease of the pancreas.
In our patient, the elevation of CA 19-9 serum levels together with the presence of a mass localized at the head of the pancreas, were considered signs compatible with pancreatic cancer and, for this reason, we operated on the patient. Even if abnormal values of the tumor marker CA 19-9 have been previously reported in about 50% of patients with autoimmune pancreatitis [6, 7], in our patient there were no other biochemical and imaging signs compatible with the diagnosis of autoimmune pancreatitis. Unfortunately, cytology obtained by fine needle aspiration was not diagnostic. Thus, the possibility of autoimmune pancreatitis was not taken into account before the surgical procedure. We should also point out that, even if magnetic resonance cholangio-pancreatography is recommended for the differential diagnosis between autoimmune pancreatitis and pancreatic cancer by detecting stenosis or the narrowing of the pancreatic ducts, in our case, this examination was not carried out because of the presence of a normal caliber of the main pancreatic duct at ultrasonography and CT. Finally, our clinical decision to operate on the patient was taken because the risk of under-diagnosing a pancreatic cancer was higher than that of considering the patients affected by autoimmune pancreatitis.
In conclusion, the case reported represents an example of one of those rare cases in which the differential diagnosis between autoimmune pancreatitis and pancreatic cancer using the commonly accepted criteria is very difficult. Thus, we should be aware that, even if the diagnosis of fully-manifested autoimmune pancreatitis is easy when at least one of the usually reported diagnostic criteria is present [5], in some cases, the diagnosis is more difficult and may be obtained only surgically.
References
- Pearson RK, Longnecker DS, Chari ST, Smyrk TC, Okazaki K, Frulloni L, Cavallini G. Controversies in clinical pancreatology: autoimmune pancreatitis: does it exist? Pancreas 2003; 27:1-13. [PMID 12826899]
- Okazaki K, Chiba T. Autoimmune related pancreatitis. Gut 2002; 51:1-4. [PMID 12077078]
- Kamisawa T, Funata N, Hayashi Y, Tsuruta K, Okamoto A, Amemiya K, et al. Close relationship between autoimmune pancreatitis and multifocal fibrosclerosis. Gut 2003; 52:683-7. [PMID 12692053]
- Kim KP, Kim MH, Lee SS, Seo DW, Lee SK. Autoimmune pancreatitis: it may be a worldwide entity. Gastroenterology 2004; 126:1214. [PMID 15057766]
- Cavallini G, Frulloni L. Autoimmunity and chronic pancreatitis: a concealed relationship. JOP. J Pancreas (Online) 2001; 2:61-8. [PMID 11867865]
- Akashi T, Oimomi H, Nishiyama K, Nakashima M, Arita Y, Sumii T, et al. Expression and diagnostic evaluation of the human tumor-associated antigen RCAS1 in pancreatic cancer. Pancreas 2003; 26:49-55. [PMID 12499917]
- Kamisawa T, Egawa N, Nakajima H, Tsuruta K, Okamoto A, Kamata N. Clinical difficulties in the differentiation of autoimmune pancreatitis and pancreatic carcinoma. Am J Gastroenterol 2003; 98:2694-9. [PMID 14687819]

