Keywords
Diabetes Mellitus, Experimental; Glucose Tolerance Test; Histology; Image Cytometry; Immunocytochemistry; Insulin; Metabolism; Postoperative Care; Streptozocin; Transplantation
Abbreviations
BGC: blood glucose concentration; IVGTT: intravenous glucose tolerance test; SD: Sprague-Dawley
INTRODUCTION
Embryogenesis of the pancreas in a laboratory rat has been shown to occur in two distinct stages. The first ensures the existence of a primarily endocrine structure at day 16 postcoitum. Rapid exocrine proliferation occurs after day 16 to produce an organ which approximates the 1:99 percent ratio of endocrine to exocrine tissue found in the juvenile at one month and in the adult [1, 2, 3, 4, 5, 6].
For a number of reasons, the endocrine nature of the 16 day post-coitum pancreas (foetal pancreas) has proved to be a useful medium for reversing chemically induced diabetes mellitus when transplanted beneath the renal capsule [7]. First, the foetal pancreas has been shown to have a substantial capacity for the growth and differentiation of beta-cells, to the point of being able to supply the insulin needs of diabetic adult transplant recipients (experience has shown that the harvesting of the pancreas after day 16 results in extensive development of the exocrine component of the pancreas followed by wide spread enzymatic damage to the recipient organ). Second, the size of the foetal pancreas facilitates rapid harvesting and transplantation, thus reducing cold ischaemic time. Penultimately, it appears to be less prone to attack by the immune system of the recipient thereby enhancing long-term graft survival and finally, the relative availability of foetal material for transplantation.
Our experimental laboratory has, for a number of years now, been involved in investigating the dynamics surrounding syngeneic/isogeneic and allogeneic foetal pancreas transplantation in a variety of normal and diabetic rat models with and/or without immune suppression [8, 9, 10, 11, 12]. Complete metabolic profiles (blood glucose concentration, water intake, urine excretion, body weight gain or loss, intravenous glucose tolerance test results, urine pH, urine glucose, ketones) histological examination and computerised morphometry have enabled us to evaluate the efficacy of graft survival and function [13].
Debate regarding the use of foetal tissue has, however, been ongoing, contentious and without any clear-cut resolution one way or the other. The few scientists entering the debate have called for decisions to be based on sound research principles, divorced from the emotionalism that usually surrounds the issue [14, 15, 16]. One can only assume that the relative reluctance to enter the debate is indicative of the general unwillingness to become involved in foetal tissue research. With this in mind, we deemed it appropriate to explore alternative sources with similar qualities to act as potential effective replacement organs for foetal tissue.
A recently completed study at our facility has demonstrated the emergence of highly proliferative pancreatic duct epithelial cells 3.5 days after ligation of the pancreatic duct distal to its confluence with the common bile duct [17]. Apoptosis was shown to be responsible for total acinar deletion by day 3 post-ligation. Duct epithelial cells, testing insulin positive during immunocytochemical/ histologic investigation - in the absence of acinar tissue, developed into an essentially endocrine organ with an insulin positive content of 11.5% of the residual tissue volume. Cell proliferation indices approximated increases found in similar studies [2, 18, 19, 20, 21].
The aim of this study was to assess the efficacy of 3.5 day post-pancreatic duct ligation transplanted tissue fragments in reversing the metabolic profile of chemically induced diabetes mellitus in a laboratory rat model.
MATERIALS AND METHODS
Laboratory Animals
Thirty normal three-month-old Sprague- Dawley (SD) laboratory rats were obtained from the central breeding facility at this university. After acclimatization, they were randomly divided into 5 groups of six animals each which were designated as A, B, C, D, and E, respectively. The experimental animals (Group A: transplant recipients; Group B: untreated diabetic) received 60 mg/kg streptozotocin (Sigma, St Louis, USA. Product Catalogue no S0130) dissolved in saline (SABAX, Port Elizabeth, South Africa) via a tail vein under intraval sodium (Thiopentone Sodium, Rhône-Poulenc Animal Health Pty. Ltd., Midrand, South Africa) general anaesthesia. At day 3.5, the Group A animals underwent transplantation and, at day 30, a nephrectomy had been performed in these animals. Groups B and C served as untreated controls: diabetic and normal controls, respectively. Group D underwent midline laparotomy only and served as sham operated controls while Group E underwent pancreatic duct ligation via a mid-line laparotomy and served as tissue donors.
Pancreatic Duct Ligation (Group E)
Anaesthetised rats were prepared for surgery by shaving the abdominal surface and thereafter cleaning it with Betadine antiseptic solution containing providone-iodine at 10 mg/mL (Adcock Ingram Pharmaceuticals, Industria, Johannesburg, South Africa). A short (2 cm) mid-line laparotomy incision extending from the xiphisternum was utilised to gain access to the abdominal cavity. After exposing and drawing out the pancreas, it was prised away from the surrounding tissue with blunt forceps. A single stitch of re-absorbable suture material (5/0 Dexon polycaprolate coated braided polyglycolic acid, Davis and Geck, Cyanamid, Hampshire, United Kingdom), was carefully placed at a point immediately distal to the confluence of the splenic and common bile ducts as described by the author [17]. This ligated the distal aspect of the duct affecting the tail portion of the pancreas, which accounted for between 50 and 60 percent of the entire organ.
After ligation, the abdomen was closed in layers as described below. Post-operatively the animals were housed in standard laboratory cages in a thermally controlled environment with free access to standard rat chow (Epol, Midrand, South Africa) and drinking water. Pethadine (Intramed, Port Elizabeth, South Africa) was administered every six hours as an analgesic under the supervision of a qualified vet.
Transplantation
After 84 hours (3.5 days), the rats having undergone pancreatic duct ligation (Group E) were sacrificed, their pancreas removed, trimmed of fat, mesenteric and normal tissue and placed in Roswell Park Memorial Institute media (RPMI 1640, Sigma 6504, Sigma-Aldrich, Atlasville 1465, South Africa) on ice until transplanted. After confirming whole blood glucose concentrations (BGC) of 20 mmol/L or greater, Group A animals were prepared for surgery as described above. A midline laparotomy incision was performed in the recipient rats and the kidney lifted into view. After exposing the kidney from the surrounding organs, a small incision, just deep enough to penetrate the capsule, was made and a subcapsular pocket prepared by gently separating the kidney capsule from the underlying cortex with a fine curved forceps. Bleeding was controlled by applying gentle pressure where necessary. The pocket was rinsed with sterile physiological saline (SABAX, Port Elizabeth, South Africa). Six to eight tissue fragments (1 mm3) of duct ligated tissue were placed beneath the renal capsule (Figure 1a). The kidney capsule was left unsutured and the kidney was allowed to return to its position. Before closing the abdomen, 5 mL of warm (±30 °C) sterile Ringers lactate (SABAX, Port Elizabeth, South Africa) was placed in the peritoneal cavity to prevent dehydration.
The laparotomy incision was sutured in two layers, first the peritoneum and muscle followed by the skin using 4/0 Dexon (Davis and Geck, Isando, South Africa). The wound was swabbed with Kleenwound foaming antiseptic spray (Beige Pharmaceuticals Pty. Ltd., Edenvale, South Africa) powdered with dry penicillin and sprayed with Spray Skin flexible plastic skin (Link Laboratories, Edenvale, South Africa).
Post-Operative Care
Post-operatively, the animals received 2.5 mg Amoxil (Smith-Kline Beecham Pharmaceuticals, Midrand, South Africa) and 0.5 mg streptomycin (Novo-Strep 5g/15 mL, Novo Nordisk Pty. Ltd., Johannesburg, South Africa) in a single dose, to guard against opportunistic infection, exogenous insulin (Humalog Mix25, Eli Lilly (S.A.) Pty. Ltd., Isando, Gauteng, South Africa) and pethidine HCl (0.25 mg) (Fresenius Kabi, Halfway House, South Africa) every six hours for the first 24 hours and every 8 hours thereafter for a another two days. The animals were returned to clean cages and housed in a thermally controlled environment with free access to water and standard rat chow (Epol, Midrand, South Africa). Blood glucose was maintained below 10 mmol/L by the subcutaneous administration of Humalog Mix25 (6.6 units/mL: 0.03 mL, equivalent to 0.198 units if BGC was greater than 20 mmol/L; 0.02 mL equivalent to 0.132 units if BGC ranged 15-20 mmol/L; 0.01 mL equivalent to 0.066 units if BGC ranged 10- 15 mmol/L).
Intravenous Glucose Tolerance Testing (IVGTT)
Glucose tolerance testing is a standard procedure used to assess pancreas beta-cell response to intravenous glucose load [22]. The ability of the beta cells to facilitate the removal of glucose via insulin mediated influx across plasma membranes and the subsequent intracellular conversion or utilization, is expressed in terms of the disappearance-rate (K-value) of glucose from the blood [23, 24, 25, 26, 27, 28].
Groups A, B, C and D underwent the first IVGTT on day 3.5 (after Groups A and B received 60 mg/kg i.v. streptozotocin as described above) under general anaesthesia (thiopentone sodium) given intraperitoneally. The IVGTT was repeated in these groups on day 30 (just prior to unilateral nephrectomy in Group A). In addition, IVGTT in Group A was also performed in Group A one week after the removal of the grafted tissue. Each rat received 1.0 g/kg 50% dextrose solution (Dextrose injection B.P. 50% m/v, 500 mL/mL, Adcock Ingram Laboratories Limited, Johannesburg, 2092, South Africa) as a single pulse over 30 seconds, i.v. via a lateral tail vein (method described below). Quoted experimental values range from 0.5 mg/kg [29], 0.5 g/kg [26, 27] to 1.5 g/kg [30].
The rats were placed on their side under a 60 W lamp for warmth (the heat causing vasodilatation). The hair at the base of the tail was shaved using a No. 23 scalpel blade, and a length of 2 mm plastic tubing was tied around the base of the tail (acting as a tourniquet), thus producing engorgement of the tail veins to facilitate venepuncture. The lateral vein was occluded by finger pressure ±3 cm below the knot. The protruding vein was then punctured from an oblique angle of ±10 degrees, using a 0.5 mm lymphangiocath (Beckton, Dickenson and Company, Rutherford, NJ, USA) needle, connected to a 1.0 mL tuberculin syringe.
After obtaining two basal blood samples from the tail, to determine fasting blood glucose level, 1.0 g/kg 50% dextrose solution was injected rapidly intravenously, via a lateral tail vein (described previously). Thereafter, blood specimens were taken at 1, 3, 5, 10, 15, 20, 25, 30, 45, 60, 90 and 120 minute intervals and analysed using a glucometer (Glucometer Elite, Bayer Pty. Ltd., Wrench Rd, Isando, 1600, South Africa).
Histological Evaluation of Transplanted Grafts
After IVGTT on day 30, Group A animals were anaesthetised and prepared for surgery, as described earlier, in order to harvest the grafts for histological assessment. The whole kidney was isolated and excised after ligation of the major blood vessels and fixed in 4% formaldehyde solution, transferred to the base of a labelled cassette, processed in an automated tissue processor and embedded in histological embedding wax (Paramat, BDH Laboratory Supplies, Poole, England). After a number of haematoxylin and eosine (H&E) stained trials to assess tissue composition, the tissue blocks were trimmed to remove excess kidney tissue, leaving only the grafts and a one to two millimetre strip of kidney tissue for comparison and further assessment.
Immunocytochemistry
Five series of two consecutive 3-6 μm sections from each animal 200 μm and apart as described by Rosenberg and Duguid [30], were stained for H&E and insulin (1/200 dilution using the Avidin-Biotin ABC Technique (Vectastain ABC Kit, Vector Laboratories, Burlingame, CA, USA), a method described by Geusdon et al. [31].
The substrate was prepared by mixing together equal volumes of 0.02% hydrogen peroxide, made in distilled water from a 30% stock, and 0.1% (1 mg/mL) diaminobenzidine tetrahydrochloride (DAB) (Sigma Fast, Sigma Chemical Company, Steinheim, Germany) made in 0.1 M Tris buffer, pH 7.2. The hydrogen peroxide solution should be freshly prepared from concentrated stock. Many peroxidase substrates are unstable in the presence of hydrogen peroxide or when exposed to light. For best results, the peroxidase substrate is made just prior to use. Paraffin sections were stained by first deparaffinising and hydrating tissue sections through xylene and graded alcohol series, and then rinsed for five minutes in distilled water. The sections were incubated in 0.3% H2O2 in methanol for 30 minutes to eliminate endogenous peroxidase activity. The sections were then washed in buffer for 20 minutes and then incubated for a further 20 minutes with diluted 1:50 normal goat serum; the excess serum blotted from the sections.
Sections were then incubated for 30 minutes with primary antiserum diluted in buffer (Table 1) and then washed for 10 minutes in buffer, after which they were incubated for 30 minutes with diluted biotinylated antibody solution and then washed for 10 minutes in buffer. A 30 minute incubation with Vectastain ABC was then required before another wash of 10 minutes in buffer. Sections were incubated for two to seven minutes in peroxidase substrate solution, washed for 5 minutes in tap water, counterstained with haematoxylin, cleared and mounted.
Antibody Specificity Controls
Method Controls
Method controls consisted of the omission of each stage, in turn of the labelling procedure.
Specificity Controls
Specificity controls included adsorption of the primary anti-sera with excess homologous or heterologous antigen (10-100 μg per mL diluted anti-serum) for 24 hours before immunolabelling. In the case of anti-sera to peptides sharing amino acid sequences, cross reactivity of the anti-sera was analysed by dot blotting and the results compared with tissue labelling, bearing in mind the different availability of epitopes between native antigen and antigen fixed in the tissue section.
Morphometry
Immunocytochemically (ICC) stained sections of the grafts were morphometrically assessed according to previously described methods [32, 33, 34] using a computerised system which consisted of a Pulnix TMC-6 CCD video camera (Total Turnkey Solutions, Mona Vale, Australia) on a standard Zeiss light microscope (Carl Zeiss Pty. Ltd., Randburg, South Africa) coupled with a DT 3153 MACH Series Frame Grabber graphics card (Agile Integration South Africa, Cape Town, South Africa) in a 486 PC. A HL Image ++ (image plus-plus) Windows 95 compatible software package (Western Vision Software, Salt Lake City, UT, USA) was used to capture and process microscopic images. Data was exported to MS Excel (Microsoft Inc., Johannesburg, South Africa) and processed through STATISTICA (Statsoft Inc, Tulsa, OK, USA).
Ten randomly selected tissue areas, totalling at least 105 μm2 from each specimen, where possible, were assessed. The immunoreactive areas for each were totalled and expressed as a percentage of the total area measured. Two further randomly selected areas for each slide were photographed for comparison and manually measured for control purposes and to determine islet size and frequency. Data obtained from ligated (Group A) and sham operated control (Group D) animals were compared with values from published literature [17].
ETHICS
This study was approved by the ethics committee of the University of Stellenbosch and has rigorously adhered to the ethical NIH guidelines for the care and use of laboratory animals.
STATISTICAL ANALYSIS
Data were analysed in MS Excel (Microsoft Inc., Johannesburg, South Africa) using the Student's t-test for independent samples and are reported as mean±SEM. Differences between experimental results were considered significant if P was less than 0.05.
RESULTS
Pre- and Post-Operative Blood Glucose Concentration (BGC)
Pre-streptozotocin BGC for all groups (A, B, C, D) was 5.2±1.4 mmol/L. Both experimental groups (A and B) presented with blood glucose levels of 20.0±3.7 mmol/L, 36 hours after streptozotocin administration (P<0.001 vs. rats in normal conditions). Blood glucose levels for transplant recipients (Group A) fluctuated through a wide range after transplantation primarily due to the administration of exogenous insulin while those for Group B remained unaltered as quoted above. Group A became less dependent on exogenous insulin over time. Insulin therapy ceased in three (50%) of these animals after 15 days post-transplantation (BGC <10 mmol/L) while it (insulin therapy) decreased by 50% in the remaining animals (untreated BGC between 10-15 mmol/L). Transplant recipients remained euglycaemic (BGC 6-10 mmol/L) following removal of the grafted tissue.
Intravenous Glucose Tolerance Testing
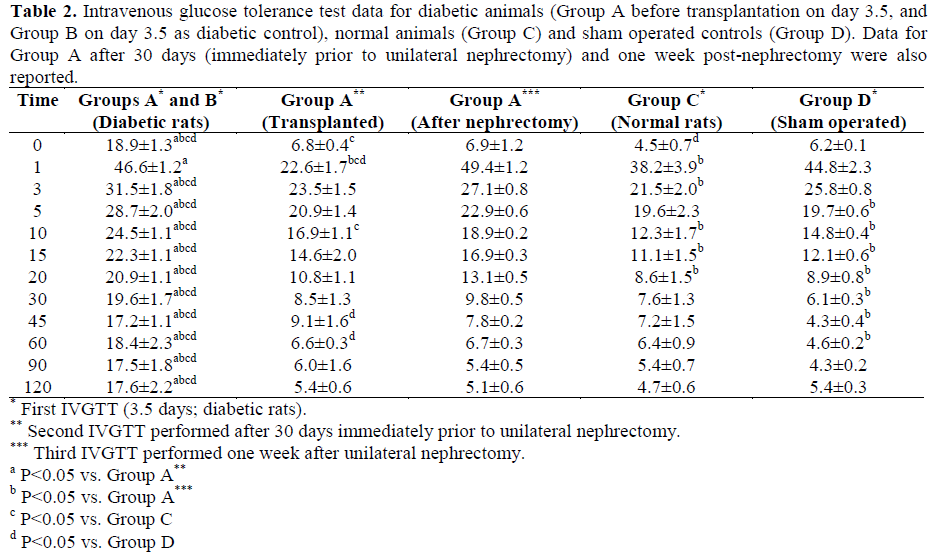
Pre-operative but post-streptozotocin intravenous glucose tolerance test results for Groups A and B, as well as thirty day posttransplantation intravenous glucose tolerance test values for Group A are presented in Table 2 and Figure 2.
K-Values
Mean K-values for normal controls (Group C) were 2.74±0.25 and for sham-operated controls (Group D) were 3.98±0.72 (P=0.135 vs. Group C) while those for Groups A and B pooled together were 1.28±0.86 (P=0.127 vs. Group C; P=0.029 vs. Group D). Postoperative values for the transplant recipients remained unchanged after a nephrectomy had been performed (3.01±0.23 both before and after nephrectomy; P=1.000). Significant differences were observed between shamoperated controls on the one side and experimental animals on the other.
Histology
On a macroscopic level, visual examination of the excised kidney revealed a barely discernable opaque layer on the ventral surface of the kidney, as illustrated in Figure 1b. Microtome sections along line B1/B2 on Figure 1b generally revealed a layer of tissue approximately 200 μm thick (morphometric assessment) consisting of ducts, ill-defined stroma and isolated cells, and small (3-8 cells) cell clusters ICC positive for insulin (Figure 3).
Figure 1. Position of engrafted material prior to
suturing (A) and post-nephrectomy (B).
Figure 2. Intravenous glucose tolerance test (IVGTT)
results for all experimental groups.
* First IVGTT (3.5 days; diabetic rats).
** Second IVGTT performed after 30 days immediately
prior to unilateral nephrectomy.
*** Third IVGTT performed one week after unilateral
nephrectomy.
**** Previously published data [13].
Figure 3. Immunocytochemical staining of grafted
pancreatic tissue (insulin positive).
Blue bar = 50 μm.
A: recipient kidney
B: transplanted pancreatic tissue
C: areas immunocytochemically positive for insulin
Morphometry
Analysis of insulin positive tissue ratio in 30 slides from each of the engrafted kidneys (total = 150) produced an average figure of 3.17±0.73% while that for the 150 recipient pancreases (without acinar tissue) was 0.50±0.25% (P<0.001 vs. engrafted kidneys).
DISCUSSION
The induction of diabetes mellitus using streptozotocin in laboratory animals has a proven dose related consistency. Severely diabetic animals (blood glucose >20 mmol/L), left untreated with exogenous insulin, rapidly deteriorated and succumbed to ketoacidosis; while those with mild diabetes (blood glucose between 10 and 20 mmol/L) developed retinopathy, nephropathy, lost weight and eventually succumbed to metabolic stress [11, 35]. Glucose tolerance testing of the first group (severely diabetic) produced a flat curve (K-value below 1.5) indicating a zero insulin response while the second group elicited a weak response (K-value between 1.5 and 2.5). These results concur with previously published findings [10, 11, 12, 13, 34].
Post-transplantation administration of exogenous insulin is presumed to protect the grafts from the vascular degenerative processes known to occur in blood vessels as a result of hyperglycaemia [5]. Poor posttransplantation insulin therapy is known to impact negatively on graft survival and/or the development of sustainable and viable islets [13, 26, 27], which would seem to suggest that graft survival could be subject to the maintenance of normoglycaemia (blood glucose level between 3 and 6 mmol/L). Whether euglycaemia, with blood glucose between 8 and 12 mmol/L would produce similar graft survival is open to speculation. It would appear as if the development of the secondary complications in diabetes mellitus could also be linked to large fluctuations (BGC 2-20 mmol/L, or greater) in blood glucose levels which in turn can be linked to poor insulin therapy. At this stage, it would seem that post-transplant insulin therapy, albeit poor, enhances graft survival and probably impacts on the quality of insulin response during the intravenous glucose tolerance test at day 30. These results compare favourably with previously published results on animals receiving no post-operative insulin therapy.
In spite of the problems experienced in postoperative diabetes management, 50% of the transplanted group showed a rapid return to normoglycaemia while the remainder of the group, although euglycaemic, did not exhibit the same degree of glucose management and tolerance. Factors influencing this phenomenon may be ascribed to non-specific and non-quantifiable mechanisms common in transplantation biology as graft failure, fibrosis, site diabetic exhaustion, ischaemia, enzymatic degradation before grafting, etc.
This model is encouraging for a number of reasons. First, as this model makes use of histocompatible tissue, the rejection response is low/zero and no immuno-suppression is required. Second, it offers an alternative source of donor tissue for transplantation into diabetic animals. Day 3.5 post duct ligation tissue is primarily an endocrine structure with an apparently high proliferative ability. Third, although only a limited number of animals were used, the incidence of total graft failure was zero while half of the experimental animals achieved normoglycaemic status and the remainder euglycaemic status. Penultimately, glucose tolerance testing produced results comparable with the established model utilizing foetal tissue as primary transplant organ, and finally, immunocytochemical analysis confirms the presence of viable functioning beta-cells.
CONCLUSION
Preliminary results seem to suggest that duct ligated tissue transplanted into the renal subcapsular space compares favourably with similar studies [10, 11, 12, 13] utilizing foetal pancreatic tissue as a donor organ. More comprehensive studies are however necessary to investigate this phenomenon especially in the long term. Duct ligation triggers neogenesis [20, 21] of the pancreas and further applications could be developed by harvesting duct ligated tissue, cryopreservation, inducing diabetes in the same animal and transplanting the frozen tissue back into the same animal.
References
- Bouwens L, Wang RN, De Blay E, Pipeleers DG, Kloppel G. Cytokeratins as markers of ductal cell differentiation and islet neogenesis in the neonatal rat pancreas. Diabetes 1994; 43:1279-83. [PMID 7523208]
- Bouwens L, Lu WG, De Krijger R. Proliferation and differentiation in the human fetal endocrine pancreas. Diabetologia 1997; 40:398-404. [PMID 9112016]
- Melmed RN, Benitez CJ, Holt SJ. Intermediate cells of the pancreas. I. Ultrastructural characterization. J Cell Sci 1972; 11:449-75. [PMID 4627700]
- Scaglia L, Cahill CJ, Finegood DT, Bonner-Weir S. Apoptosis participates in the remodeling of the endocrine pancreas in the neonatal rat. Endocrinology 1997; 138:1736-41. [PMID 9075738]
- McEvoy RC. Fetal rat pancreas in organ culture: effects of serum on the development of the endocrine cells. Differentiation 1980; 17:105-9. [PMID 6108888]
- McEvoy RC, Madson KL. Pancreatic insulin-, glucagon-, and somatostatin-positive islet cell populations during the perinatal development of the rat. II. Changes in hormone content and concentration. Biol Neonate 1980; 38:255-9. [PMID 6106512]
- du Toit D, Muller C, Page B, Louw J. Foetal rat pancreatic transplantation: posttransplantation development of foetal pancreatic iso- and allografts and suppression of rejection with mycophenolate mofetil (MMF) and cyclosporine based immunesuppression. Microsc Res Tech 1998; 43:347-55. [PMID 9849976]
- du Toit DF, Muller C, Mouton Y, Page B, Mattysen J, Lyners R, Woodroof C. Tacrolimus (FK506) monotherapy provides potent and significant suppression of allogeneic foetal rat pancreatic allograft rejection. Transplant Proc 1998; 30:4073-4. [PMID 9865300]
- du Toit DF, Muller C, Page B, Mattysen J, Lyners R. Immunosuppression with cyclosporin A in combination with mycophenolate mofetil suppresses rejection of allogeneic fetal rat pancreatic allografts. Transplant Proc 1998; 30:4092-3. [PMID 9865308]
- Muller CJ, Du Toit DF, Beyers AD, Page BJ, Muller N. Prolongation of rat fetal pancreas allograft survival using a nondepleting anti-CD4 monoclonal antibody W3/25. Transplant Proc 1998; 30:4180-3. [PMID 9865339]
- Muller CJ, du Toit DF, Page B, Louw J, Muller BJF, Williams K, Mattysen J, et al. Islet morphology and function following foetal rat pancreatic transplantation. Eur J Anat 2000; 4:149-60.
- Muller CJ, duToit DF, Page BJ, Muller N, Mattysen J, Lyners R. Efficacy of malononitrilamide 715 as immunosuppressant, alone or in combination with cyclosporin, in allogeneic foetal rat pancreatic transplantation. Transplant Proc 2001; 33:2229-31. [PMID 11377510]
- Page BJ. Autogenous Foetal Rat Pancreas Transplantation in Syngeneic Inbred Diabetic Rats. Tygergerg, South Africa: Stellenbosch University Press, 1992. 14. Koshland DE Jr. Fetal tissue research. Science 1992; 256:1741. [PMID 1615314]
- Gibson A. Ethical considerations with regard to the sanctity of human life. South African Medical Journal 1998; 88:131-2.
- Rizvi SA. Ethical issues in transplantation. Transplant Proc 1999; 31:3269-70. [PMID 10616471]
- Page BJ, du Toit DF, Muller CJ, Mattysen J, Lyners R. An immunocytochemical profile of the endocrine pancreas using an occlusive duct ligation model. JOP. J Pancreas (Online) 2000; 1:191-203. [PMID 11856861]
- Brelje TC, Parsons JA, Sorenson RL. Regulation of islet beta-cell proliferation by prolactin in rat islets. Diabetes 1994; 43:263-73. [PMID 7904577]
- Scott RJ, Hall PA, Haldane JS, Van Noorden S, Price Y, Lane DP, Wright NA. A comparison of immunohistochemical markers of cell proliferation with experimentally determined growth fraction. J Pathol 1991; 165:173-8.
- Walker NI, Winterford CM, Kerr JF. Ultrastructure of the rat pancreas after experimental duct ligation, II. Duct and stromal cell proliferation, differentiation and deletion. Pancreas 1992; 7:420-34. [PMID 1641387]
- Walker NI. Ultrastructure of the rat pancreas after experimental duct ligation, I. The role of apoptosis and intraepithelial macrophages in acinar cell deletion. Am J Pathol 1987; 126:439-51. [PMID 3826300]
- Korsgren O, Jansson L, Eizirik D, Andersson A. Functional and morphological differentiation of fetal porcine islet-like clusters after transplantation into nude mice. Diabetologia 1991; 34:379-86. [PMID 1884897]
- Ferrannini E, Pilo A. Pattern of insulin delivery after intravenous glucose injection in man and its relation to plasma glucose disappearance. J Clin Invest 1979; 64:243-54. [PMID 447855]
- Thorell JI, Nosslin B, Sterky G. Estimation of early insulin response to intravenous glucose injection. J Lab Clin Med 1973; 82:101-10. [PMID 4717996]
- Vallerand AL, Frim J, Kavanagh MF. Plasma glucose and insulin responses to oral and intravenous glucose in cold-exposed humans. J Appl Physiol 1988; 65:2395-9. [PMID 3063707]
- Du Toit DF, Heydenrych JJ, Louw G, Zuurmond T, Laker L, Smit B, et al. Diabetes in pancreatectomized baboons: A model for pancreatic transplantation studies. J Surg Oncol 1987; 35:213-6. [PMID 3298861]
- Du Toit DF, Heydenrych JJ, Smit B, Louw G, Zuurmond T, Laker L, et al. Early postoperative pancreatic endocrine function after segmental and pancreaticoduodenal allotransplantation in nonimmunesuppressed primates. J Surg Oncol 1987; 34:272-7. [PMID 3550295]
- Cerasi E, Luft R. Plasma-insulin response to sustained hyperglycemia induced by glucose infusion in human subjects. Lancet 1963; 28:1359-61. [PMID 14071152]
- Kaneko JJ, Mattheeuws D, Rottiers RP, Vermeulen A. Renal function, insulin secretion, and glucose tolerance in mild streptozotocin diabetes in the dog. Am J Vet Res 1978; 39:807-9. [PMID 153115]
- Rosenberg L, Clas D, Duguid WP. Trophic stimulation of the ductal/islet cell axis: a new approach to the treatment of diabetes. Surgery 1990; 108:191-7. [PMID 2200154]
- Guesdon JL, Ternynck T, Avrameas S. The use of avidin-biotin interaction in immunoenzymatic techniques. J Histochem Cytochem 1979; 27:1131-9. [PMID 90074]
- Bouwens L, Lu WG, De Krijger R. Proliferation and differentiation in the human fetal endocrine pancreas. Diabetologia 1997; 40:398-404. [PMID 9112016]
- Louw J. The establishment of baseline parameters of the vervet monkey endocrine pancreas as a model to investigate possible therapies for diabetes. PhD Thesis. Bellville, South Africa: University of Western Cape Press, 1995.
- McEvoy RC, Hegre OD. Morphometric quantitation of the pancreatic insulin-, glucagon-, and somatostatin-positive cell populations in normal and alloxan-diabetic rats. Diabetes 1977; 26:1140-6. [PMID 338404]
- Marble A, Podansky S. Joslin?s Diabetes Mellitus. 12th edition. Philadelphia, PA, USA: Lee and Febiger, 1985.
- Marble A, Podansky S. Joslin’s Diabetes Mellitus. 12th edition. Philadelphia, PA, USA: Lee and Febiger, 1985.




