Keywords
pancreatitis; Erythrocyte Indices
Abbreviation
AP acute pancreatitis; AUC area under the curve; OF
organ failure; RDW red cell distribution width
INTRODUCTION
Acute pancreatitis (AP) is a disorder featured by local
and systemic inflammatory response, which is observed
clinically as a spectrum varying from a mild, self-limited
disorder to systemic inflammation, organ failure (OF)
and even mortality [1]. According to 2012 revised Atlanta
classification, severe AP has been redefined as AP with
persistent OF (OF lasts more than 48 hours) with a
mortality rate of 20-60% [2, 3, 4, 5, 6]. Early identification
of severe AP is fundamental for the determination of
therapeutic strategy and efficient management since
effective intervention could significantly decrease
morbidity and mortality of severe pancreatitis [7, 8].
Red cell distribution width (RDW) is a parameter
reflecting the size variability of peripheral erythrocytes.
It is one part of the complete blood count test. Elevated level of RDW represents greater heterogeneity of red
cells. Higher RDW values were strongly associated
with increased deaths from cardiovascular disease,
cancer and other causes in older adults [9], and allcause
mortality irrespective of nutritional deficiencies in
both middle-aged and older adults [10]. Elevated RDW level
was a predictor of mortality in patients with Gram-negative
bacteremia [11] and was significantly related with higher
rates of 90-day mortality and severe morbidity in young
patients with community acquired pneumonia [12]. RDW was an
independent predictor of 1-year mortality and re-hospitalization
in patients with acute decompensated heart failure [13], and 30-
day mortality in patients with acute dyspnea [14]. Increased
RDW was significantly associated with in-hospital-, ICU-, and
1-year mortality in unselected critically ill patients [15], and
an increase in RDW from baseline during the first 72 hours
after hospitalization is significantly associated with 28-day and
90-day mortality in patients with severe sepsis or septic shock
[16]. Moreover, two recent studies demonstrated that RDW was
predictive of mortality in AP [17, 18].
However, the association underlying RDW and
persistent OF in AP has not been fully elucidated yet.
MATERIALS AND METHODS
Patient Selection
We performed a retrospective study of AP patients
admitted to the department of Pancreatic Surgery in Union Hospital (Wuhan, China) between March 2016 and January
2017. Diagnosis of AP was made if one met with more than
2 of the following 3 criteria: 1) abdominal pain; 2) serum
lipase and/or serum amylase elevated more than 3 times
of the upper normal limit; 3) abdominal imaging including
computed tomography (CT) or magnetic resonance
imaging (MRI) shows AP characteristics [2]. The exclusion
criteria were as follows: 1) age smaller than 18 years; 2)
the time from symptom onset to hospital presentation ≥48
hours; 3) patients without CT or MRI scan; 4) patients with
insufficient clinical record; 5) trauma-induced pancreatitis;
6) chronic pancreatitis (Figure 1).
Figure 1. Flow diagram of patient selection.
AP acute pancreatitis; CT computed tomography; MRI magnetic radiologic imaging
Admission laboratory information were obtained from
the blood test results upon presentation. The automated
Coulter Counter Model S-Plus Jr (Coulter Electronics,
Hialeah, FL) was used to measure the value of RDW.
The medical records of patients were reviewed by one
independent physician for data on basic demographics, pre-existing comorbidities, and disease severity. The study
was conducted according to the Declaration of Helsinki
principles. Informed consent was waived because all of
the related data were acquired retrospectively from the
hospital recording system, thus no additional laboratory
assessments were needed. The study was approved by the
ethics review board of Union Hospital (Wuhan, China).
Definitions
Severity of AP was defined according to the 2012
revised Atlanta criteria [2]. OF was determined when the
following cutoffs were exceeded: 1) failure of respiratory
system when PaO2/FiO2 was less than 300 mmHg; 2)
failure of renal system when creatinine was ≥1.9 mg/
dl; and 3) failure of cardiovascular system when systolic
blood pressure was less than 90 mmHg despite fluid
resuscitation. When OF lasts ≥48 h, persistent OF was
identified. Pancreatic necrosis (PNec) was diagnosed if
contrast-enhanced computed tomography (CECT) showed non-enhanced area of pancreatic parenchymal and/or
peri-pancreatic part [2].
Statistical Analysis
Statistical analysis was conducted with SPSS 20.0
(Chicago IL, USA). Continuous data are presented as
median (interquartile range). Categorical variables are
reported as number (%). Mann-Whitney U and Student’s t tests were performed to assess the differences between
two study groups. Log-rank test was used for uni-variable
analysis. Parameters showing statistical significance in
uni-variable analysis were included in multi-variable
regression. Cox regression model was utilized for multivariable
analysis. Hazard ratios (HRs) and associated
95% confidence intervals (95% CIs) are shown. We used
receiver-operator characteristic (ROC) curves to evaluate
the predictive ability and its positive predictive value
(PPV), negative predictive value (NPV), sensitivity and
specificity of different parameters. P<0.05 was considered
as statistical significance.
RESULTS
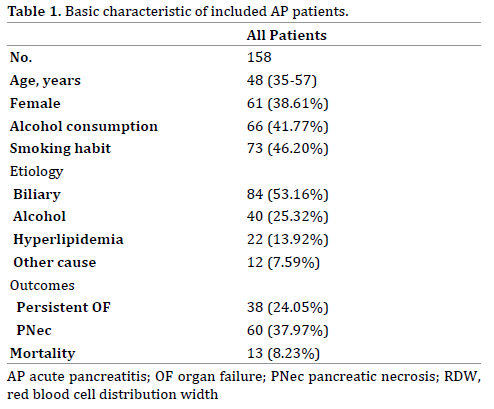
Patient Characteristics
A total of 158 AP patients admitted to our department
during the period were included in this study. Baseline
characteristics of these patients are presented in Table
1. The median age was 48 years and 61 (38.16%) of the
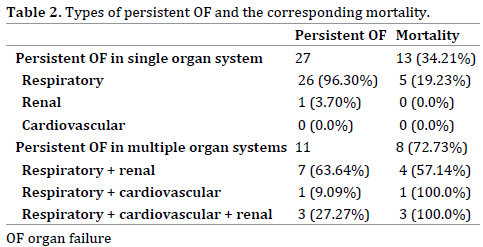
patients were females. Overall, 38 patients developed
persistent OF. 27 patients were identified as persistent
OF in single organ system. Multiple persistent OF was
observed in 11 patients (7 of the lung and the kidney, 1 of
the lung and the heart, and 3 of all three organs). During
hospitalization, 13 patients with POF died with an overall
mortality of 8.23%. No death was found in AP patients
without persistent OF (Table 2).
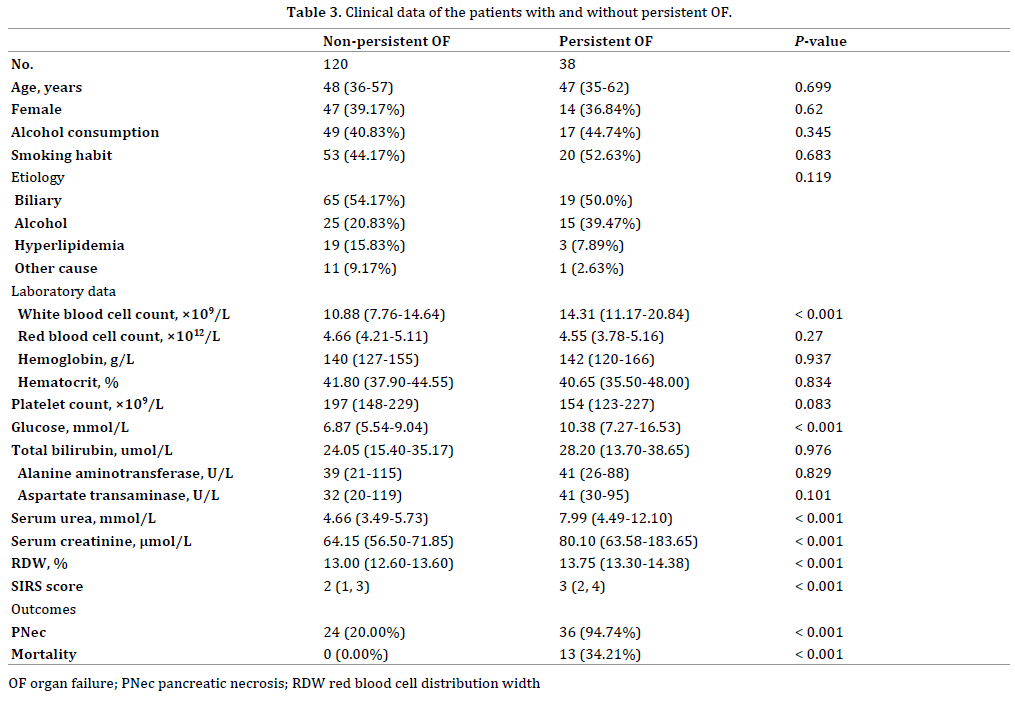
Comparison between Patients with and without
Persistent OF
The comparison of basic characteristics between the
two groups was shown in Table 3. Age, gender, smoking
and drinking habits, and disease etiology were not
different between patients with and without persistent
OF. The levels of white blood cell count, glucose, urea,
creatinine and RDW were statistically higher in patients
with POF. While the values of red blood cell count,
hemoglobin, hematocrit, platelet, total bilirubin, alanine
aminotransferase, and aspartate transaminase showed no
significant differences between the two groups. Moreover,
SIRS score on admission was significantly higher in
persistent OF ones.
Admission RDW as an Independent Predictor for
Persistent OF
In order to further investigate the association between
RDW and incidence of persistent OF, we used logistic
regression model. We included white blood cell count,
glucose, RDW and SIRS score in uni-variable analysis. The
results suggested they were all correlated significantly with the incidence of persistent OF. As white blood cell
count was included in SIRS score, we decided to exclude it
from multi-variable analysis. On multi-variable regression,
RDW and glucose were identified as independent
prognostic factors (HR: 2.26, 95%CI 1.46-3.51; P<0.001 for
RDW and HR: 1.18, 95%CI 1.06-1.32; P = 0.003) (Table 4).

As shown in Table 5, the area under curve of the receiver
operating characteristic (AUC) for prediction of POF was
0.791 (95%CI: 0.722-0.860) of RDW, which was superior to
that of glucose (0.737 [95%CI: 0.637- 0.837]) and SIRS score
(0.691 [95%CI: 0.607- 0.775]). RDW showed a sensitivity of
97.4%, specificity of 55.8%, PPV of 41.1%, and NPV of 98.5%.
The optimal threshold was 13.05 %.

DISCUSSION
In this study, we revealed that admission RDW was
an independent prognostic parameter of persistent OF
in patients with AP. Moreover, the predictive value was
superior to scores of SIRS and Ranson’s criteria.
Although a majority of patients with AP have a mild
course of the disease, severe forms of AP require more
attention because of its high morbidity and mortality.
Persistent OF, the most widely observed cause of mortality
within the first two weeks of disease onset, occures in
10-20% of AP patients, shows a mortality rate of 20
-50% [2, 3]. Early identification of AP patients at risk for
persistent OF is critical, both for triaging patients to the
appropriate grade of care and for designing relative clinical
intervention.
A wide range of methods such as biochemical variables,
radiological imaging modalities and clinical severity
scores have been used for predicting persistent OF in
AP [19]. Studies have compared the predictive ability of
several existing scoring systems, including SRIS, Ranson,
Glasgow, APACHE II and the Bedside Index of Severity in
Acute Pancreatitis (BISAP) score [20, 21, 22]. They found
that these scoring systems demonstrated modest accuracy
with an AUC ranging from 0.6 to 0.8 in both the training and
the validation cohorts. The authors figured out that these
scores seemed to have reached their maximal efficacy.
Recently, studies have shown that several parameters
were predictive of persistent OF in AP, including peripheral blood CD4+T lymphocytes [23], neutrophil to lymphocyte
ratio [24], lactate dehydrogenase [25], calcium [26], mean
platelet volume [27] and high density lipoprotein [28].
The role of RDW in AP has been explored in some
researches. A study by Şenol et al. [17] showed that elevated
level of admission RDW was an independent predictor of
mortality in AP. High RDW level (i.e., RDW >14.8%) upon
presentation functions better than conventional prognostic
markers for the prediction of mortality. Later, Wang et al. [18] demonstrated in their study that using RDW
>14.35% as a cut-off value, the sensitivity and specificity
for predicting deaths were 88.2% and 91.8%, respectively.
Another study [29] found that RDW was correlated with 48-hour Ranson score, but not associated with admission
Ranson score. However, the definition for OF was not
based on modified Marshall Score or SOFA score described
in 2012 Atlanta criteria [2].
Based on these studies mentioned above, we tried
to assess whether RDW could be useful to predict the
incidence of persistent OF (OF is classified according
to modified Marshall score mentioned in 2012 Atlanta
criteria) in AP. In our study, the incidence of persistent OF
was 24.05% (38/158) among all AP patients. Our results
suggested that RDW was an independent prognostic factor
of persistent OF in AP. Using RDWLDH ≥13.05% as a cutoff
value, the AUC for the prediction of persistent OF was
0.876, which was superior to the AUCs of glucose and SIRS
score. The RDW is a convenient and cheap laboratory test
that could be routinely utilized in clinical setting.
Several limitations are evident in the study. First,
due to the small number of our study population and
its retrospective nature, selection bias may influence
the generalization of our results. Second, as this is an
observational single-center study, the causality role
of RDW and persistent OF in AP, however, requires
to be investigated further in prospective multi-center
validation researches. Besides, we only examined one
time measurements. Therefore, this study did not address
the problem of intra-individual variation in RDW value.
Additional prospective data on consecutive patients are
urgently needed to confirm our findings.
The strengths of the present study are as follows: 1)
To our knowledge, this is the first detailed study exploring
the relationship between RDW and persistent OF in AP
using uni- and multi-variate logistic regression model. 2) Patients included were all admitted within 48 hours from
AP symptom onset and without any treatment before the
blood samples were collected. It is possible that therapeutic
manipulations may rapidly influence the value of RDW. 3) The
predictive value of RDW was compared with conventional
severity scores such as SIRS criteria (Figure 2).
Figure 2. Receiving operator curve analysis of RDW, glucose and SIRS score in predicting persistent OF.
OF organ failure; RDW red blood cell distribution width; SIRS systemic inflammatory response syndrome
CONCLUSION
In conclusion, our present study indicates that RDW
on admission is an independent prognostic factor for
persistent OF in AP. RDW may serve as a biomarker
of severity, and might be utilized together with other
predictors to form a new severity scoring system for AP.
Conflict of Interest Statement
The authors declare that they have no conflict of
interest.
References
- Oiva J, Mustonen H, Kylänpää ML, Kyhälä L, Kuuliala K, Siitonen S, et
al. Acute pancreatitis with organ dysfunction associates with abnormal
blood lymphocyte signaling: controlled laboratory study. Crit Care 2010;
14:R207. [PMID: 21087472]
- Banks PA, Bollen TL, Dervenis C, Gooszen HG, Johnson CD, Sarr MG,
et al. Classification of acute pancreatitis-2012: revision of the Atlanta
classification and definitions by international consensus. Gut 2013;
62:102–111. [PMID: 23100216]
- Nawaz H, Mounzer R, Yadav D, Yabes JG, Slivka A, Whitcomb DC, et
al. Revised Atlanta and determinant-based classification: application in
a prospective cohort of acute pancreatitis patients. Am J Gastroenterol
2013; 108:1911–1917. [PMID: 24126632]
- Johnson CD, Abu-Hilal M. Persistent organ failure during the first
week as a marker of fatal outcome in acute pancreatitis. Gut 2004;
53:1340–1344. [PMID: 15306596]
- Mofidi R, Duff MD, Wigmore SJ, Madhavan KK, Garden OJ, Parks RW.
Association between early systemic inflammatory response, severity of
multiorgan dysfunction and death in acute pancreatitis. Br J Surg 2006;
93:738–744. [PMID: 16671062]
- Lytras D, Manes K, Triantopoulou C, Paraskeva C, Delis S, Avgerinos
C, et al. Persistent early organ failure: defining the high-risk group of
patients with severe acute pancreatitis? Pancreas 2008; 36:249–254.
[PMID: 18362837]
- Eatock FC, Chong P, Menezes N, Murray L, McKay CJ, Carter CR, et
al. A randomized study of early nasogastric versus nasojejunal feeding in
severe acute pancreatitis. Am J Gastroenterol 2005; 100:432-439. [PMID:
15667504]
- Oría A, Cimmino D, Ocampo C, Silva W, Kohan G, Zandalazini
H, Szelagowski C, et al. Early endoscopic intervention versus early
conservative management in patients with acute gallstone pancreatitis
and biliopancreatic obstruction: a randomized clinical trial. Ann Surg
2007; 245:10-17. [PMID: 17197959]
- Patel KV, Semba RD, Ferrucci L. Red cell distribution width and
mortality in older adults: a meta-analysis. J Gerontol A Biol Sci Med Sci
2010; 65:258–65. [PMID: 19880817]
- Patel KV, Ferrucci L, Ershler WB, Longo DL, Guralnik JM. Red blood
cell distribution width and the risk of death in middle-aged and older
adults. Arch Intern Med 2009; 169:515–23. [PMID: 19273783]
- Ku NS, Kim HW, Oh HJ, Kim YC, Kim MH, Song JE, et al. Red blood
cell distribution width is an independent predictor of mortality in
patients with gram-negative bacteremia. Shock 2012; 38: 123–7. [PMID:
22683729]
- Braun E, Domany E, Kenig Y, Mazor Y, Makhoul BF, Azzam ZS.
Elevated red cell distribution width predicts poor outcome in young
patients with community acquired pneumonia. Crit Care 2011; 15:R194.
[PMID: 21835005]
- Makhoul BF, Khourieh A, Kaplan M, Bahouth F, Aronson D, Azzam
ZS. Relation between changes in red cell distribution width and clinical
outcomes in acute decompensated heart failure. Int J Cardiol 2012; 167:
1412-6. [PMID: 22560496]
- Hong N, Oh J, Kang SM, Kim SY, Won H, Youn JC, et al. Red blood
cell distribution width predicts early mortality in patients with acute
dyspnea. Clin Chim Acta 2012; 413:992–7. [PMID: 22406179]
- Hunziker S, Celi LA, Lee J, Howell MD. Red cell distribution width
improves the simplified acute physiology score for risk prediction
in unselected critically ill patients. Crit Care 2012; 16:R89. [PMID:
22607685]
- Kim CH, Park JT, Kim EJ, Han JH, Han JS, Choi JY, et al. An increase
in red blood cell distribution width from baseline predicts mortality in
patients with severe sepsis or septic shock. Crit Care 2013; 17:R282.
[PMID: 24321201]
- Senol K, Saylam B, Kocaay F, Tez M. Red cell distribution width as
a predictor of mortality in acute pancreatitis. Am J Emerg Med 2013;
31:687–9. [PMID: 23399348]
- Wang D, Yang J, Zhang J, Zhang S, Wang B, Wang R, et al. Red cell
distribution width predicts deaths in patients with acute pancreatitis. J
Res Med Sci 2015; 20:424–428. [PMID: 26487869]
- Moinzer R, Langmead CJ, Wu BU, Evans AC, Bishehsari F, Muddana V,
et al. Comparison of existing clinical scoring systems to predict persistent
organ failure in patients with acute pancreatitis. Gastroenterology 2012;
142:1476–82. [PMID: 22425589]
- Yang CJ, Chen J, Phillips AR, Windsor JA, Petrov MS. Predictors of
severe and critical acute pancreatitis: a systematic review. Dig Liver Dis
2014; 46:446–51. [PMID: 24646880]
- Gomatos IP, Xiaodong X, Ghaneh P, Halloran C, Raraty M, Lane B, et
al. Prognosticmarkers in acute pancreatitis. Expert Rev Mol Diagn 2014;
14:333–46. [PMID: 24649820]
- Mounzer R, Langmed CJ, Wu BU, Evans AC, Bishehsari F, Muddana V,
et al. Comparison of existing clinical scoring systems to predict persistent
organ failure in patients with acute pancreatitis. Gastroenterology 2012;
142:1476–82. [PMID: 22425589]
- Yang Z, Zhang Y, Dong L, Yang C, Gou S, Yin T, et al. The reduction of
peripheral blood CD4+ T cell indicates persistent organ failure in acute
pancreatitis. PLoS One 2015; 10:e0125529. [PMID: 25938229]
- Zhang Y, Wu W, Dong L, Yang C, Fan P, Wu H. Neutrophil to lymphocyte
ratio predicts persistent organ failure and in-hospital mortality in an
Asian Chinese population of acute pancreatitis. Medicine 2016; 95:37.
[PMID: 27631223]
- Cui J, Xiong J, Zhang Y, Peng T, Huang M, Lin Y, et al. Serum lactate
dehydrogenase is predictive of persistent organ failure in acute
pancreatitis. J Crit Care 2017; 41:161–165. [PMID: 28554094]
- Peng T, Peng X, Huang M, Cui J, Zhang Y, Wu H, et al. Serum calcium as
an indicator of persistent organ failure in acute pancreatitis. Am J Emerg
Med 2017; 35:978-982. [PMID: 28291705]
- Huang P, Zhang Y, Wu H. Mean platelet volume as an indicator of
persistent organ failure in acute pancreatitis. Int J Clin Exp Pathol 2016;
9:12883–12889.
- Zhang Y, Guo F, Li S, Wang F, Meng Z, Zhao J, et al. Decreased high
density lipoprotein cholesterol is an independent predictor for persistent
organ failure, pancreatic necrosis and mortality in acute pancreatitis. Sci
Rep 2017; 7:8064. [PMID: 28808236]
- Kilic M, Celik C, Yuksel C, Yıldız BD, Tez M. Correlation between
Ranson score and red cell distribution width in acute pancreatitis. Ulus
Travma Acil Cerrahi Derg 2017; 23:112-116. [PMID: 28467576]



